
The Common Vein
Ashley Davidoff
Copyright 2019
Buzz
less than 2 mm
smooth
Although the pericardium is visible over the right atrium and right ventricle in most individuals, it often is not visible over the lateral and posterior walls of the left ventricle.
The parietal and visceral layers are separated by a small amount of serous fluid?normally, about 15?50 mL
The left atrium is only partially covered by the pericardium; it has been suggested that this anatomic feature may contribute to the left atrial enlargement seen in patients with constrictive pericarditis

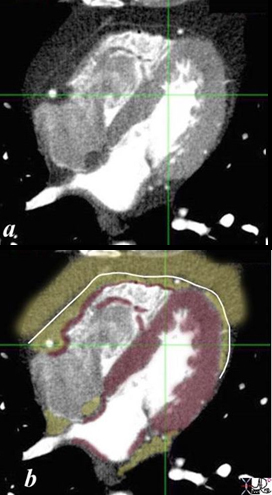
The coronal CTscan of the heart and the pericardium shows the inner visceral pericardium (pink) and the outer parietal or somatic pericardium (green) . The pleural components have similar morphological distribution. The lungs are surrounded by an inner visceral pleural layer (pink) and an outer parietal layer (green). Note how the pericardium extends superiorly to the region of the ascending aorta.
The visceral pericardium is in intimate contact with the outer surface of the heart and is derived from the splanchnic mesoderm. The parietal pericardium lining the outer portion of the heart is derived from somatic mesoderm.
This intent of this image is also to demonstrate the distribution of visceral and somatic (parietal) nociceptors in the chest. The visceral layers are shown in pink and the somatic layers are shown in green. The skin (green) is derived from somatic mesoderm and contains a large variety and number of nociceptors, as does the outer parietal pleura (green) and parietal pericardium (green) around the contrast-filled heart.
The parietal or somatic linings of the lungs and the heart (outer linings (green) are heavily endowed with nociceptors, while the visceral linings of the lung and the heart have fewer nociceptors both in number and type. The organs themselves have even less nociceptors.
The somatic and visceral linings of the organs of the upper abdomen follow the same pattern.
Ashley Davidoff MD 2019
82950c07b01.8s
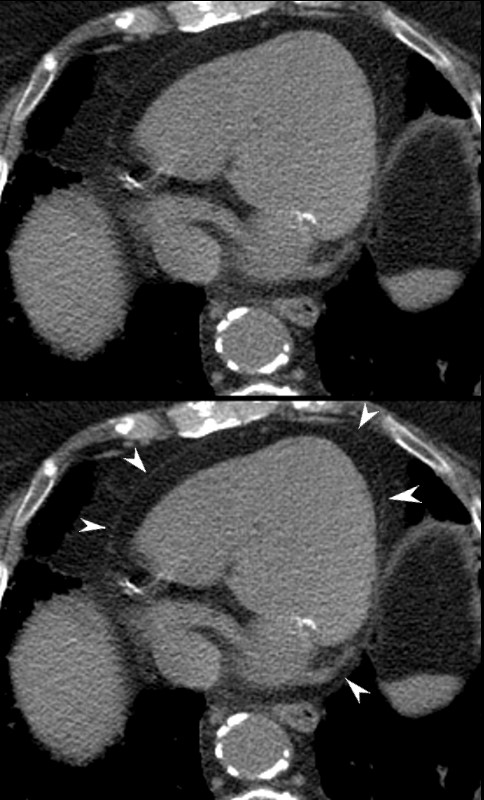
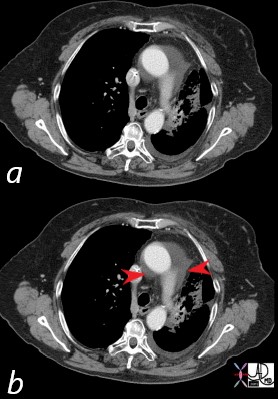
Non contrast CT through the base of the heart shows a normal, barely perceptible pericardium (white arrowheads in lower image), surrounded by epicardial and pericardial fat.
