
Basic Approach To The Heart In The Frontal CXR
Frontal X-Ray- Parts

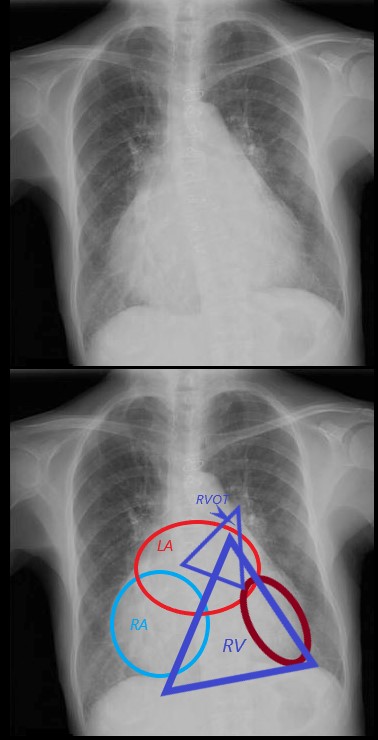
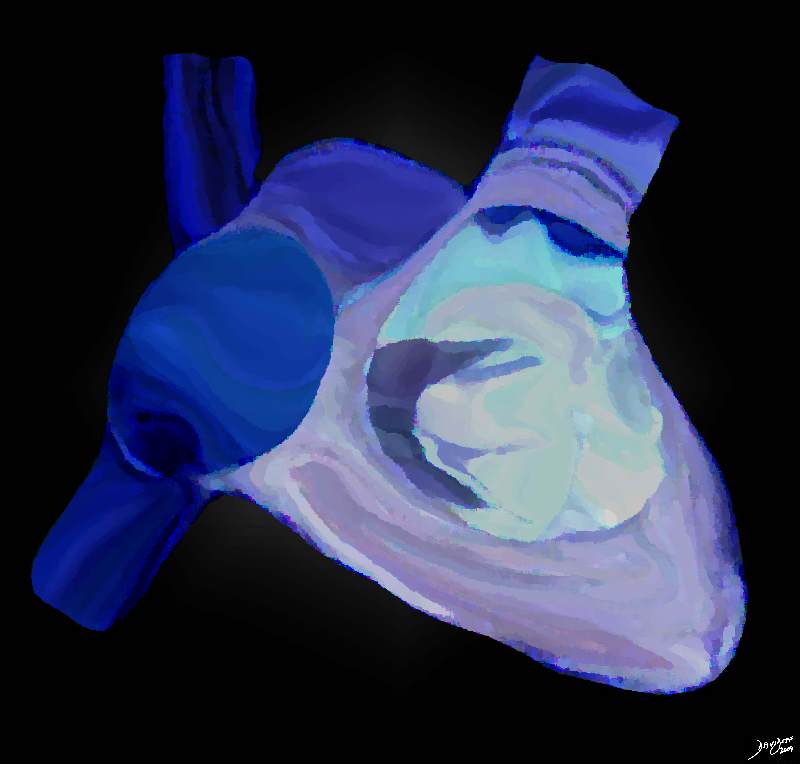
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.
Ashley Davidoff MD
Many Different and Interesting Shapes of the Heart on Frontal View – mostly involving CHD
7 TA Pulmonary atresia pulmonary bay PAtresia TEt 8 L TGA Coronal LTGA is 07197 9 total absent pericardium 10 Tetralogy 11 dextrocardia 12 waterbottle pericardial effusion
Coronal LTGA is 07197
But in Adults There are Two Basic Common Shapes of Cardiomegaly

NORMAL AND TWO BASIC TYPES OF CARDIOMEGALY
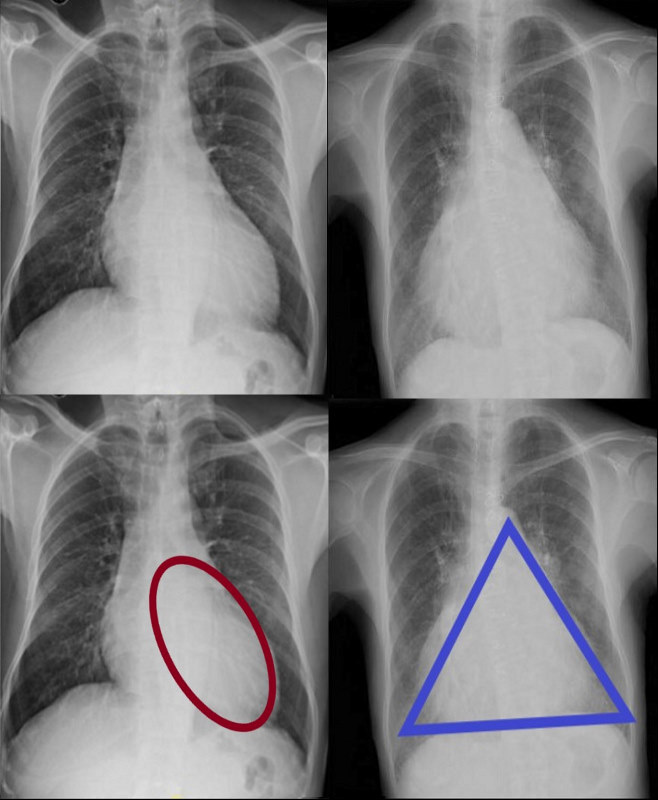
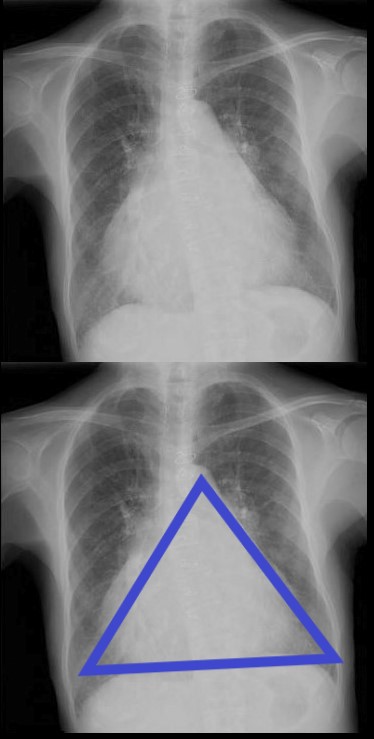
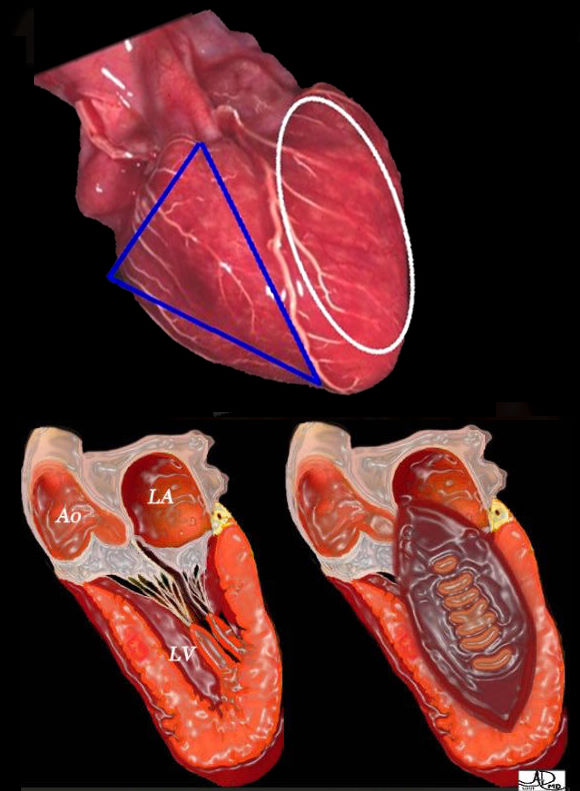
The normal heart (above) is a combination of a triangle and an oval. Cardiomegaly on CXR is mostly assessed by an increased cardiothoracic ratio, and takes on two basic forms based on the overall shape of the heart; the ovoid form (bottom left) which suggests left ventricular dominance and triangular form (bottom right) which suggests right ventricular dominance.
Ashley Davidoff MD
Cardiomegaly on CXR is mostly assessed by an increased cardiothoracic ratio, takes on two basic forms based on the overall shape of the heart; the ovoid form which suggests left ventricular dominance and triangular form which suggests right ventricular dominance.
Ashley Davidoff MD
How to Diagnose Cardiomegaly
Cardiothoracic Ratio
Cardiomegaly -2 different entities
The normal heart (above) is a combination of a triangle and an oval.
The maximum transverse length of the heart is expressed as a percentage of the maximum length of the internal diameter of the chest. When this ratio – the cardiothoracic ratio (c t r )is greater than 50% cardiomegaly is present. Cardiomegaly takes on two basic forms based on the overall shape of the heart; the ovoid form (bottom left) suggests left ventricular dominance and triangular form (bottom right) which suggests right ventricular dominance.
