
On the CXR

The enlarged LV (a,b) is shaped like an oval and it is likened to a rugby ball or an American football placed on the field at kick off time. LVE on CXR is mostly assessed by an increased cardiothoracic ratio as well as the accentuation of the ovoid shape. (lower images c, d,e, f)
Ashley Davidoff MD
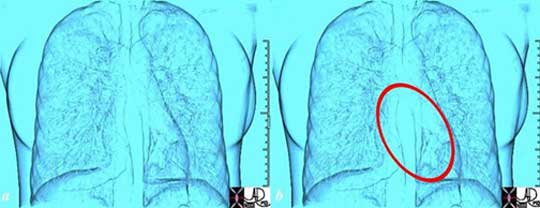
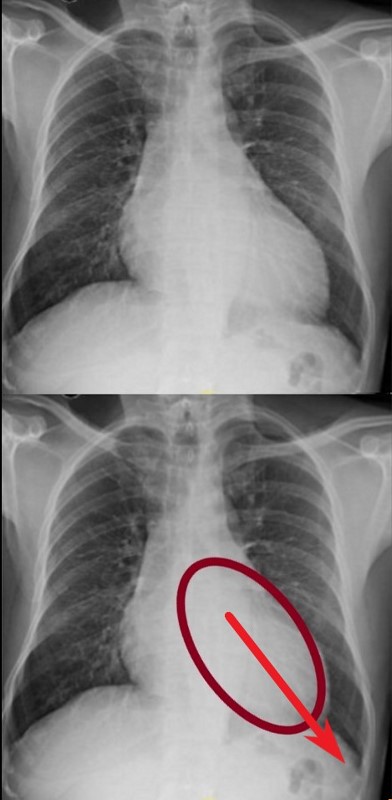
DOWN AND OUT
The left ventricle (LV) enlarges in a posterior, downward and lateral direction resulting in the characteristic changes of LVE on CXR
Ashley Davidoff MD
X- Section CT and MRI
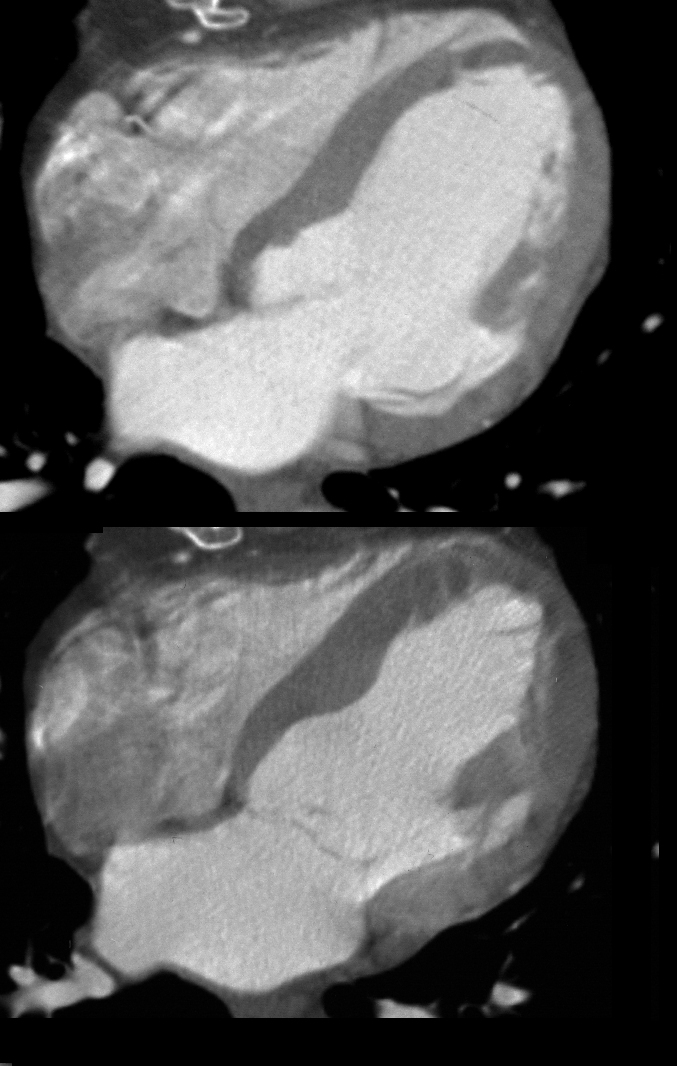