Ashley Davidoff MD
measuring 2.3 mm. A small amount of physiological pericardial fluid is noted posteriorly (red arrowhead)
Ashley Davidoff MD
Recesses and Sinuses
Superior Pericardial Recess
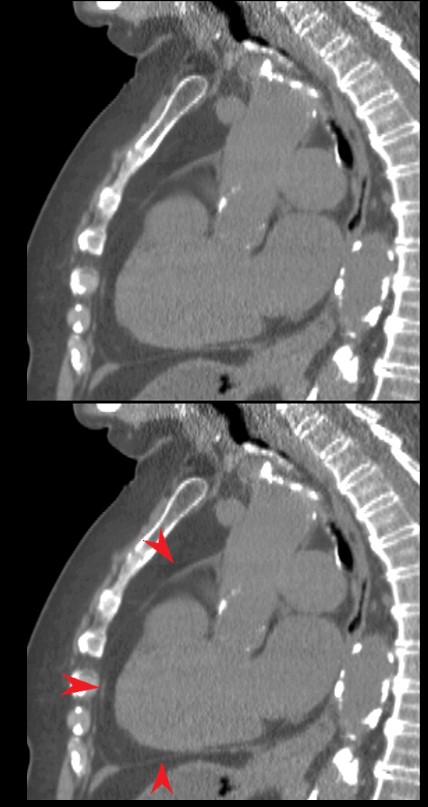
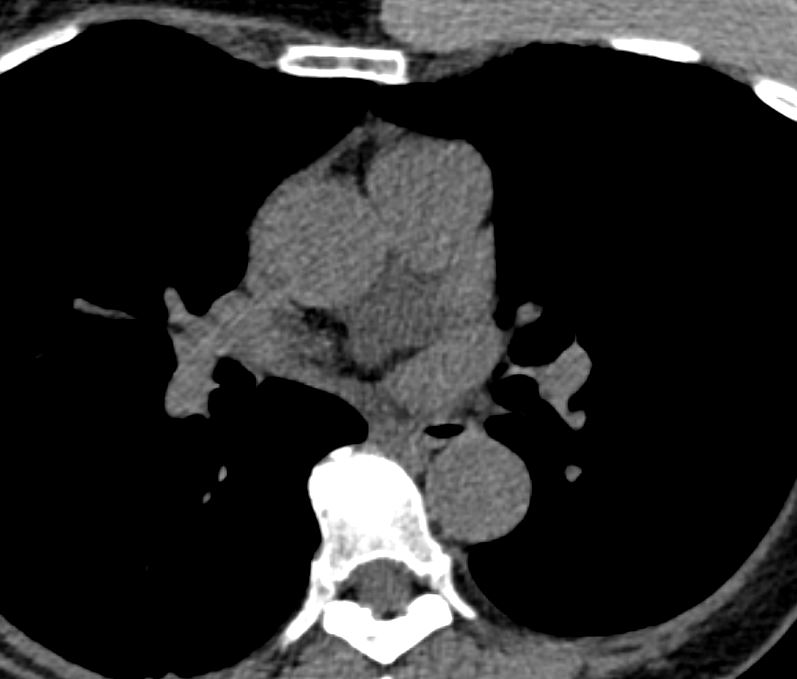
76 year old female with chest pain and SOB with XRT(radiation changes along the left side of the mediastimum demonstrates extension of a pericardial effusion to the superior aspect of the insertion. The superior recess red arrowheads) is noted posterior to the aorta and pulmonary artery
key words
heart, pericardium, superior recess, pericardial effusion,
moderate
dx pericarditis imaging radiology CTscan
Ashley Davidoff 2019
43707

Ashley Davidoff MD TheCommonVein.net

Ashley Davidoff MD TheCommonVein.net

{kind=link}
{kind=link}
Oblique pericardial sinus betweeen the superior pulmonary veins
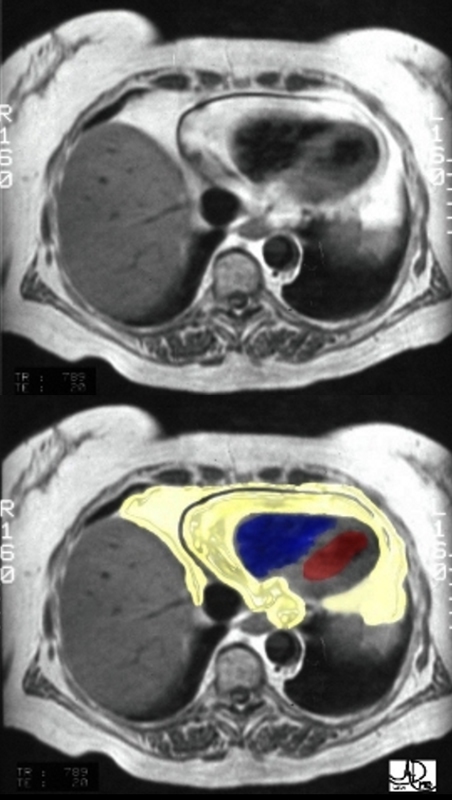
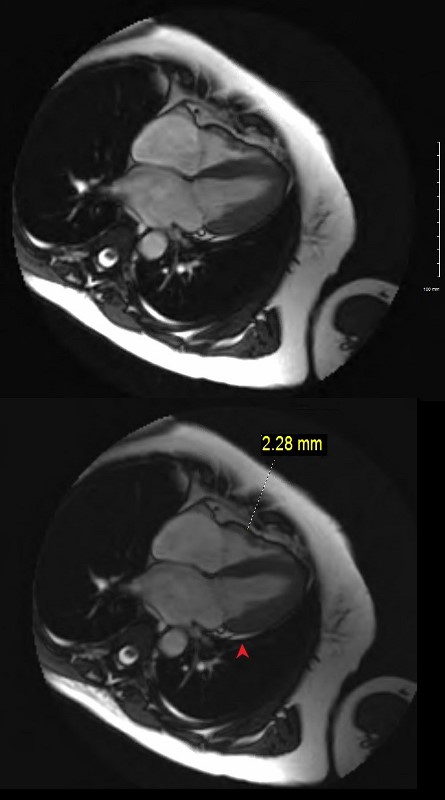
An axial T1 weighted MRI shows a large amount of fat (yellow overlay) around the heart. The epicardial fat is the inner layer and is intimately related to the heart and the pericardial fat is the outer layer. The normal pericardium is seen as a black line between the two layers of fat. Although the pericardium looks like a single layer, it actually consists of two structures – the epicardial serous component and the pericaricardial fibrous component. In pericardial effusion the two layers are separated.
The amount of fat is more than expected and this amount is often associated with Syndrome X.
Courtesy of Ashley Davidoff M.D. 32141.8 code normal heart epicardial fat pericardium anatomy cardiac imaging radiology MRI
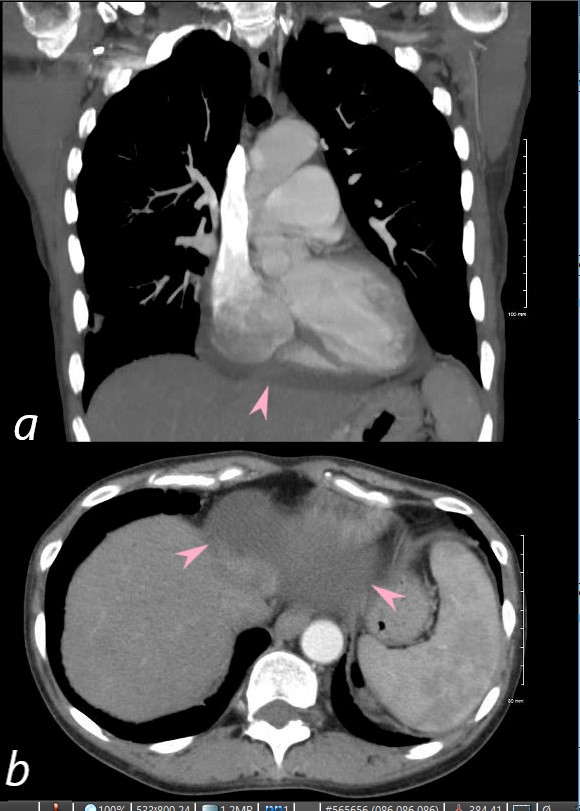
Coronal (a) and axial (b) CT images reveal the pericardial space below the heart in the region of the central tendon of the diaphragm (pink arrows in a and b).
The patient is a 54 year old female with SLE and Sjogren’s syndrome.
Ashley Davidoff MD
key words SLE, pericarditis, pericardial effusion
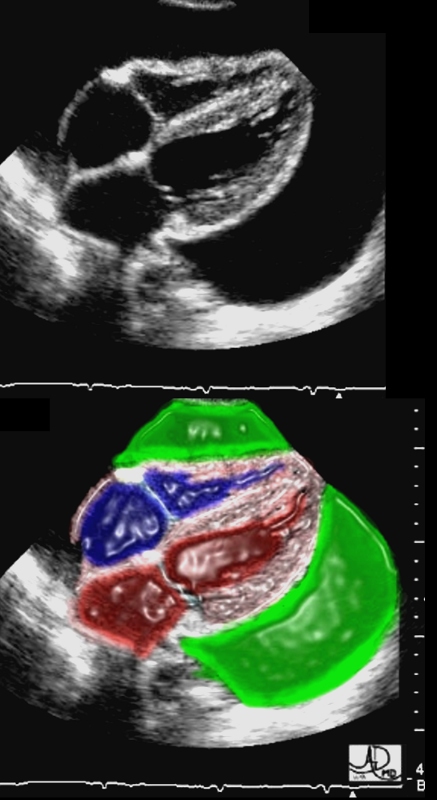
This four chamber echocardiogram shows a large pericardial effusion. (green overlay). The right ventricular (RV) lateral wall has slight inward bowing, but the septum has a normal shape.
Ashley Davidoff M.D.
32142.8
Pericarditis
{kind=link}
54-F-sarcoidosis-pericardial-effusion.8.jpg
NODULAR MULTICENTRIC LGE- SARCOIDOSIS AND PERICARDITIS54 year old female with a history of sarcoidosis diagnosed on a groin node biopsy. History of recurrent pericarditis with tamponade s/p pericardial window
MRIs performed 4 months apart reveal vague nodular changes at the hinge points and in the inferolateral portions of the left ventricle. In the first short axis scan the changes were thought to be artifact. However on follow up the finding are persistent and therefore real.
On both scans there is diffuse enhancement of the pericardium.
Courtesy Ashley Davidoff MD
34800c01 cardiac heart pericardium fx lucent subcarinal angle altered dx lipoma of pericardium fat CTscan plain film scout Davidoff MD
Definition
The heart and the base of the great vessels of the heart are contained in a fibroserous sac called the pericardium. Although the pericardium is usually described as a single sac, it actually consists of two sacs intimately connected with one another, but totally different in structure.
The Outer Sac- Parietal Pericardium
The outer sac, the fibrous pericardium, consists of fibrous tissue. The fibrous pericardium is attached at its base to the central tendon and to the muscular fibers of the left side of the diaphragm. It is also attached to the posterior surface of the sternum by the superior and inferior sternopericardial ligaments.
The Inner Sac – Visceral Pericardium
The inner sac, serous pericardium, is a delicate membrane composed of a single layer of flattened cells resting on loose connective tissue. The pericardial space with pericardial fluid separates the two layers. The visceral portion, or epicardium, covers the left ventricle and is continuous with the parietal layer which lines the fibrous pericardium.
Function
The function of the heart coverings are to provide protection against friction. The outer sac (fibrous pericardium) consists of fibrous tissue. The inner sac (serous pericardium) lies within the fibrous sac. It is composed of a single layer of flattened cells resting on loose connective tissue. The space between these two sacs is merely a potential one. The serous pericardium consists of a visceral and a parietal portion. The heart and the base of the great vessels of the heart are contained in a fibroserous sac called the pericardium. Although the pericardium is usually described as a single sac, it actually consists of two sacs intimately connected with one another, but totally different in structure. The outer sac, the fibrous pericardium, consists of fibrous tissue. The inner sac, serous pericardium, is a delicate membrane composed of a single layer of flattened cells resting on loose connective tissue. The pericardial space with pericardial fluid separates the two layers. The function of the heart coverings are to provide protection against friction. Functionally although the intact pericardium is not essential, several functions have been attributed to it (1)limitation of intrathoracic heart movement (2)balancing right and left ventricular outputs through diastolic and systolic interactions (3) minimize friction between cardiac chambers and surrounding structures and (4)limitation of acute dilatation of the heart.