Ashley Davidoff MD
The Ovoid Form of Cardiomegaly – Consider LVE

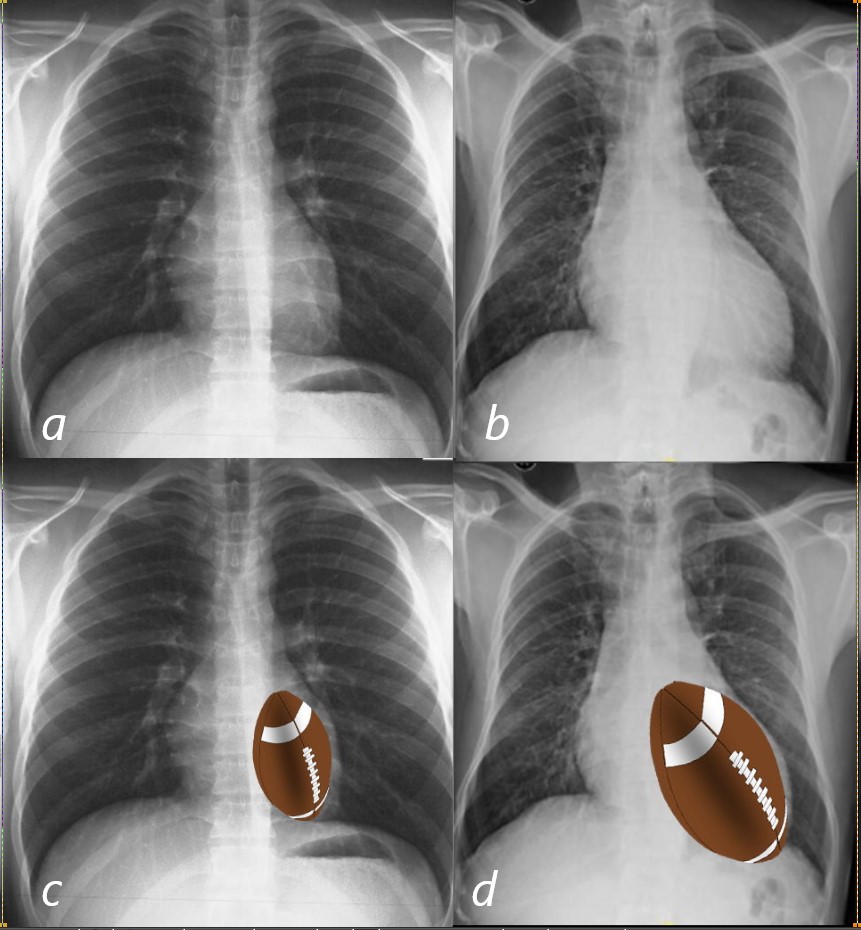
The enlarged LV (a,b) is shaped like an oval and it is likened to a rugby ball or an American football placed on the field at kick off time. LVE on CXR is mostly assessed by an increased cardiothoracic ratio as well as the accentuation of the ovoid shape. (lower images c, d,e, f)
Ashley Davidoff MD
Vector of the Enlarging LV – Rotate Down and to the Left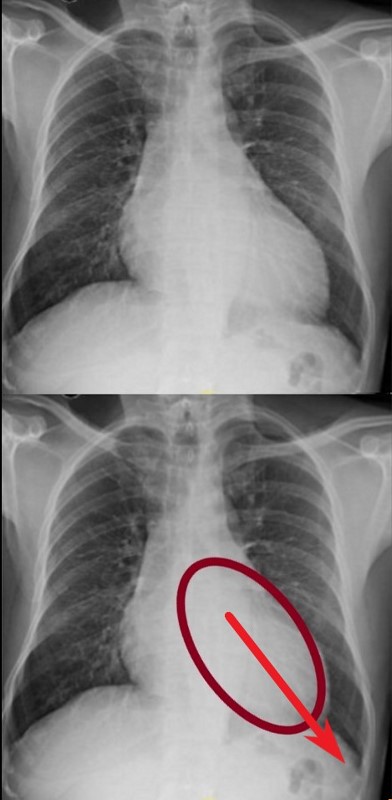 VECTOR FOR LV ENLARGEMENT
VECTOR FOR LV ENLARGEMENT
DOWN AND OUT
The left ventricle (LV) enlarges in a posterior, downward and lateral direction resulting in the characteristic changes of LVE on CXR
Ashley Davidoff MD
Clinical Exam – Focal LV Thrust

The left ventricle (LV) enlarges in a downward and lateral direction resulting in the apical impulse displacement and increase forcefulness of the apical tap.