Tags, LV, CT, systole, diastole,
Ashley Davidoff MD 24839c
MRI Systole and Diastole
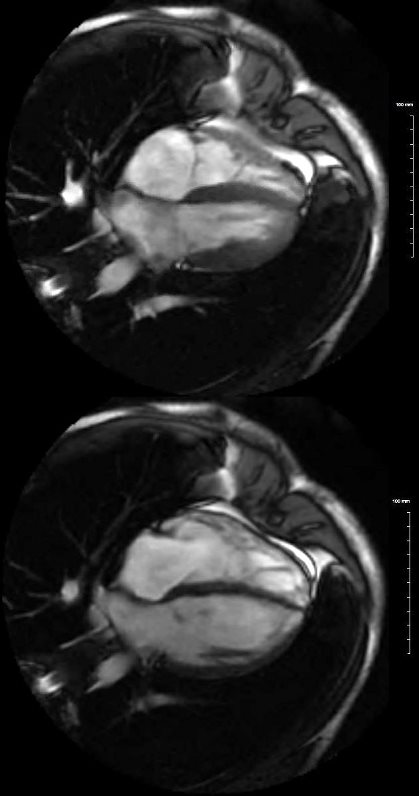
This is the MRI of a 19 year old male who presented with syncope and the study was performed to identify a possible arrhythmogenic focus
White blood imaging using 4 chamber view shows a normal sized heart in systole (above) and diastole below. The left and right atria have flattened surfaces, and occupy about 1/3 the volume of the ventricles. The RV volume is about 2/3 the volume of the LV. The wall of the LV in diastole (lower image) is less than 1 cms and the wall of the RV is barely seen and is in the range of about 3mm. Note in diastole the MV and TV are open