The pericardial space with pericardial fluid separates the two layers.
Diseases of the pericardium are not uncommon and include acute pericarditis, chronic pericarditis, constrictive pericarditis and cardiac tamponade to name a few.
Diagnosis of pericardial diseases may be suspected in patients presenting with chest pain, fever and signs of heart failure. On examination pulsus paradoxus may be appreciated, jugular veins may be distended with abnormal venous wave forms, heart sounds may be distant, a pericardial knock, or pathognomonic triphasic scratching sound of pericardial rub may be heard. Chest radiography may show an enlarged cardiac silhouette in cardiac tamponade with calcification in chronic pericarditis. EKG may show characteristic changes in pericarditis which global ST elevation and absent Q waves. Trans thoracic echo is useful to identify cardiac tamponade . CT may be indicated in cases of constrictive pericarditis.MRI may be superior to CT in identifying pericardial effusion . Cardiac catheterization is helpful in understanding the hemodynamics.
Medical therapy and surgical options are available depending on the disease process in question.
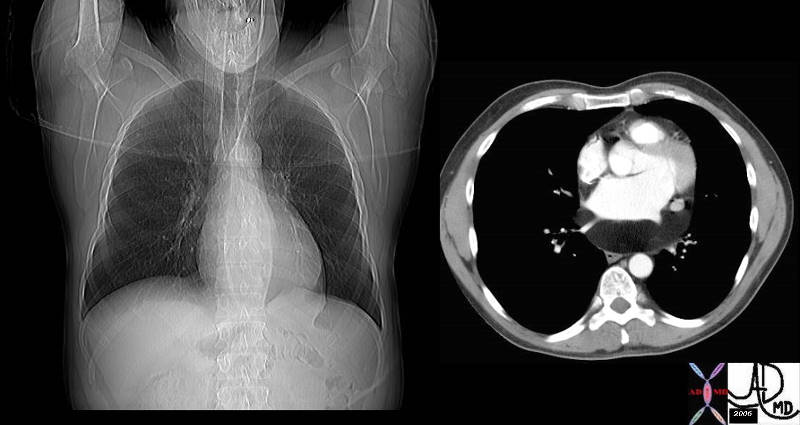
 Lipoma of the Pericardium Lipoma of the Pericardium |
| 34800c01 cardiac heart pericardium fx lucent subcarinal angle altered dx lipoma of pericardium fat CTscan plain film scout Davidoff MD |
Invasion of Pericardium and Pericardial Fat by Mesothelioma
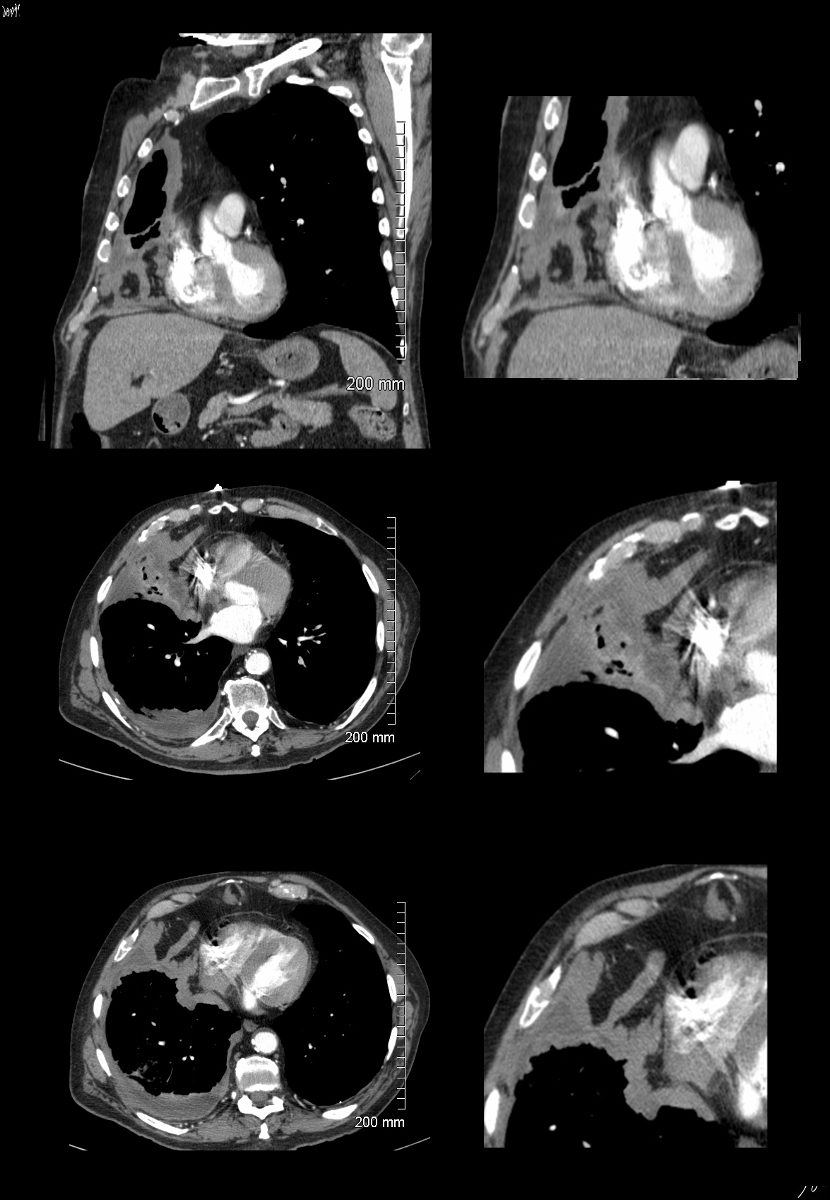
Ashley Davidoff MD TheCommonVein.net
pleura mesothelioma 0028c01
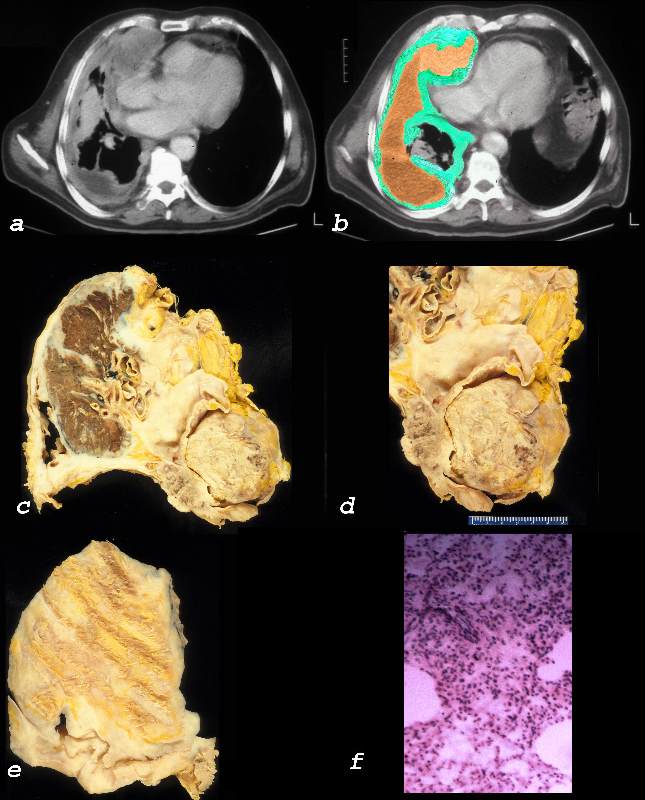
Ashley Davidoff MD TheCommonVein.net 32640c01L01.8
Pericardium
The heart and the base of the great vessels of the heart are contained in a fibro-serous sac called the pericardium. Although the pericardium is usually described structurally as a single sac, it actually consists of two sacs intimately connected with one another, but totally different in structure1. The outer sac, the fibrous pericardium, consists of fibrous tissue. The inner sac, serous pericardium, is a delicate membrane composed of a single layer of flattened cells resting on loose connective tissue.
