
Pulmonary Edema
The Common vein
Copyright 2009
Definition
Pulmonary edema is a circulatory abnormality of the pulmonary circulation with multiple causes, but most commonly due to left ventricular failure and resulting in the accumulation of fluid in the interstitium and alveoli of the lungs .
Clinically it results in shortness of breath, coughing, coughing up blood, breathing difficulty, wheezing, sweating, skin paleness, nasal flaring, and behavioral problems.
It is diagnosed clinically by observation, listening to respiratory sounds, oxygen level measurement, chest x-ray, and ultrasound.
Treatment includes the administration of oxygen, diuretic and cardiac support and if severe may require intubation, and ventilatory support.
Acknowledgment webpath.med.utah.edu
{kind=link}
42076c04-1-scaled.jpg
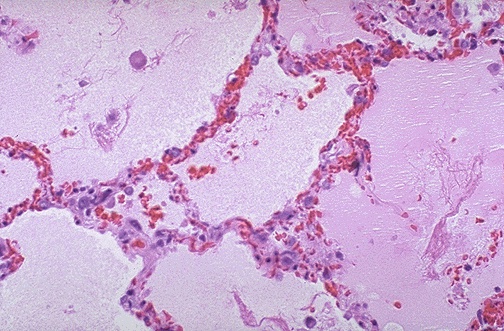
Normal vs Alveolar EdemaAshley Davidoff MD TheCommonVein.net
42076c04
TAKOTSUBO CARDIOMYOPATHY
74-year-old male with type 2 diabetes, CAD s/p stent 6 years prior, hypertension and hypercholesterolemia, fell at home and presents to the ER.
