
Linear
Congestive Cardiomyopathy
61 male, alcoholic
Imaging shows a dilated lv and normal sized LA, RA, and RV. EF was between 10% and 20%
Ashley DAvidoff MD
{kind=link}
{kind=link}
Diffuse
Amyloidosis
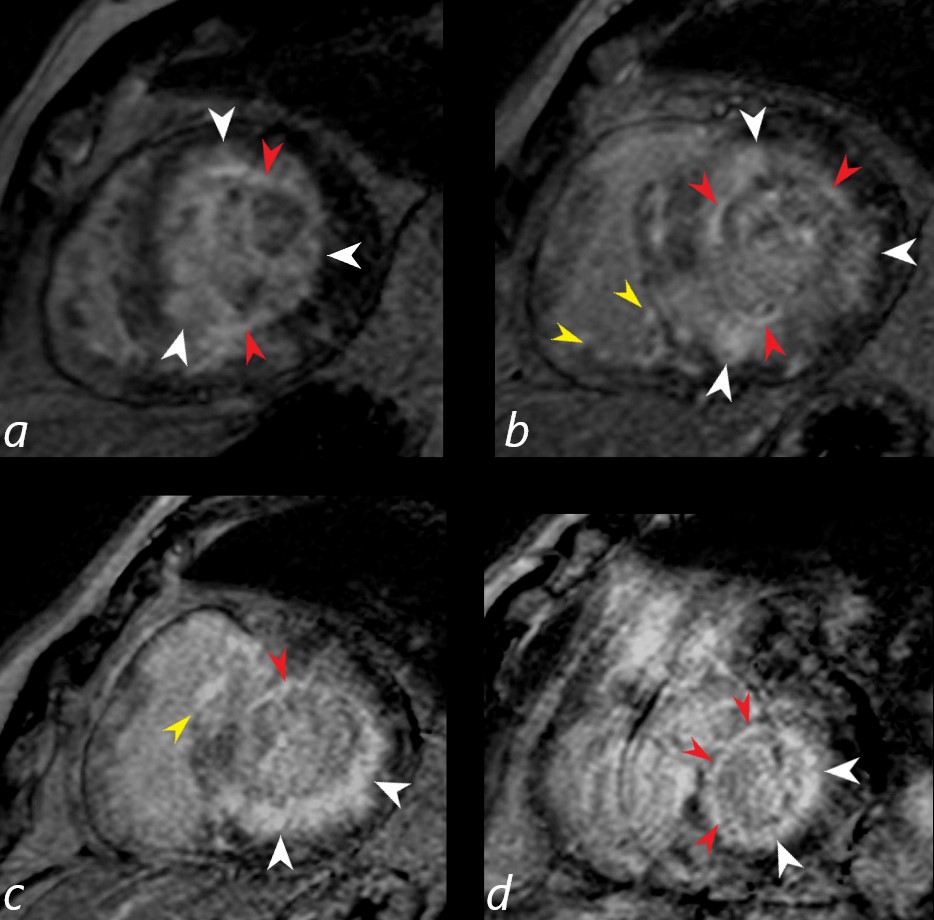
Gated short axis delayed gadolinium sequence through the base LV during diastole and shows subendocardial LGE (red arrowheads in a,b,c, and d, diffuse mid myocardial LGE (white arrowheads) (a,b,c,d) and subepicardial LGE in the RV (yellow arrowheads (b,c)
Ashley Davidoff MD
fabry’s Disease
Fabry Disease
{kind=link}
?Delayed enhanced images of 64-year-old heterozygotic woman with Fabry?s disease?related cardiac hypertrophy. Minimal thinning of basal segment of left ventricular inferolateral wall is associated with thick mesocardial striae of delayed enhancement shown on short-axis delayed enhanced images.?
De Cobelli et al Delayed-Enhanced Cardiac MRI for Differentiation of Fabry?s Disease from Symmetric Hypertrophic Cardiomyopathy
AJR Volume 192, Issue 3 2009
 LGE in FABRY DISEASE
LGE in FABRY DISEASE
?40-year-old man with Fabry?s disease?related hypertrophy. Long-axis delayed enhanced images show typical pattern of delayed enhancement: thick striae involving inferolateral wall of basal segment of left ventricle in mesocardial distribution. Note sparing of subendocardial layer.