Ashley Davidoff MD
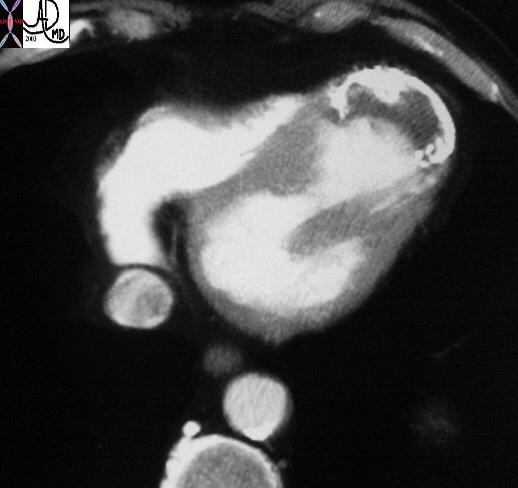
Angiography
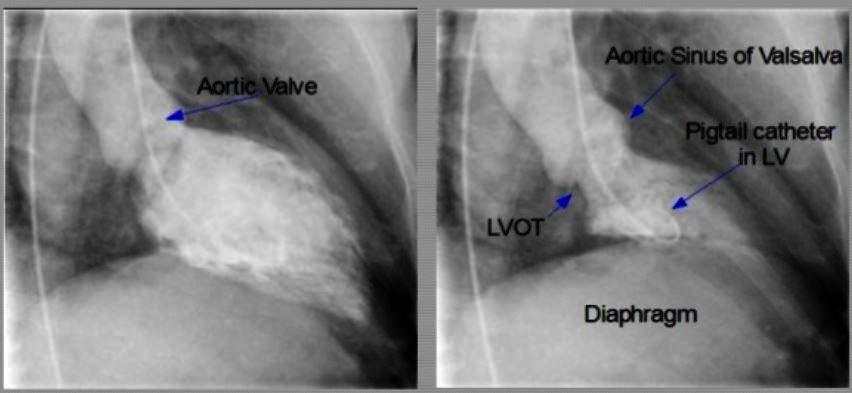
Courtesy Slide Share Shyam Saidharan
In Disease
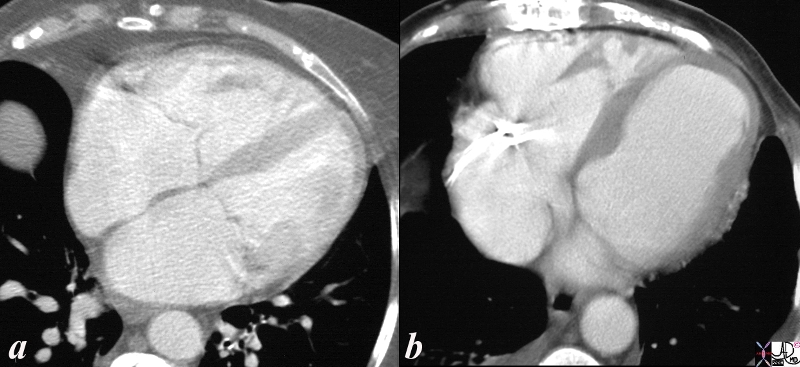
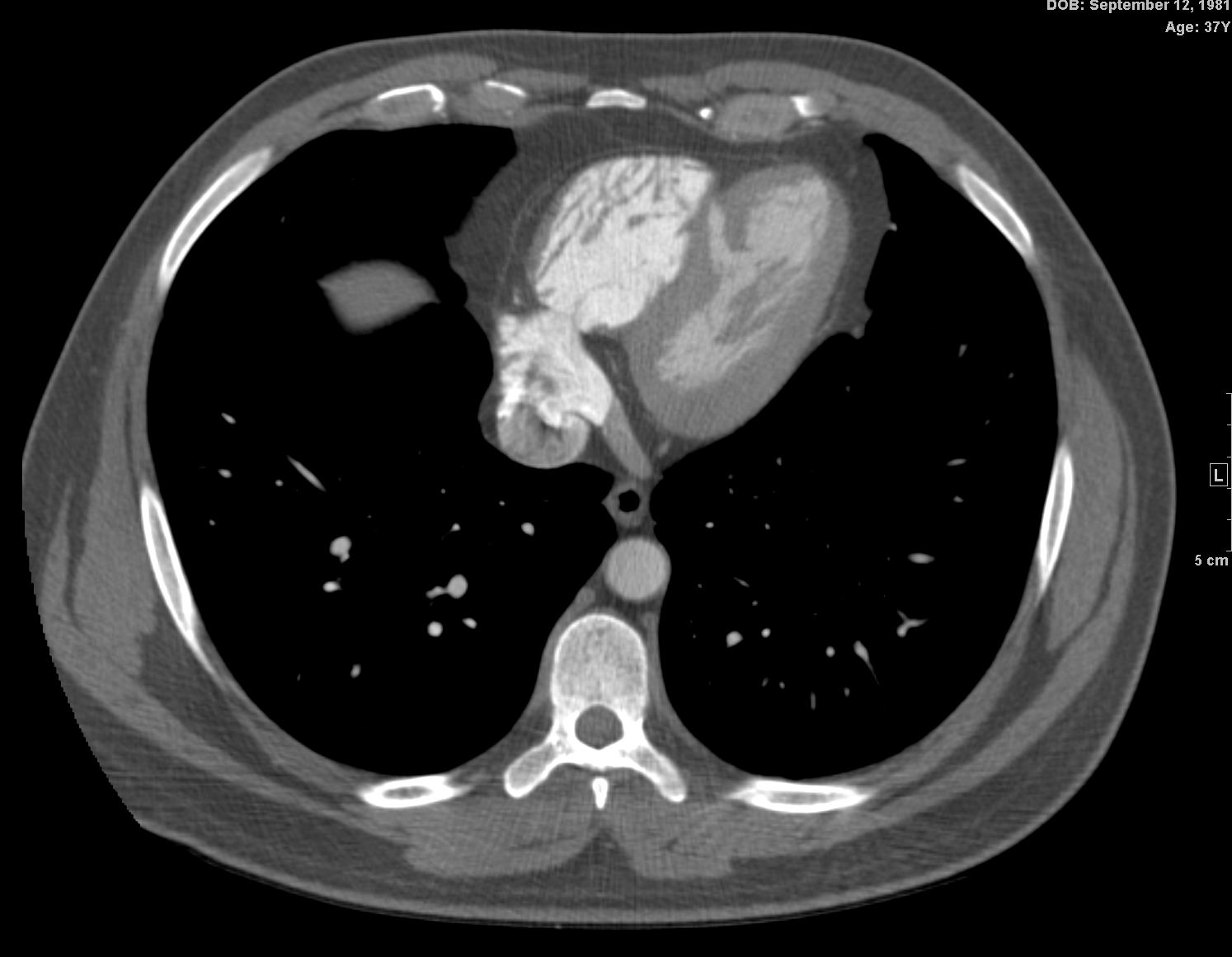
Axial images through the chest show a normal patient (a) and a patient with an aneurysm of the left ventricle (b). In the normal image of the ventricles the shape of the apex of the LV is slightly pointed . The bulbous shape of the apex of the left ventricle in the second image becomes obviously abnormal and is diagnostic of a left ventricular aneurysm.