A CXR performed 4 years before, showed no acute cardiopulmonary disease. Healed right sided rib fractures and healed right clavicular fracture were of incidental note
In the ER a non-displaced right hip fracture was identified and uncomplicated hemiarthroplasty was performed.
CXR at the time showed no acute disease
He was discharged and in the interim prior to readmission 2 weeks later his wife fell and had to be admitted to the hospital.
At the time of his next readmission he presented in shock. (NYHA Class IV and ASA Class 4)
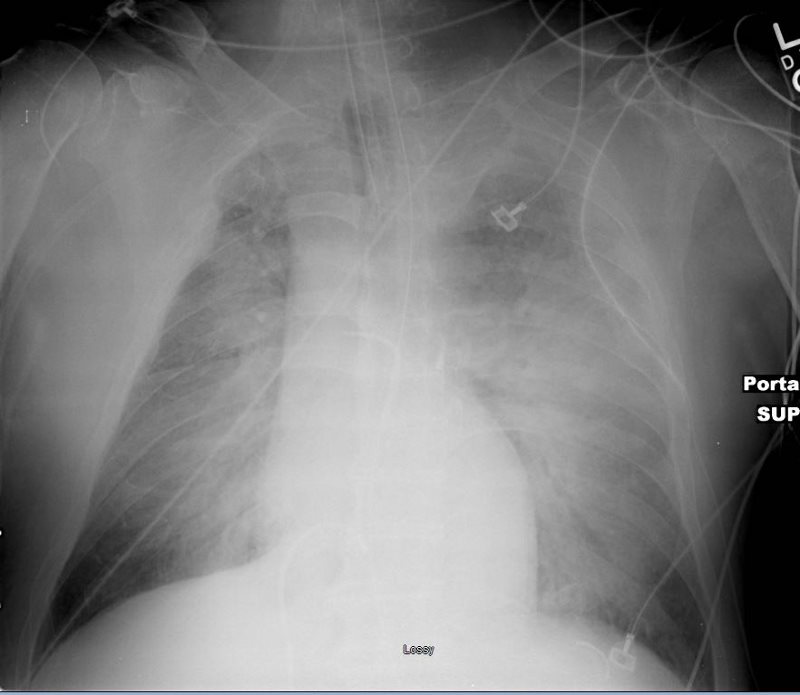
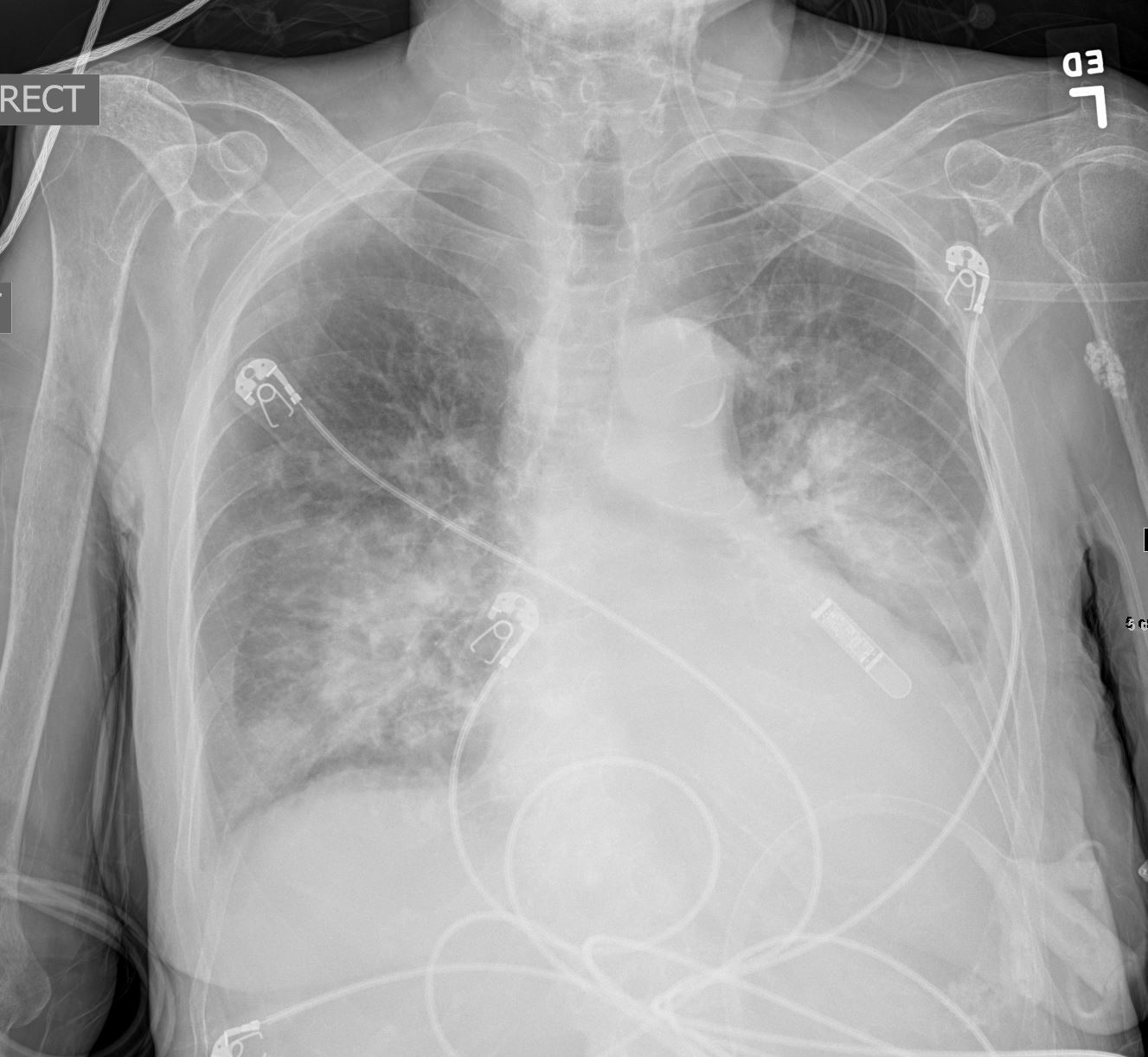
CXR showed pulmonary edema.
EKG showed new LBB
Echo at the bedside in the ICU showed an ejection fraction of 15%, with global hypokinesis sparing the base of the heart. There was moderate MR, PAP 44-65mm Hg, RV was normal.
Preliminary diagnosis of an acute MI was made with acute systolic heart failure and cardiogenic shock.
He was transferred to the cath lab for evaluation.