De Cobelli et al Delayed-Enhanced Cardiac MRI for Differentiation of Fabry?s Disease from Symmetric Hypertrophic Cardiomyopathy?
AJR Volume 192, Issue 3 2009
{kind=link}
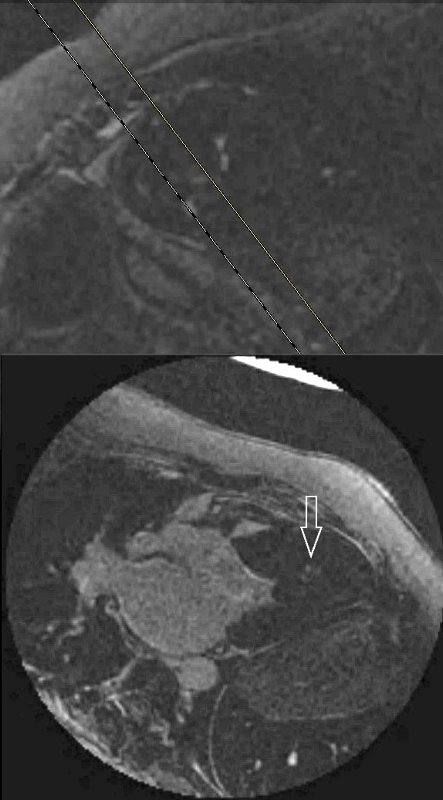
Fine Line Curvilinear
{kind=link}
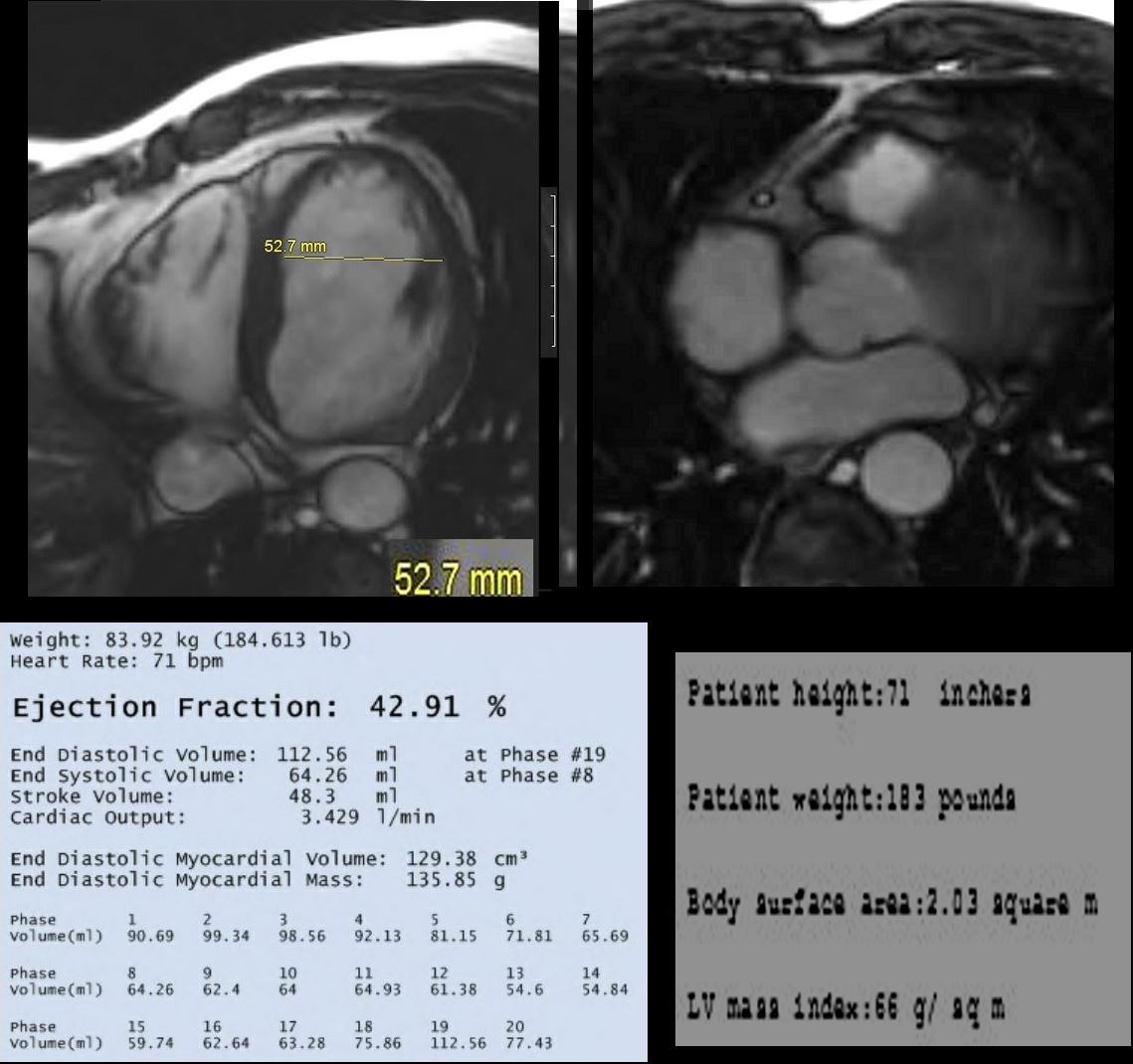
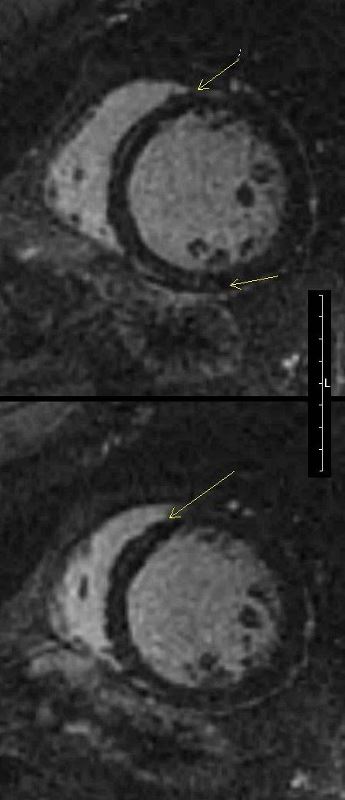
Axial MRI through mid ventricle using white blood imaging algorithm, in a 66 year old male with mild dyspnea, shows mild left ventricular (LV) enlargement (LVE) with an internal diameter of 5.3cms (normal 4.5cms) (top left), normal sized left atrium (LA) approximating the size of the normal aorta (Ao) with an ejection fraction of 43% and normal end diastolic volume (112 ccs) and normal LV mass (66gms/sq m)
Ashley Davidoff MD
{kind=link}

Short axis MRI in a 66 year old male with mild dyspnea, post gadolinium infusion through mid ventricle using white blood imaging algorithm, shows linear enhancement in the mid myocardium of the septum (white arrows in b) consistent with congestive cardiomyopathy. Myocarditis is included in the radiological differential diagnosis.
