
Biventricular Pacemaker
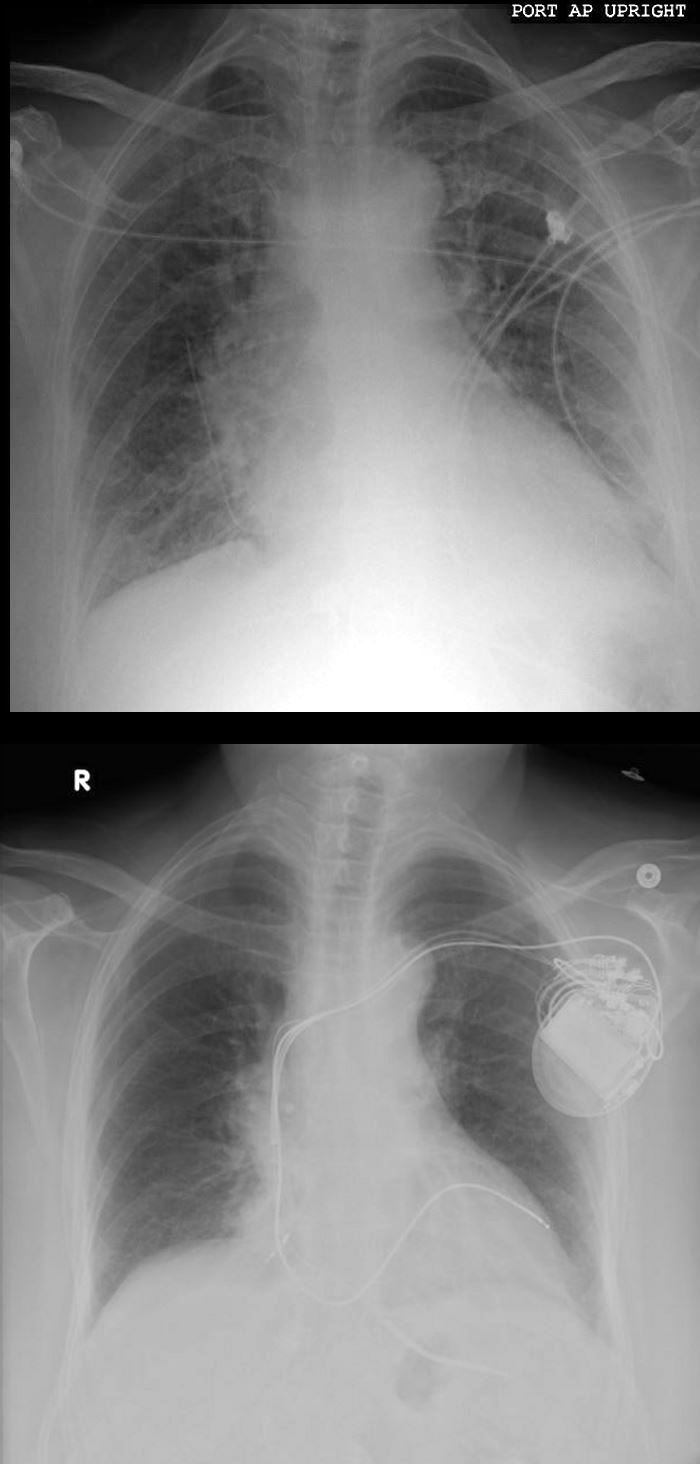
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non-compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Volume measurements showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Following placement of biventricular pacemaker CXR showed resolution of the heart failure, but persistence of the LAE.
Ashley Davidoff MD
Sarcoidosis and VT

57-year-old male with pathology findings consistent with granulomatous hepatitis and non-necrotizing granulomas in inguinal lymph nodes both consistent with sarcoidosis but without pulmonary findings. Lymphadenopathy is also present in the axillae and groins without involvement of the mediastinum
? Associated cardiovascular findings include findings consistent with hypertrophic cardiomyopathy with:
o Diabetes and Hypertension
o CXR showing LVE
o Abnormal stress test with concerning regions in RCA territory inferiorly
o Moderate LVH on echo with normal EF (68%) normal LA, RA PAP and RV function. LV mass was 127g/sq. m
o Focal nodular LGE in the anterior apical region in mid myocardial/subendocardial region and in the inferior mid myocardial wall medially
o Subsequently developed episodes of paroxysmal ventricular tachycardia with EP ablation and placement of a defibrillator (ICD)
o LH and RH catheterization performed 6 years after initial studies showed elevation of PC WP of 25 mmHg, mean RA pressure of 16 mmHg, mean PAP of 34 mmHg no CAD
o Subsequent CT showed mildly enlarged LA and RA with mild TR
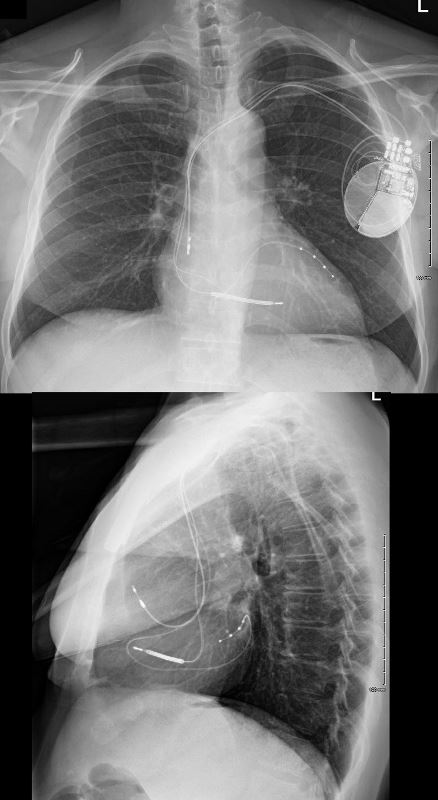
o 6 years after initial presentation he had symptoms of biventricular failure with increasing dyspnea and pedal edema culminating in an acute episode of monomorphic VT episode, ectopic atrial flutter/fibrillation, and left bundle branch aberrancy requiring amiodarone and cardioversion. Underwent upgrade to biventricular upgrade to his ICD
Ashley Davidoff MD
Exchange for Biventricular Pacemaker
Ashley Davidoff MD
References and Links
TCV