Prior to gaining access to the arterial system the patient went into PEA requiring sustained CPR requiring both epinephrine, atropine and urgent intubation
Emergent cardiac catheterization showed an LV pressure of 64/17 and wedge pressure of 41 mmHg. Temporary pacemaker was placed as well as an IABP. No significant CAD was identified. LV gram showed ballooning of the apex of the heart consistent with Takotsubo cardiomyopathy with an estimated ejection fraction of 10%
Serial CXR showed ongoing perihilar infiltrates with air bronchograms consistent with cardiogenic and alveolar edema. He passed away 2 days later
Ashley Davidoff MD
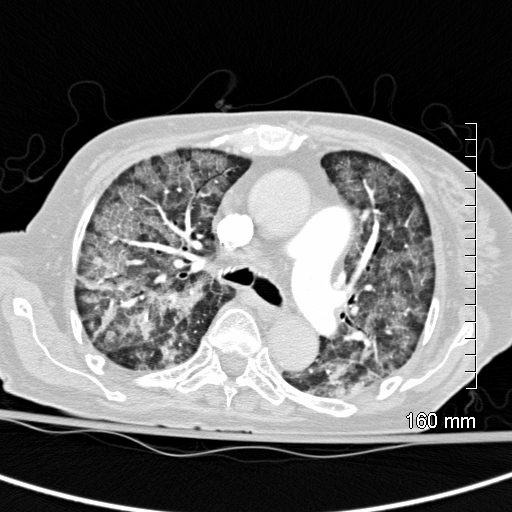
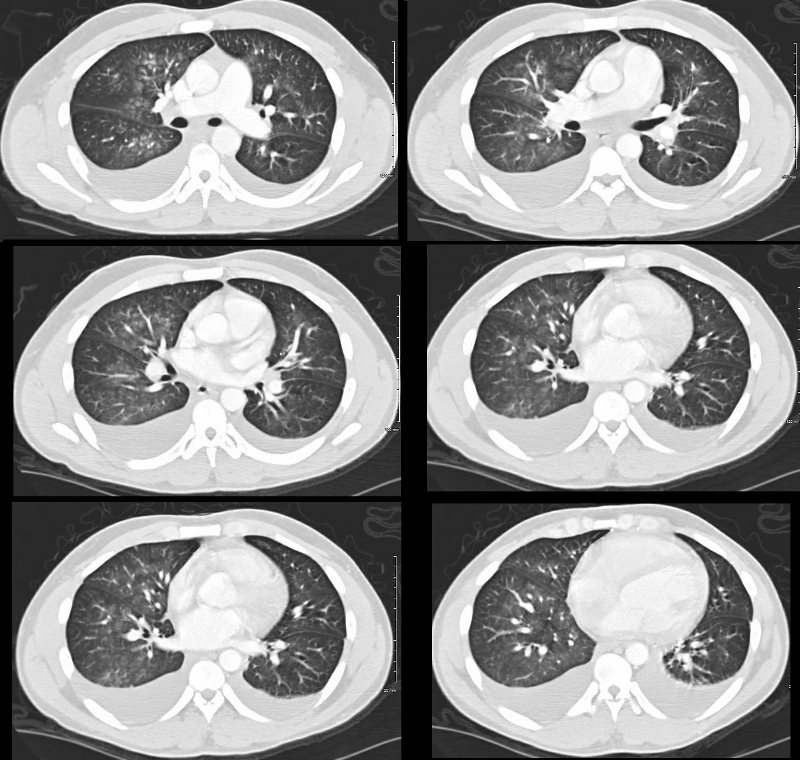
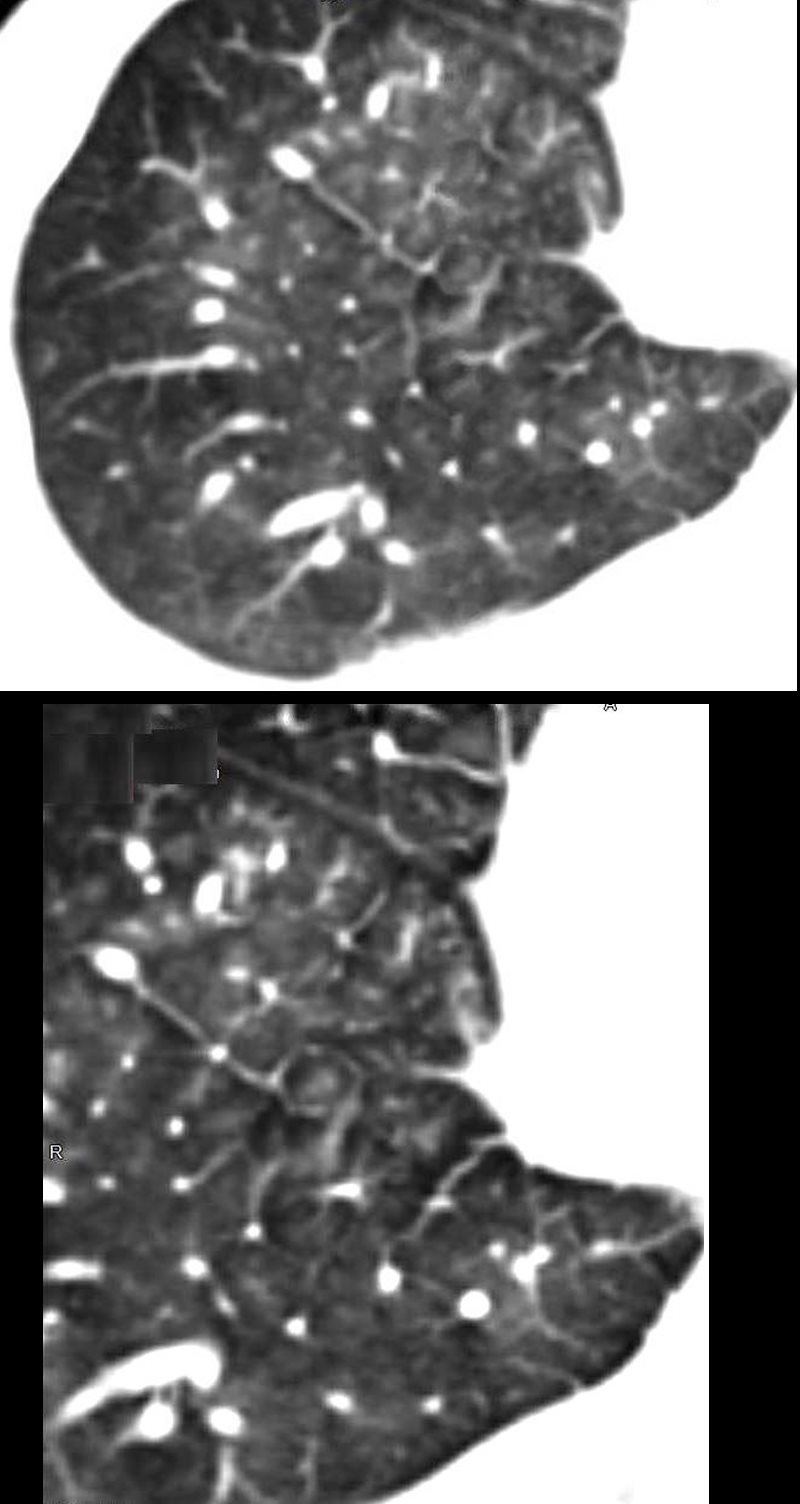
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD
Acknowledgment Hellerhoff – Wiki
Ashley Davidoff MD
TheCommonVein.net
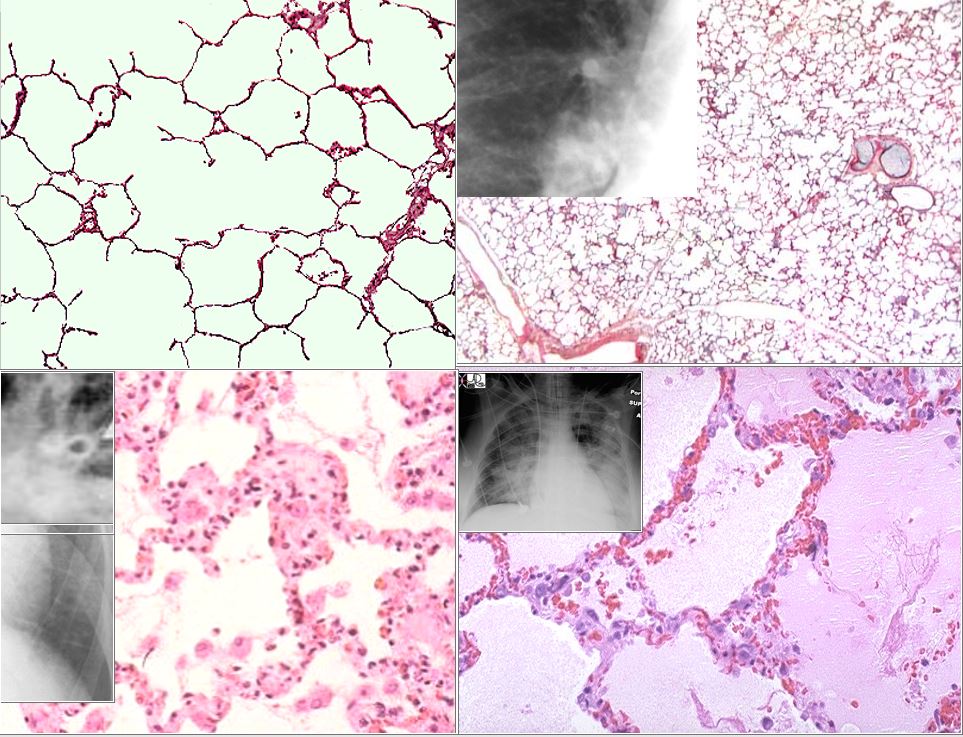
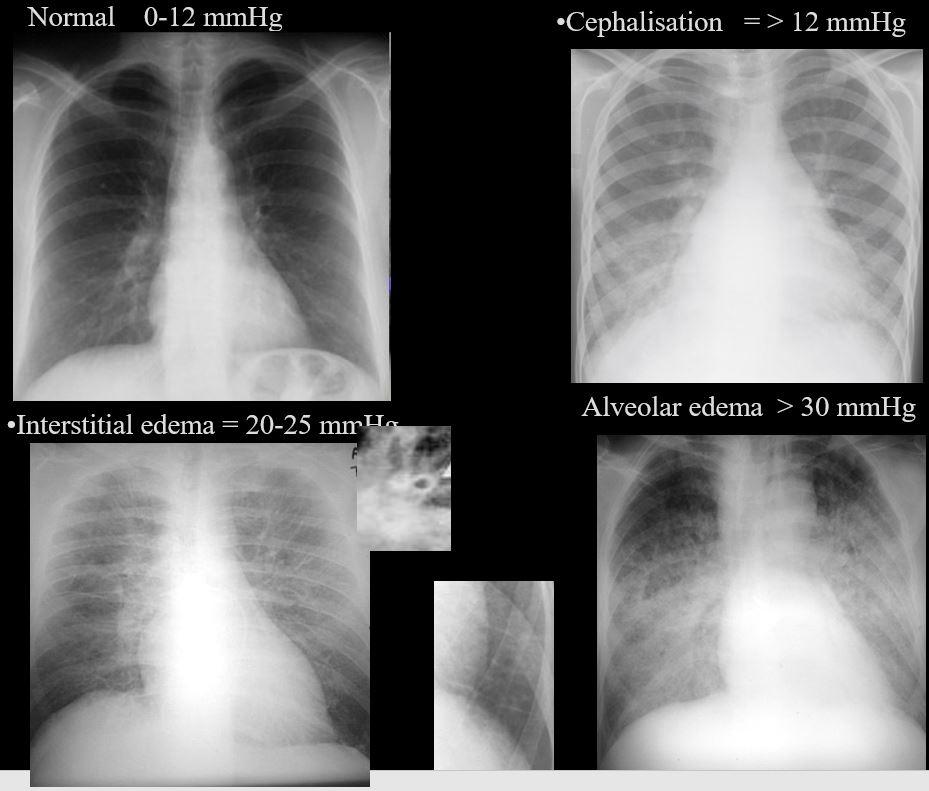
The top left image is the a histological section of normal alveoli and normal wall and interstitium. Heart failure occurs when the left ventricular end diastolic pressure rises. There are 3 basic phases of heart failure. in the first phase (top right) the LVEDP rises above 12 mmHg and on an upright CXR there is equalization of the size of the vessels going to the upper lobes and lower lobes. As the LVEDP goes above about 15-18 mm Hg there is cephalization of the vessels and the upper lobe vessels are larger than the lower lobe vessels.