Ashley Davidoff MD
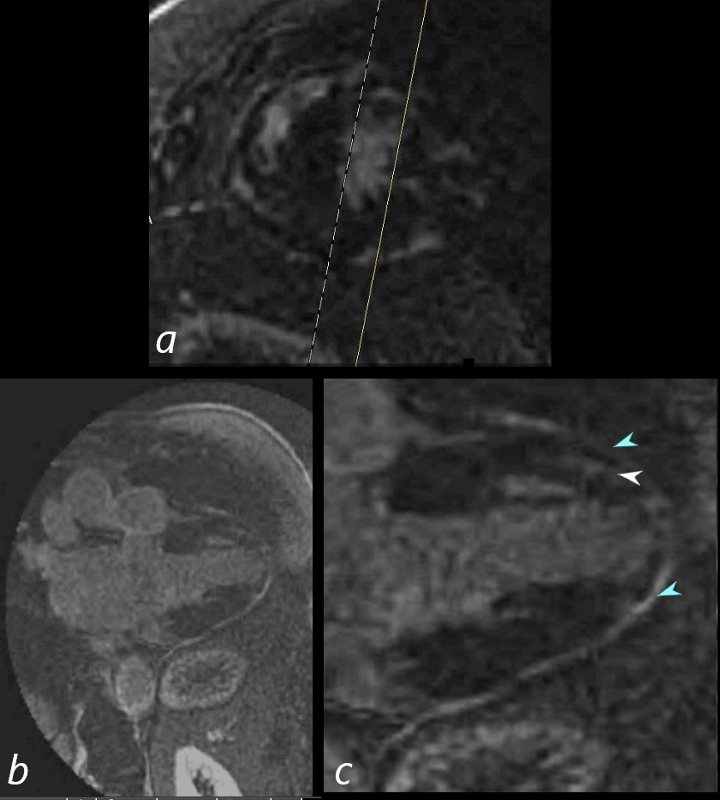
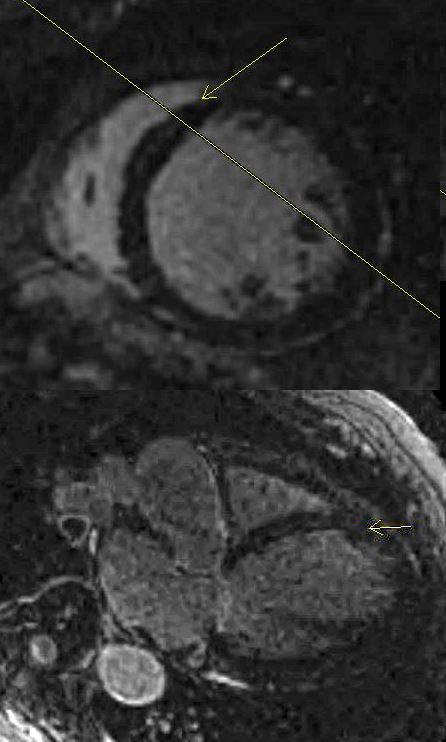
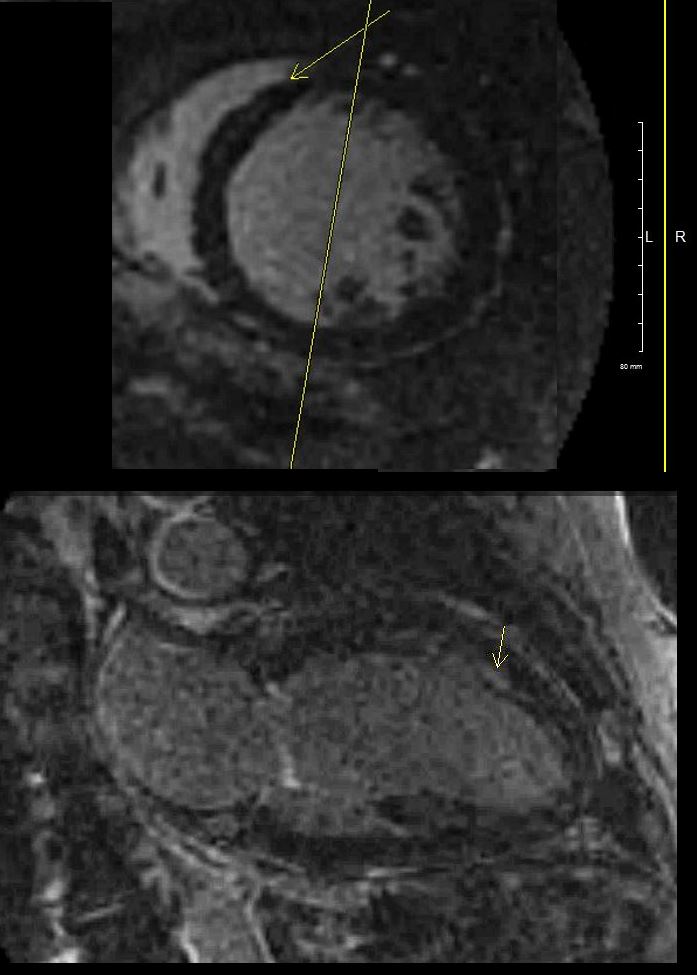
69-year-old male presented with history of cardiomyopathy and atrial fibrillation
In this series, the long axis 2 chambered view (c is magnified view of b) reveals intense continuous pericardial disease (teal blue arrowheads) and mid myocardial linear-nodular LGE (white arrowhead)
Ashley Davidoff MD
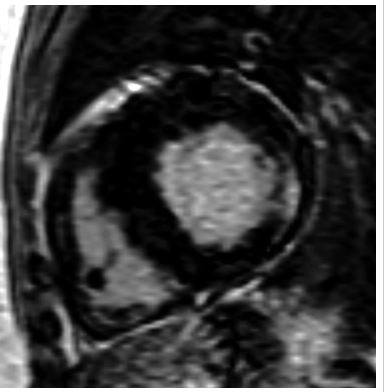
Nodular Form
53 year old male with a clinical history of sarcoidosis and right bundle branch block. Echocardiography showed left ventricular hypertrophy and normal ejection fraction