Courtesy Ashley Davidoff copyright 2009 all rights reserved 26336cc01.8s
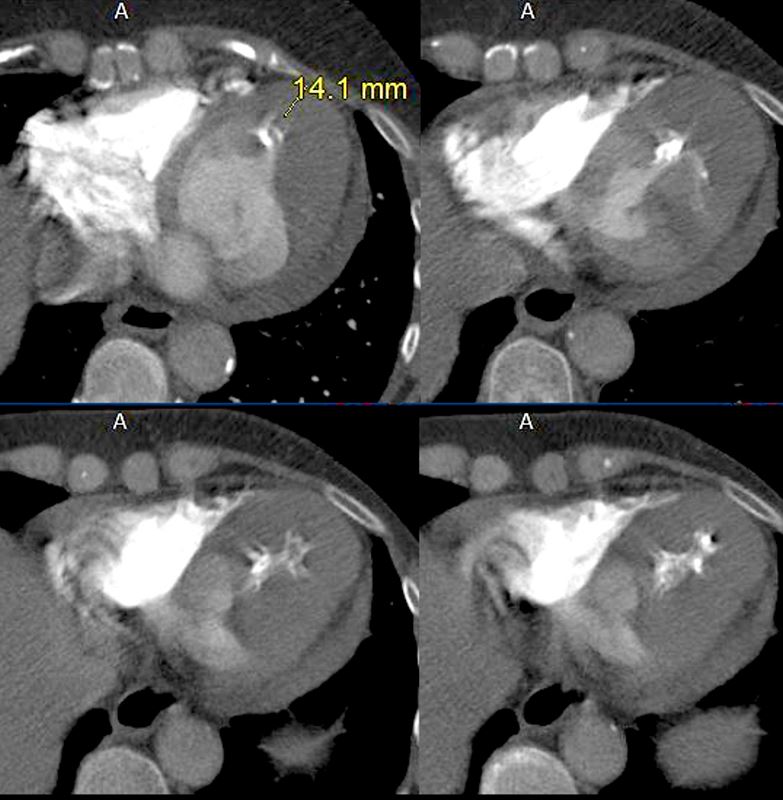
Ashley Davidoff MD 27129b
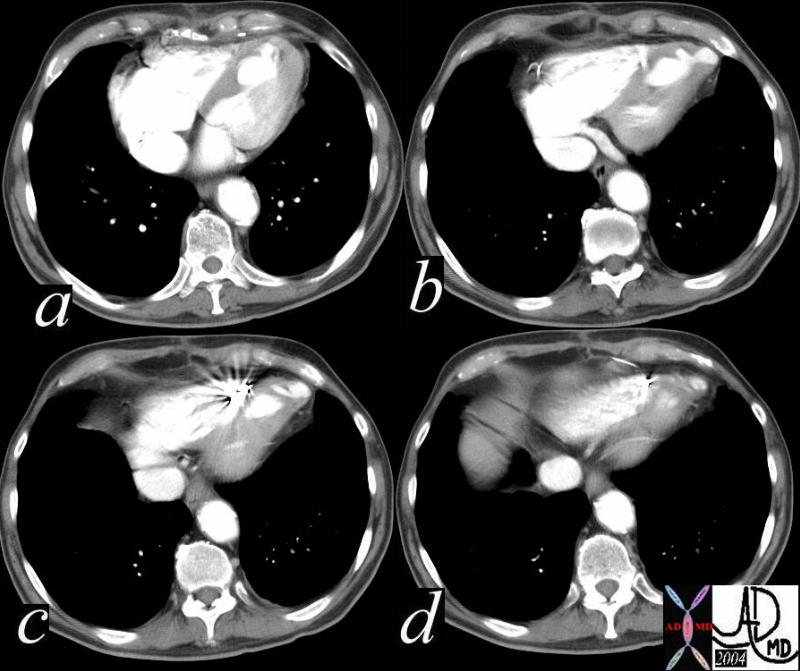
Description: This series of CT scans through the bottom of the left ventricle show an apical outpouching in this patient who has not had previous evidence of CAD. This finding is characteristic of a left ventricular diverticulum. . 38332c code CVS heart cardiac LV apex diverticulum congenital cardiac imaging radiology CTscan congenital
Keywords: CVS heart cardiac LV apex diverticulum congenital cardiac imaging radiology CTscan congenital Ashley Davidoff MD 38332c

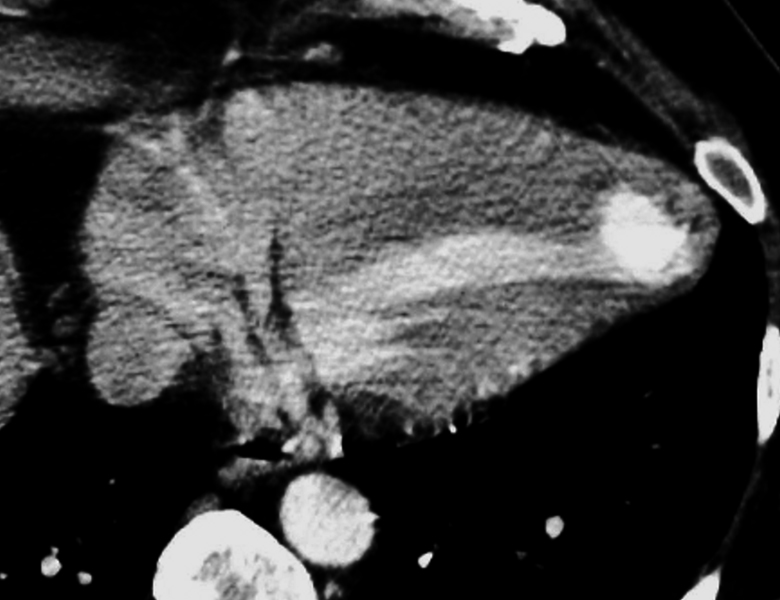
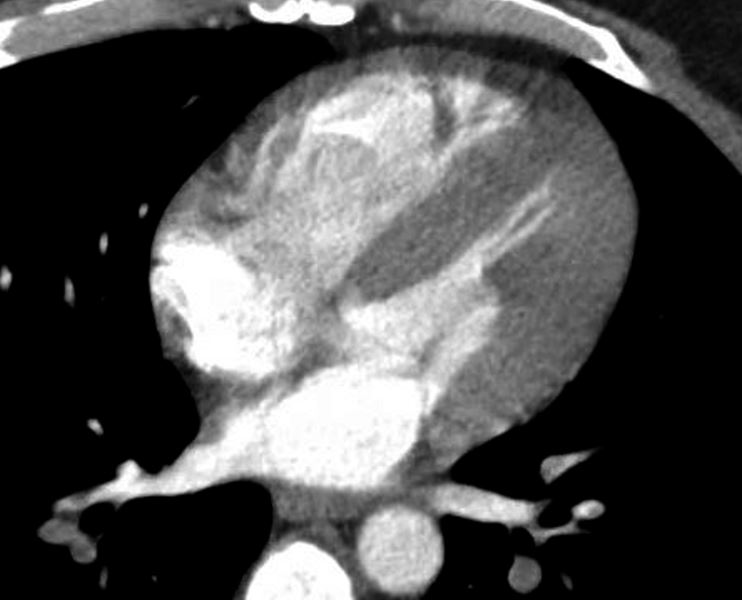
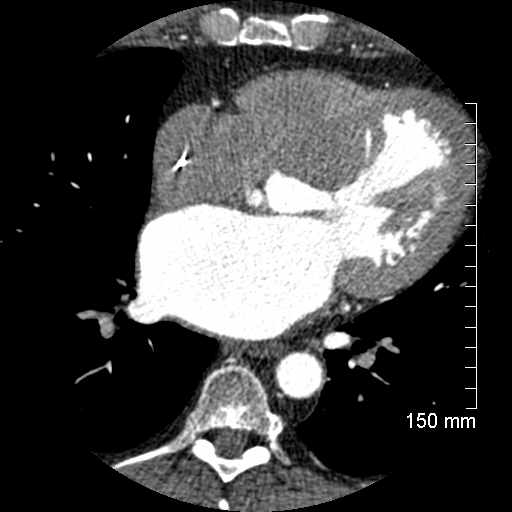
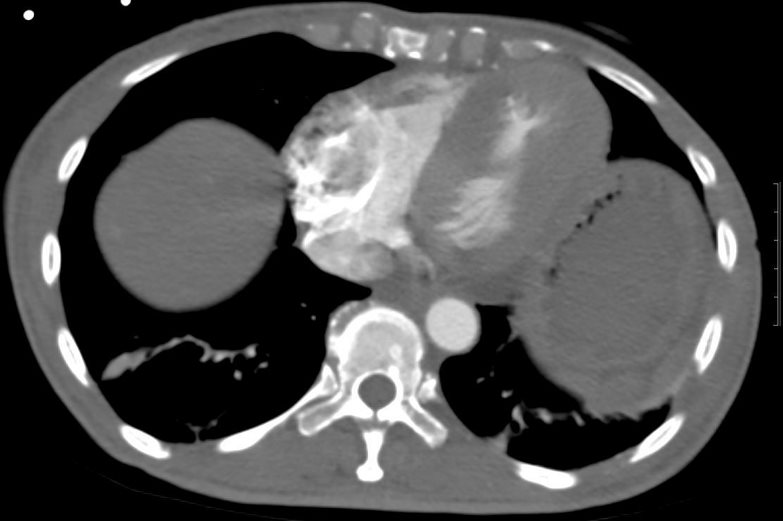
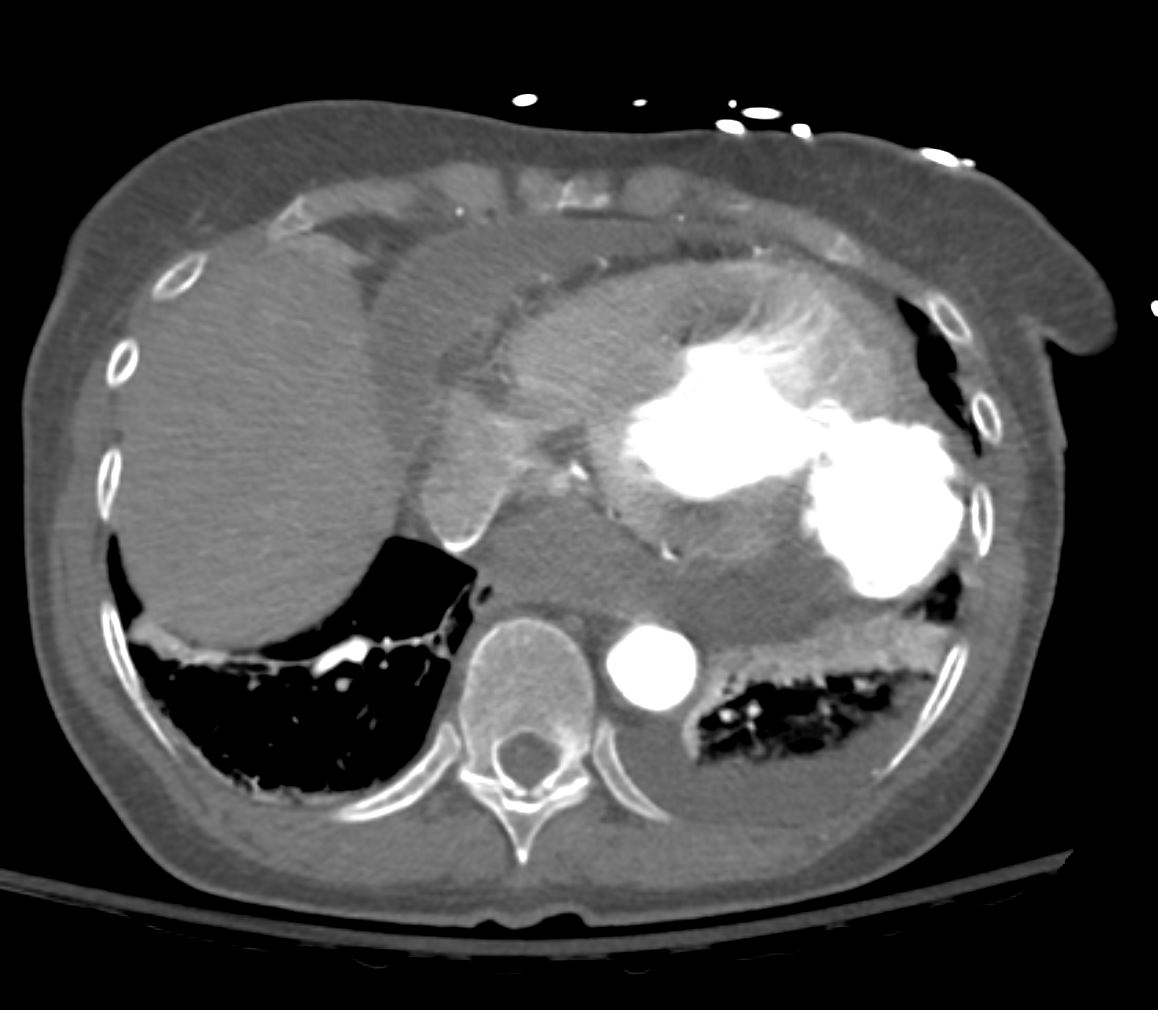
Recent MI
This elderly female recently sustained an acute MI and the resulting functional myocardial loss has resulted in a globular deformity of the heart as seen on this non gated CT through the chest. Note the malorientation of the posterior papillary muscle that prohibits normal function of the mitral valve and results in mitral regurgitation. A Small pericardial effusion is present.
Courtesy Ashley Davidoff MD copyright TCV 2008 75517
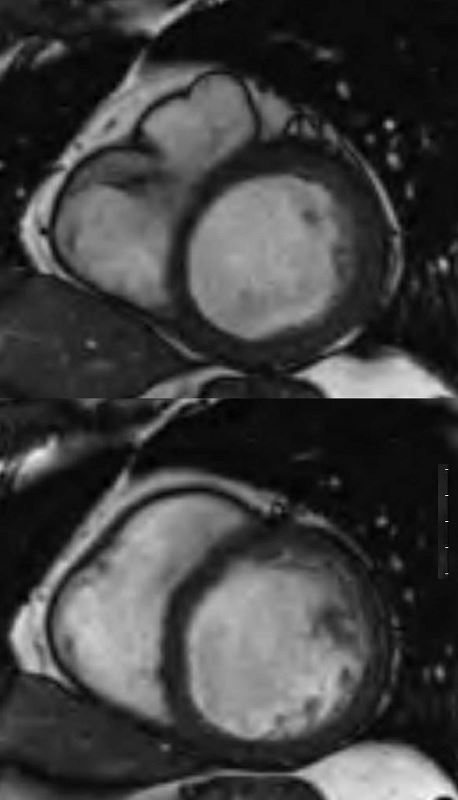
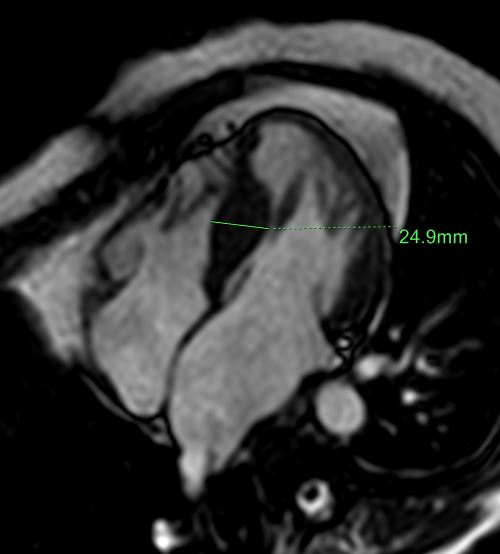
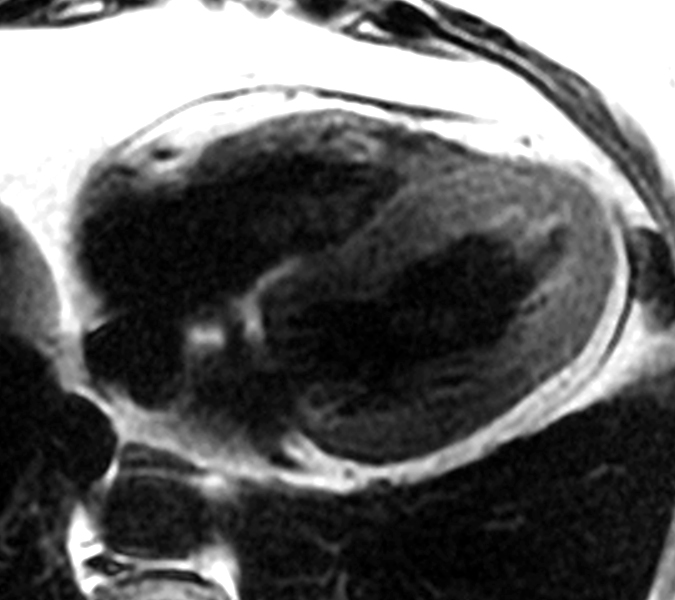
61 male, alcoholic with congestive cardiomyopathy
MRI in short axis through the body of the LV in systole (above) and diastole (below)shows a dilated LV without much change in the dimensions of the LV cavity. EF was between 10% and 20%
Ashley Davidoff MD
Concentric Hypertrophy
Ballet slipper appearance in Systole with
Left ventricular hypertrophy
Ashley Davidoff MD
130536b
Asymmetric Septal Hypertrophy
48 year old male with a history of IHSS by echo and CT findings consistent with f subaortic stenosis characterised by eccentric thickening of the septum in the subaortic region, a slightly thickened anterior leaflet of the mitral valve, and an enlarged left atrium.