The second phase of interstitial edema (bottom left) occurs when the intravascular hydrostatic pressure exceeds the intravascular oncotic pressure and this occurs when the LVEDP goes above 25 mm Hg. Fluid accumulates in the alveolar walls and interstitium and the wall becomes thicker with fluid, and the lymphatics and interlobular septa are distended.
The last phase of alveolar edema (lower right) occurs when the pressure exceeds 35 mmHg and the fluid leaks into the alveoli .
Ashley Davidoff MD
Cardiogenic Shock
Other Examples

34-year-old male has a normal appearing CXR 1 year before presentation
At the time of his first presentation with dyspnea his CXR showed perihilar infiltrates.
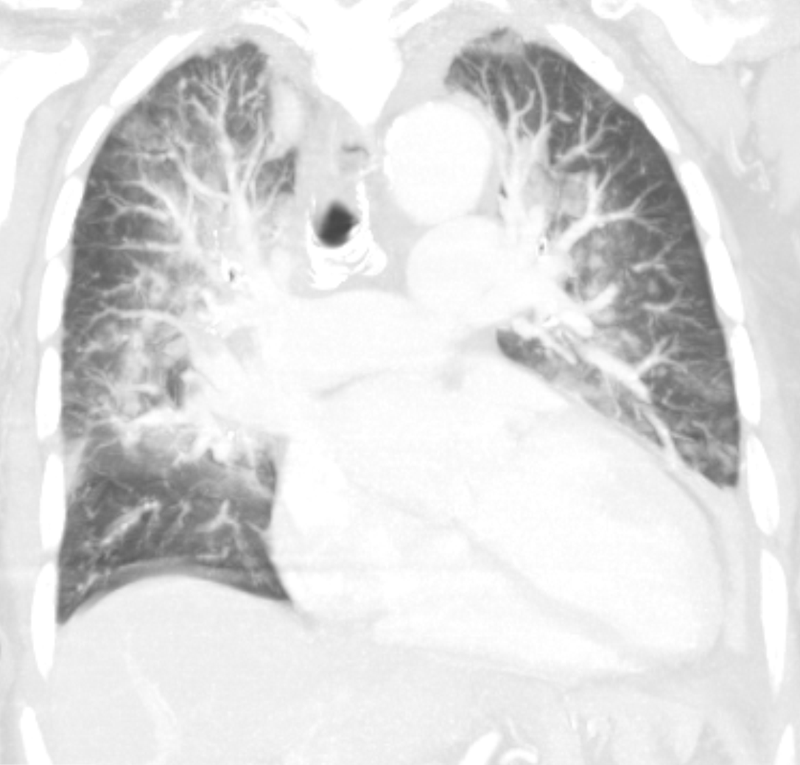
A CT confirmed progressive alveolar edema, with bilateral effusions (right greater than left), mild left ventricular dilatation, Kerley B lines and centrilobular densities and small pericardial effusion.
1 month after this admission a treadmill stress and rest gated SPECT study showed no evidence of ischemia with a calculated ejection fraction of 31%
A repeat CXR showed classical findings of left ventricular dilatation and left atrial enlargement but without CHF
Ct showed early coronary calcification, LAE, LVE and resolution of the pericardial effusion with pulmonary hypertension. Lungs were clear.
MRI confirmed the presence of a dilated cardiomyopathy, small pericardial effusion, without evidence of LGE, global hypokinesis and EF of about 20%
2 years later he presented with acute hemorrhagic pancreatitis that was felt to be related to his CRF
Serial CXRs over 3-4 days showed CHF with cephalization and early interstitial edema.
Echo showed improved LV function with EF of 50%, normal PAP, normal sized chambers, improved since the study performed 2 years earlier.
Repeat CT of the abdomen showed maturing pancreatic pseudocysts, mildly dilated LA, calcified medium sized vessels and calcification of the vasa deferentia
Ashley Davidoff MD
Ashley Davidoff MD
S/P Cardiac Arrest and ROSC with CXR evidence of Central Alveolar Edema
Alveolar Edema in a Patient with Dilated Cardiomyopathy, Diabetes, Chronic Renal Failure , Pancreatitis

Ashley Davidoff MD
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
Pulmonary Edema, Thickened Interlobular Septa and Crazy Paving
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD