

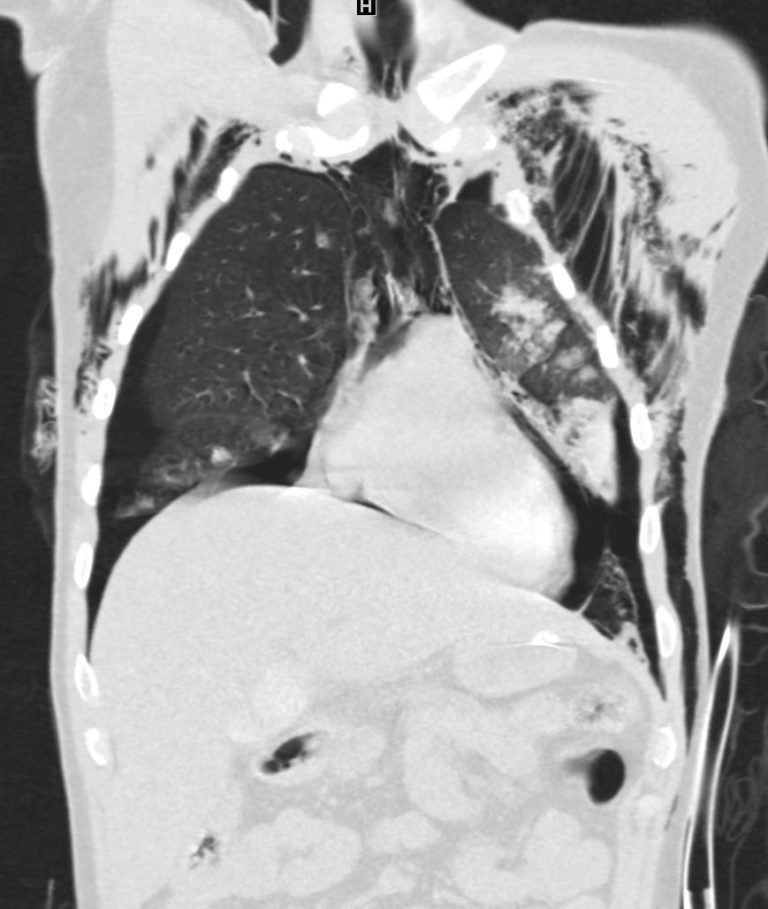
CT of a 31 year old male involved in a MVA with extensive trauma to the chest including bilateral pneumothoraces, pneumopericardium, lung contusion and significant consolidation, possibly hemorrhagic, and multiple sternal fractures
Ashley Davidoff MD
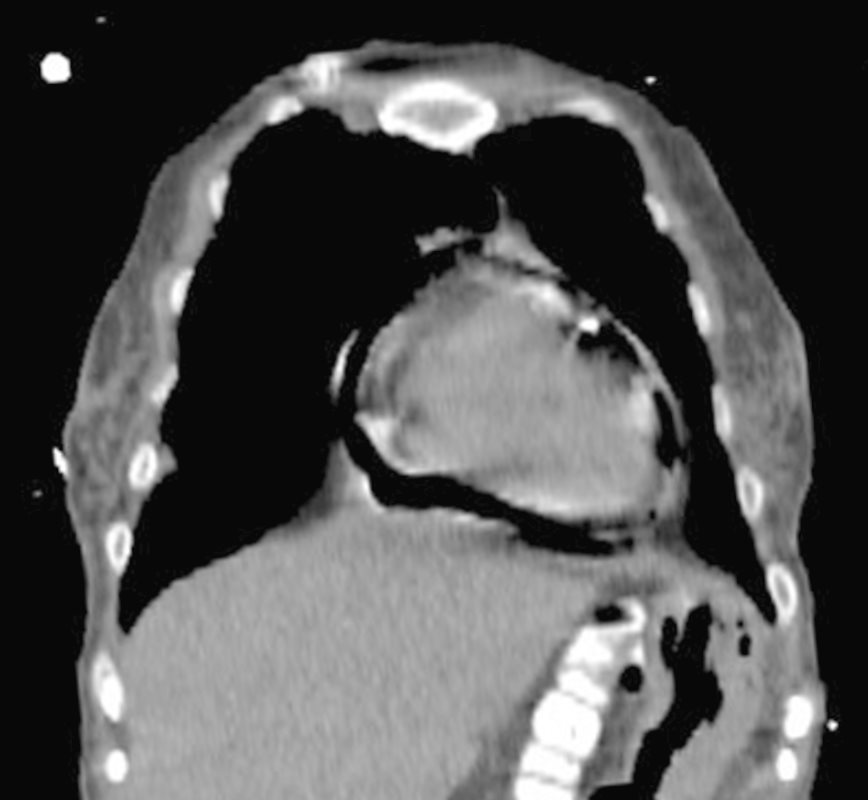
CT of a 31 year old male involved in a MVA with extensive trauma to the chest including bilateral pneumothoraces, pneumopericardium, lung contusion and significant consolidation, possibly hemorrhagic, and multiple sternal fractures
Ashley Davidoff MD

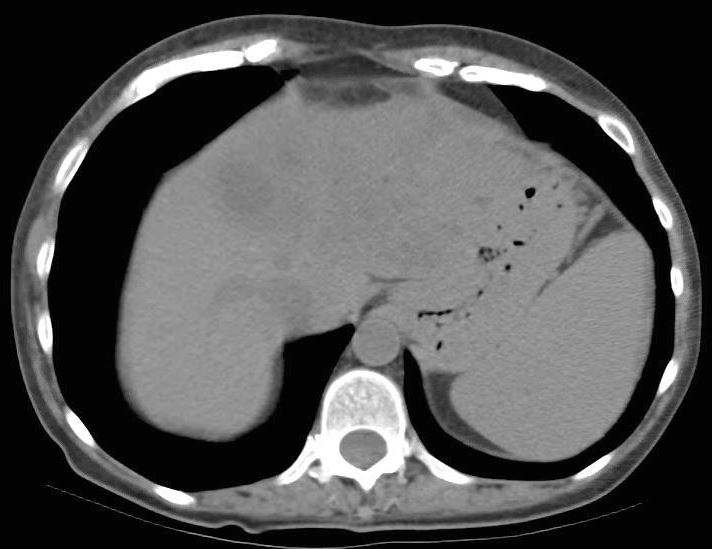
CT of a 31 year old male involved in a MVA with extensive trauma to the chest including bilateral pneumothoraces, pneumopericardium, lung contusion and significant consolidation, possibly hemorrhagic, and multiple sternal fractures
Ashley Davidoff MD

51 year old female with a history of chronic pancreatitis , pancreatic cancer s/p Whipple who presented with pericardial tamponade with PEA and emergent echo showed moderate pericardial effusion, and an EF of 20%, requiring emergent placement of a pericardial catheter. The effusion was purulent growing E Coli
CT scan showed a probable abscess in the dome of the liver and obstructed left bile ducts likely from recurrence
Patient subsequently expired
Ashley Davidoff MD

51 year old female with a history of chronic pancreatitis , pancreatic cancer s/p Whipple who presented with pericardial tamponade with PEA and emergent echo showed moderate pericardial effusion, and an EF of 20%, requiring emergent placement of a pericardial catheter. The effusion was purulent growing E Coli
CT scan showed a probable abscess in the dome of the liver and obstructed left bile ducts likely from recurrence
Patient subsequently expired
Ashley Davidoff MD

51 year old female with a history of chronic pancreatitis , pancreatic cancer s/p Whipple who presented with pericardial tamponade with PEA and emergent echo showed moderate pericardial effusion, and an EF of 20%, requiring emergent placement of a pericardial catheter. The effusion was purulent growing E Coli
CT scan showed a probable abscess in the dome of the liver and obstructed left bile ducts likely from recurrence
Patient subsequently expired
Ashley Davidoff MD
51 year old female with a history of chronic pancreatitis , pancreatic cancer s/p Whipple who presented with pericardial tamponade with PEA and emergent echo showed moderate pericardial effusion, and an EF of 20%, requiring emergent placement of a pericardial catheter. The effusion was purulent growing E Coli
CT scan showed a probable abscess in the dome of the liver and obstructed left bile ducts likely from recurrence
Patient subsequently expired
Ashley Davidoff MD
LIVER ABSCESS ? INCITING CAUSE
51 year old female with a history of chronic pancreatitis , pancreatic cancer s/p Whipple who presented with pericardial tamponade with PEA and emergent echo showed moderate pericardial effusion, and an EF of 20%, requiring emergent placement of a pericardial catheter. The effusion was purulent growing E Coli
CT scan showed a probable abscess in the dome of the liver and obstructed left bile ducts likely from recurrence
Patient subsequently expired
Ashley Davidoff MD
References and Links
Garcia et al Purulent Pericarditis after Liver Abscess: A Case Report
Case Rep Med. 2014; 2014: 735478.
Shorr et al Annals of Surgery Blunt Thoracic Trauma