Ashley Davidoff MD 116175
{kind=link}
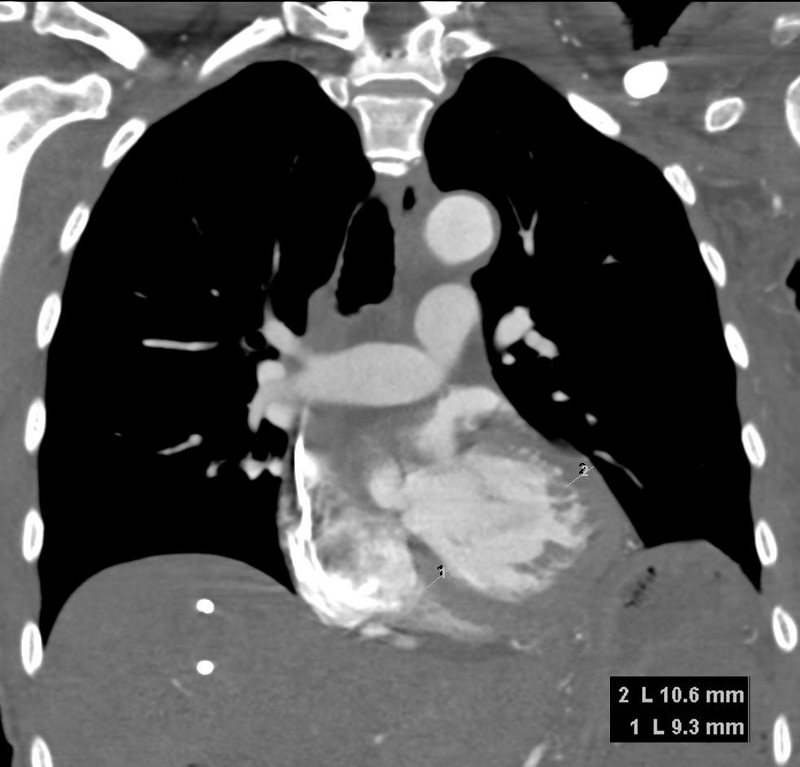
Apical Hypertrophy
64-year-old male with pancreatic carcinoma and apical hypertrophic cardiomyopathy.
CXR shows left ventricular configuration with an unusually prominent left ventricle. CT shows dominant apical hypertrophy of the LV.
Echocardiogram confirmed the presence of apical hypertrophy with mid systolic gradient within the LV cavity of 38mmHg.
Ashley Davidoff MD
64-year-old male with pancreatic carcinoma and apical hypertrophic cardiomyopathy.
CXR shows left ventricular configuration with an unusually prominent left ventricle. CT shows dominant apical hypertrophy of the LV.
Echocardiogram confirms the presence of apical hypertrophy with mi systolic gradient within the LV cavity of 38mmHg.
Ashley Davidoff MD
73-year-old female with a history of CREST syndrome, COPD and apical hypertrophic disease with extensive apical calcification
Ashley Davidoff MD 130453c.8
Takotsubo
Ashley Davidoff MD
tags, LV, pseudoaneurysm, hemopericardium, 133893
TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
Ashley Davidoff MD

TAKO TSUBO = CRAB TRAP

Takotsubo Heart – aka Broken heart Syndrome – A transient apical dyssynergy due to extreme emotional and or physical stress
Ashley Davidoff MD
Ventricular Septal Defect

Ashley Davidoff MD
Rhabdomyoma

The fetal ultrasound of the heart shows an echogenic filling defect in the apex of the left ventricle (LV). Maternal history of tuberous sclerosis suggests a diagnosis of a rhabdomyoma in the LV
Ashley Davidoff MD
Collage of the Normal and Abnormal Shapes of the LV in Axial Projection
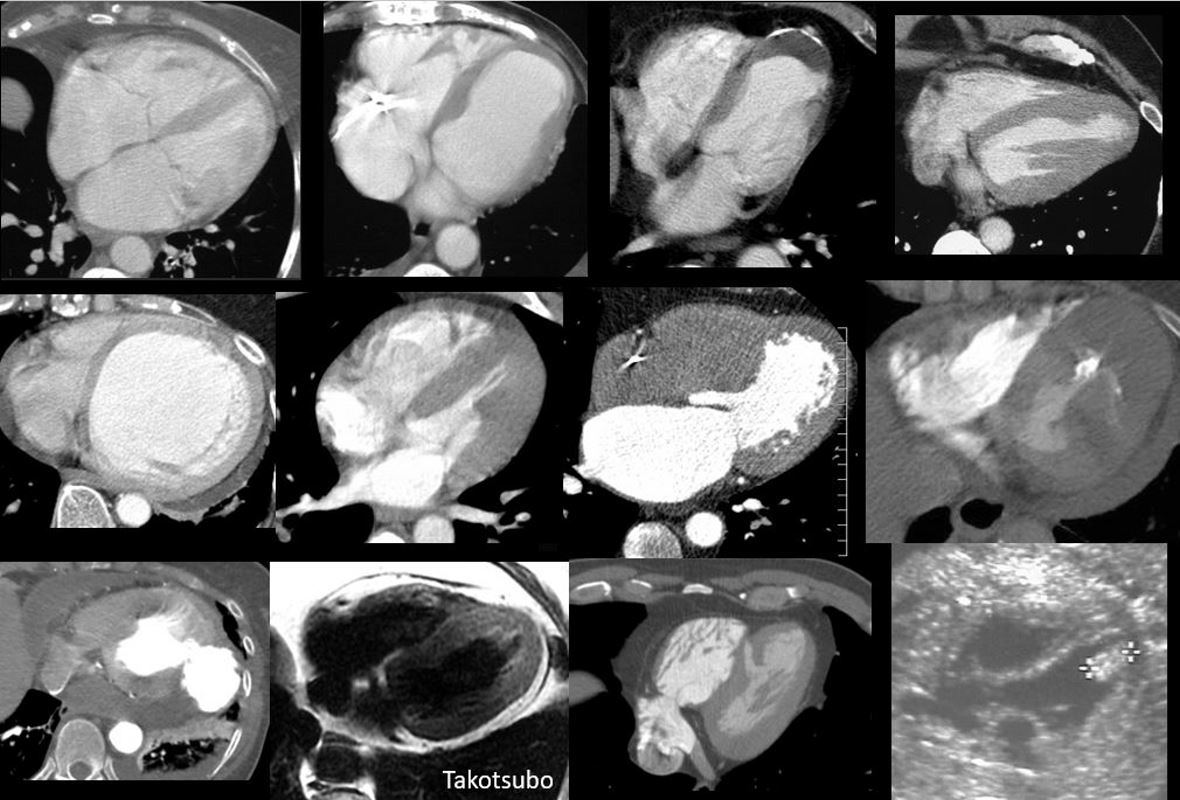
2nd row Dilated congestive cardiomyopathy, concentric hypertrophy, asymmetric septal hypertrophy, apical hypertrophy
Bottom row pseudoaneurysm of the LV, Takotsubo heart, VSD, LV hamartoma in a fetus