MRI shows multifocal regions of LGE in the mid myocardium involving the inferobasal portion and inferolateral portion of the of the LV
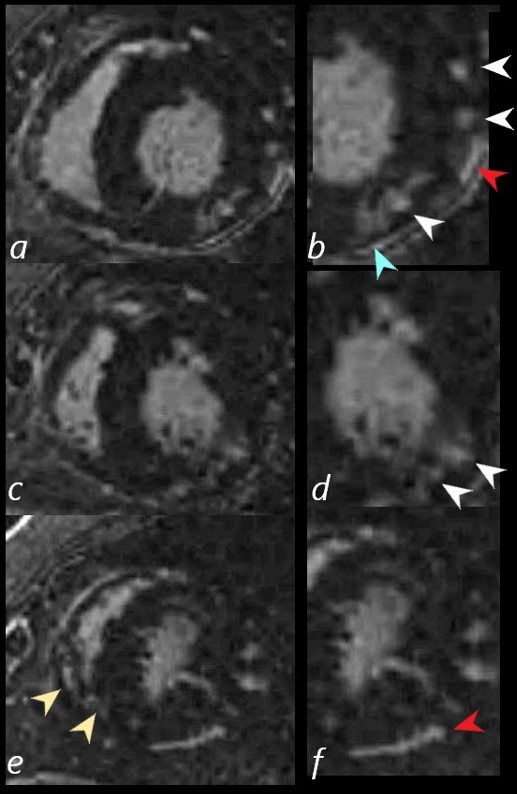
69 year old male presented with history of cardiomyopathy and atrial fibrillation
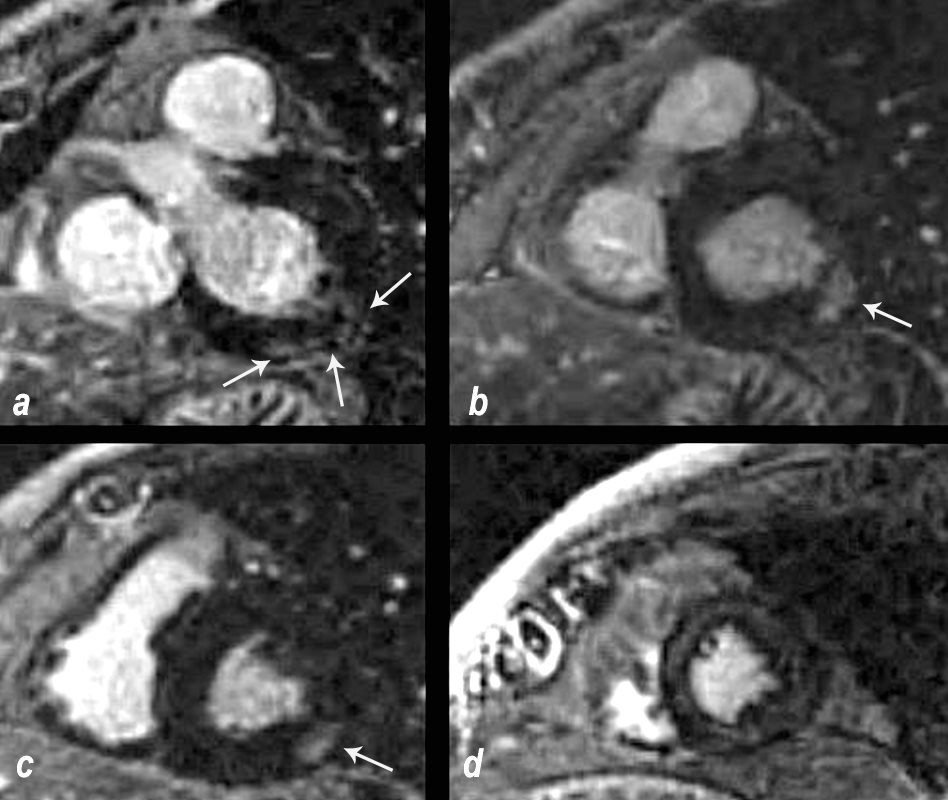
The findings on MRI are highly suggestive of sarcoidosis. There are multicentric foci of LGE in linear and nodular form in the mid myocardial and subepicardial layers and likely in the pericardium and myocardium of the right ventricle.