Structural Considerations:
The pericardium lies in the middle mediastinum posterior to the sternum and 2nd to 6th costal cartilages and anterior to 5th to eight vertebrae. It is a fibro serous sac that invest the heart and great vessels and is composed of two layers(1) Outer tough fibrous pericardium which blends with the central tendon of the diaphragm and (2) serous pericardium which has a parietal (lines the inner surface of the fibrous pericardium) and visceral layer (lines the external surface of the heart and great vessels) .
The attachments of the fibrous pericardium to neighboring structures limit excessive intrathorcic cardiac motion. The fibrous pericardium is fastened1 (1) above with the tunica adventitia of the great vessels and the pretracheal layer of the deep cervical fascia (2) anteriorly to the posterior surface of the sternum by the sternopericardial ligaments (3) inferiorly it blends with the central tendon of the diaphragm and (4)posteriorly it is bound by loose connective tissue to structures in the posterior mediastinum.
The serous pericardium encloses a potential space between the visceral and parietal layers called the pericardial space. This space usually contains 15- 50 ml of pale serous fluid and serves to minimize friction between cardiac chambers and surrounding structures2.
The reflection of the visceral pericardium over the cardiac chambers and surrounding great vessels forms the pericardial sinuses(transverse and oblique) and recesses in the pericardial space4. The transverse pericardial sinus is a passage in the pericardial sac that lies just above the left atrium, and is bound anteriorly by the pericardial reflections over the aorta and pulmonary artery and posteriorly by pericardial reflection extending transversely between the right and left superior pulmonary veins. On the left and right it communicates with the main pericardial cavity. The oblique sinus lies in the pericardial cavity posterior to the left atrium and anterior to the esophagus. It is bound laterally by the pericardial reflections over the pulmonary veins and IVC. The transverse sinus lies superior and anterior to the oblique sinus and is separated from it at this level by two layers of serous pericardium transversely connecting the right and left superior pulmonary veins .
The recesses are pericardial cavity diverticula between major vessels. There are categorized 4 on the basis of whether they arise from the (1) pericardial cavity proper,(2) the transverse sinus , or the(3) oblique sinus.
The pulmonary vein recesses 4, which are usually small, lie along the lateral borders of the heart between the superior and inferior pulmonary veins. The anatomy of these recesses are important in catheter ablation of atrial fibrillation.
The superior aortic recess 4 extends anterior to the ascending aorta and has anterior, posterior, and right lateral portions . The anterior portion of the superior aortic recess has a characteristic triangular shape as it insinuates itself between the ascending aorta and the main pulmonary artery. The lateral portion similarly insinuates itself between the ascending aorta and the SVC. The posterior portion lies posterior to the ascending aorta. The inferior portion of the superior aortic recess communicates with the transverse sinus.
The inferior aortic recess4 extends inferiorly from the transverse sinus posterior to the aorta and anterior to the left atrium, extending inferiorly to the level of the aortic valve.
The right and left pulmonic recess 4 lie inferior to the right and left pulmonary arteries, respectively.
The upper right lateral extension of the oblique sinus lies behind the right pulmonary artery and medial to the bronchus intermedius, where it is called the posterior pericardial recess 4.
Clinical considerations :
Knowledge of the anatomy of pericardial sinuses and recesses helps to avoid a misdiagnosis of lymphadenopathy or other mediastinal pathology (thymic , aortic dissections , esophageal )
Hemorrhagic Effusins
- Renal Failure
- TB
- Malignancy
- Aortic Dissection
- Idiopathid
Clinical presentations
- Acute and recurrent pericarditis
- Pericardial effusion without major hemodynamic compromise
- Cardiac tamponade
- Constrictive pericarditis
- Effusive-constrictive pericarditis
Trauma
References:
Sobel Burton
Broderick LS, Brooks GN, and Kuhlman JE. Anatomic Pitfalls of the Heart and Pericardium. RadioGraphics 2005;25:441-453
Shabetai Ralph
Wang et al CT and MR Imaging of Pericardial Disease RadioGraphicsVol. 23, No. suppl_1
Video
Pericardium ken HubYou Tu Tube