Courtesy Ashley Davidoff MD
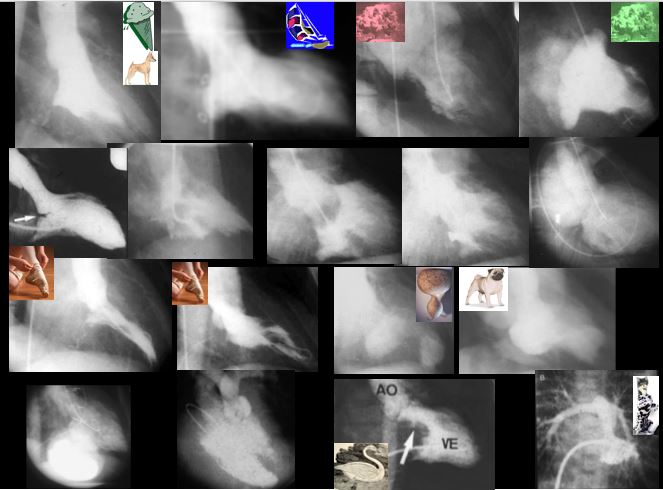
The collage reveals the variation in the shapes of the LV in diseases of the LV and of the mitral valve.
Top row (from l to r) Normal appearance of the LV in systole with an ice cream cone shape. Billowing posterior leaflet of the mitral valve with prolapse of the posterior leaflet with mild mitral regurgitation. Image 3 and 4 in patients with Marfan?s syndrome show prolapse of both the anterior and posterior leaflets of the mitral valve with severe mitral regurgitation
2nd row 1st image is a patient with a cleft mitral valve with mild mitral regurgitation. The second image shows catheter induced mitral regurgitation. Image 3 and 4 show evidence of rheumatic mitral disease, with image 3 showing poor excursion of the MV and both images 3 and 4 show enlarged papillary muscles. Image 4 shows a ruptured papillary muscle 8 days post MI with severe mitral regurgitation.
3rd row 1st image is a patient with IHSS with hypercontractile LV (that looks like a ballet shoe) with mitral regurgitation due to systolic anterior motion of the mitral valve during systole. The second is a patient with aortic stenosis and also has a ballet shoe appearance to the LV due to hypercontractility. Image 3 is a patient with apical dyskinesis (aneurysm) and compensatory midventricular hypercontractility. Last image is a similar situation, but the pug nose appearance of the apex is caused by thrombus in the apex
4throw 1st image is a patient with a basal pseudoaneurysm post MI, 2nd a patient with Tetralogy of Fallot with a conal VSD , overriding aorta and PS. Next is the swan neck deformity of the LV outflow tract in complete AV canal defect. The last is an LV subtending the PA in DTGA ? a dog born to be a cat
Ashley Davidoff MD