In this series images on the right (b,,d,,f) are magnified views of images on the left (a,c,e)
There are multicentric foci of LGE nodular form in the mid myocardial region (white arrowheads) linear LGE in the subepicardial layers (red arrowheads, b and f) in the pericardium (teal blue arrowhead) and myocardium of the right ventricle (yellow arrowhead e).
There was associated global hypokinesis of the LV with an EF of 40%, and increase in the LV mass of 120gms/ sq m
Ashley Davidoff MD
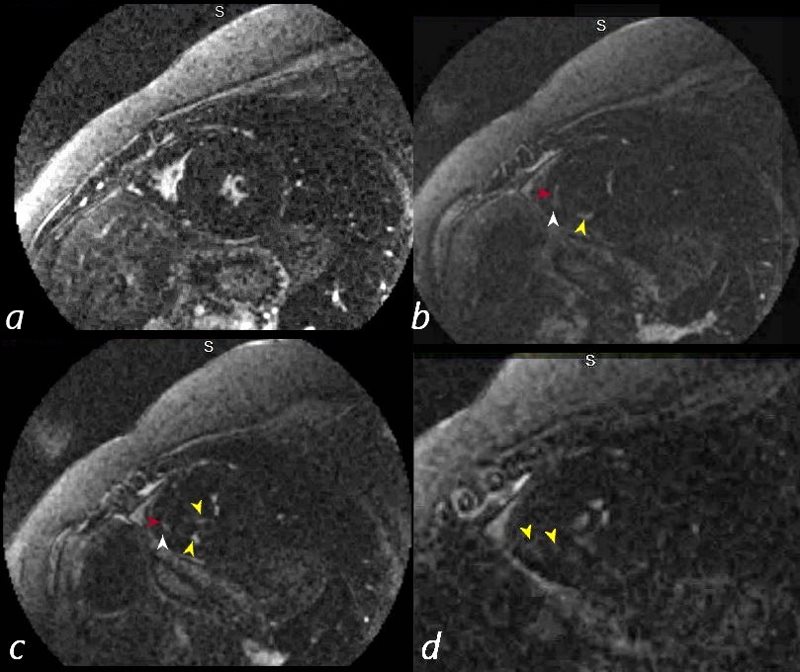
54-F-sarcoidosis-pericardial-effusion.8.jpg
54 year old female with a history of sarcoidosis diagnosed on a groin node biopsy. History of recurrent pericarditis with tamponade s/p pericardial window
MRIs performed 4 months apart reveal vague nodular changes at the hinge points and in the inferolateral portions of the left ventricle. In the first short axis scan the changes were thought to be artifact. However on follow up the finding are persistent and therefore real.
On both scans there is diffuse enhancement of the pericardium.
Courtesy Ashley Davidoff MD
{kind=link}
HOCM
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
37-year-old female with a history of hypertrophic cardiomyopathy presented to the ER with pleuritic chest pain
CXR showed cardiomegaly with evidence of left ventricular enlargement and left atrial enlargement.
CTA showed no evidence of PE but confirmed the presence of LAE and LVH with asymmetric septal thickening and relative sparing of the apex.
A pyrophosphate scan was negative for amyloidosis
An echocardiogram confirmed the presence of an obstructive cardiomyopathy with systolic anterior motion of the mitral valve and late systolic mitral regurgitation. The left atrium was enlarged and the right atrium was mildly enlarged. The ejection fraction was normal and estimated to be between 64%. There was a resting gradient across the outflow tract of 40-68 mmHg. LV mass index was 156g/sq m
MRI confirmed the findings of the echo showing asymmetric septal hypertrophy, systolic anterior motion of the mitral valve with mitral regurgitation. The LA was 5.2cms, septal wall in diastole was 27.6mms and free wall was 16.8 mms. LV cavity size in diastole was normal. RA and RV were normal. EF was 70% and LV mass was 130g/ sq. m
Nodular LGE was noted in the mid myocardium in the inferoseptal region at the hinge points and at the antero-apical regions
Ashley Davidoff MD

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
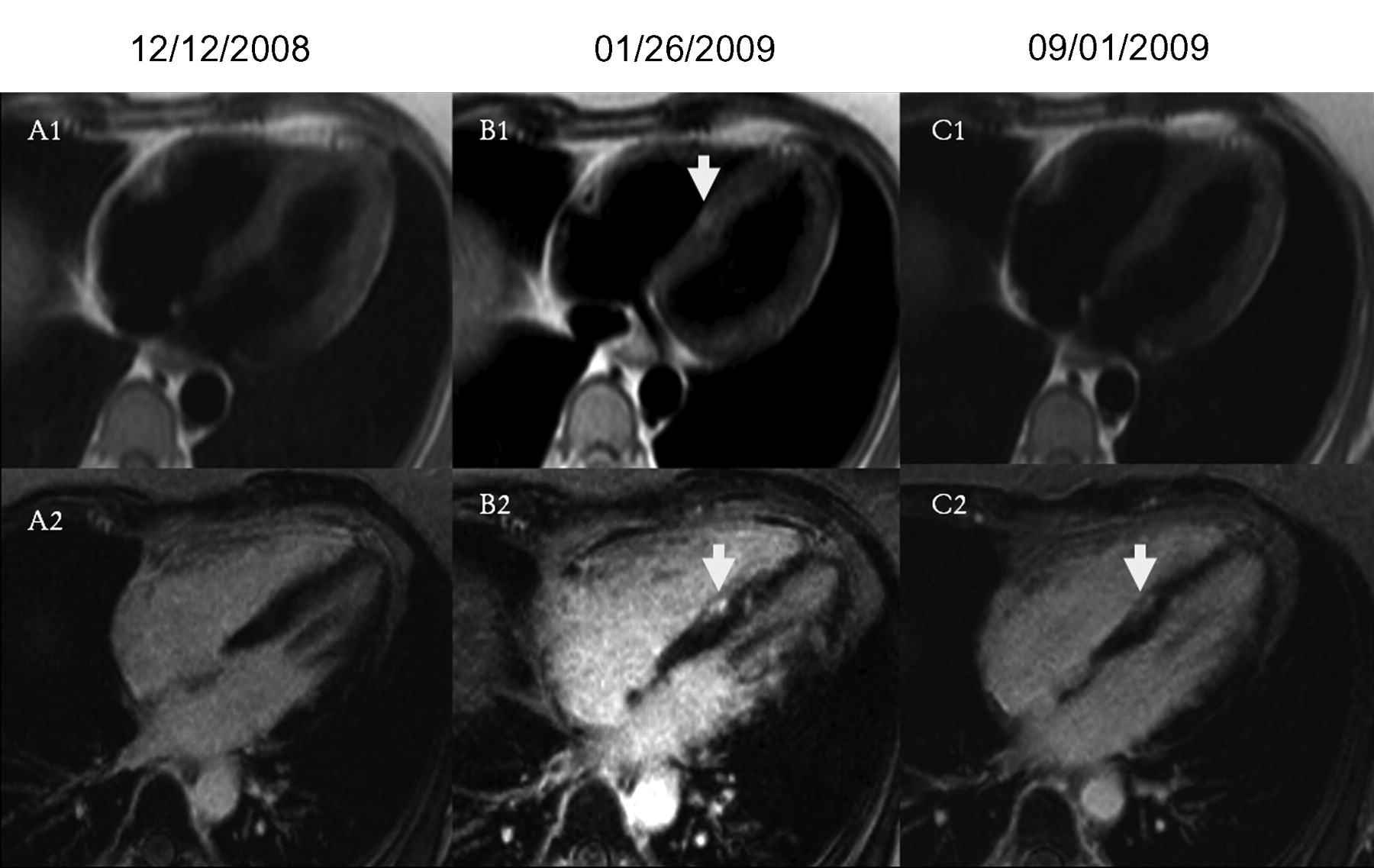
Delayed enhancement images, 4-chamber views. B2 demonstrates interventricular patchy enhancement (arrow) on cardiac MRI performed during an SLE flare and active chest pain. Appearance is typical for myocarditis and a new finding compared to the baseline scan A, with some residual involvement after resolution of the SLE flare and medical treatment (C2). The finding of myocarditis is supported by a patchy enhancement (arrow), consistent with myocardial edema and active inflammation on T2-weighted images without fat saturation. No active inflammation is noted on a followup scan (C1).
Goykman et al Subendocardial Ischemia and Myocarditis in Systemic Lupus Erythematosus Detected by Cardiac Magnetic Resonance Imaging
The Journal of Rheumatology February 2012, 39 (2) 448-450; DOI: https://doi.org/10.3899/jrheum.110812
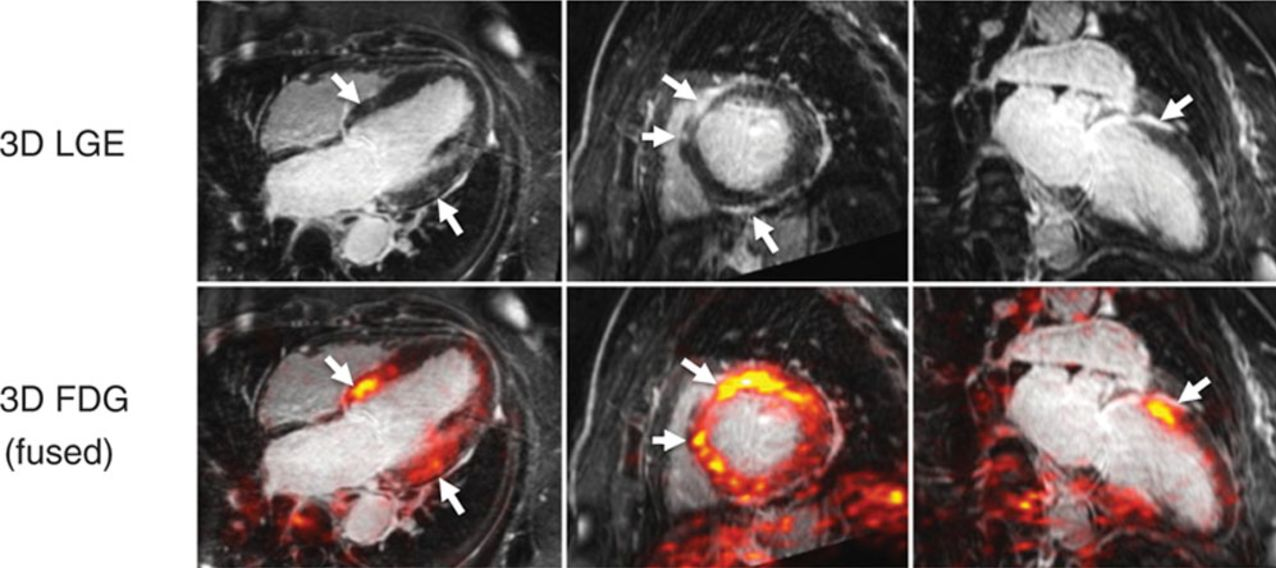
CMR images demonstrating 3-dimensional LGE imaging (top row), also fused with FDG-PET signal (bottom row), suggestive of active inflammation surrounding regions of scar (arrows) in a patient with unexplained cardiomyopathy and suspected cardiac sarcoidosis. Images are shown in the 4-chamber, short-axis, and 2-chamber orientations, respectively. Reproduced with permission from White et al.
Courtesy https://www.acc.org/latest-in-cardiology/articles/2017/04/10/08/43/cardiac-mri-vs-pet
-
References and Links
-
TCV
- Case Studies
-