Ashley Davidoff MD
The Triangular Form of Cardiomegaly – Consider RVE
71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
Ashley Davidoff MD
Note the Basic Shape of the RV in almost all Views

The enlarged LV (a,b) is shaped like an oval and it is likened to a rugby ball or an American football placed on the field at kick off time. LVE on CXR is mostly assessed by an increased cardiothoracic ratio as well as the accentuation of the ovoid shap. (lower images c, d,e, f)
Ashley Davidoff MD
Vector of the Enlarging RV – Rotate Laterally to the Right
ANTERIOR LEFTWARD
The right ventricle (RV) enlarges with a clockwise rotation resulting in an upward turning of the apex and enlargement in a anterior and leftward lateral direction.
Ashley Davidoff MD
As the right ventricle (RV) enlarges with a clockwise rotation the apex of the small ventricle succumbs to the larger silhouette of the RV which pints upward and to the left and has been called the “proud breast” appearance.
Ashley Davidoff MD

Ashley Davidoff MD
Clinical Exam – Parasternal Heave
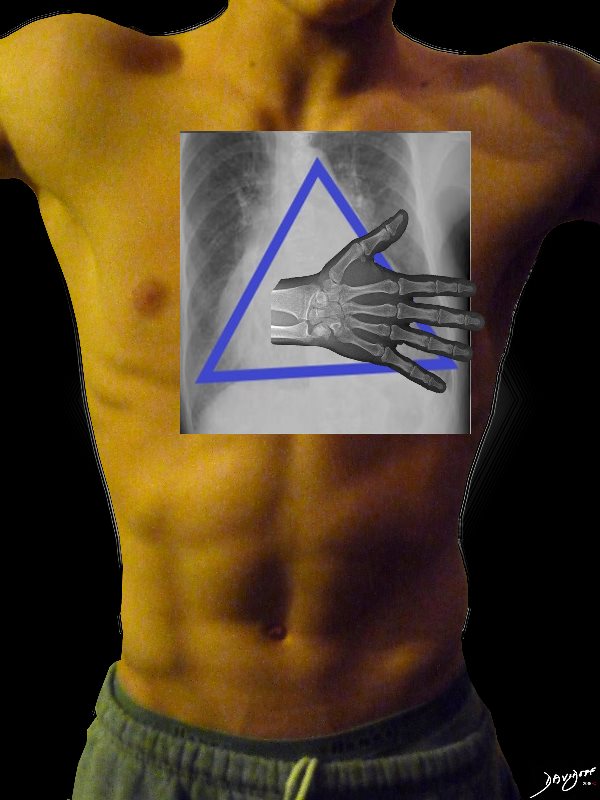
The right ventricle (RV) enlarges in a anterior, upward and lateral direction resulting in the broad based parasternal pulsation which on clinical examination is identified as a parasternal heave identified with the base of the extended hand
Ashley Davidoff MD
What about the Right Atrium (RA) and Right Heart Border?
The RA does not make much a statement on the frontal CXR
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.
Ashley Davidoff MD
The right atrium is the most difficult chamber to assess unless it is very large in which case it will present on the frontal CXR with a very large right paravertebral border.
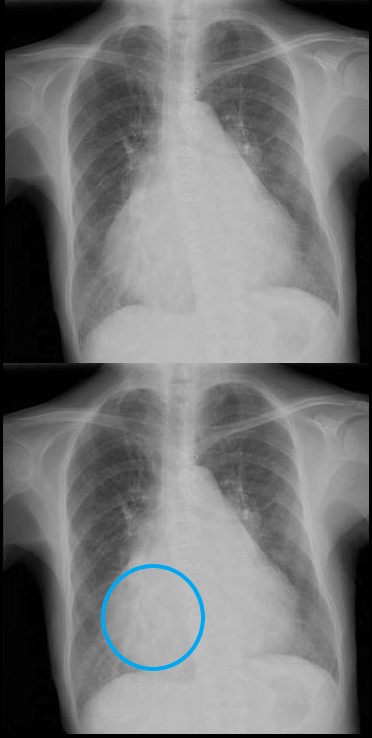
The right atrium is the most difficult chamber to assess unless it is very large in which case it will present on the frontal CXR with a very large right paravertebral border. This is a 71 year old female person with rheumatic heart disease with pulmonary hypertension and tricuspid regurgitation hence resulting in a large right atrium (RAE)
Ashley Davidoff MD

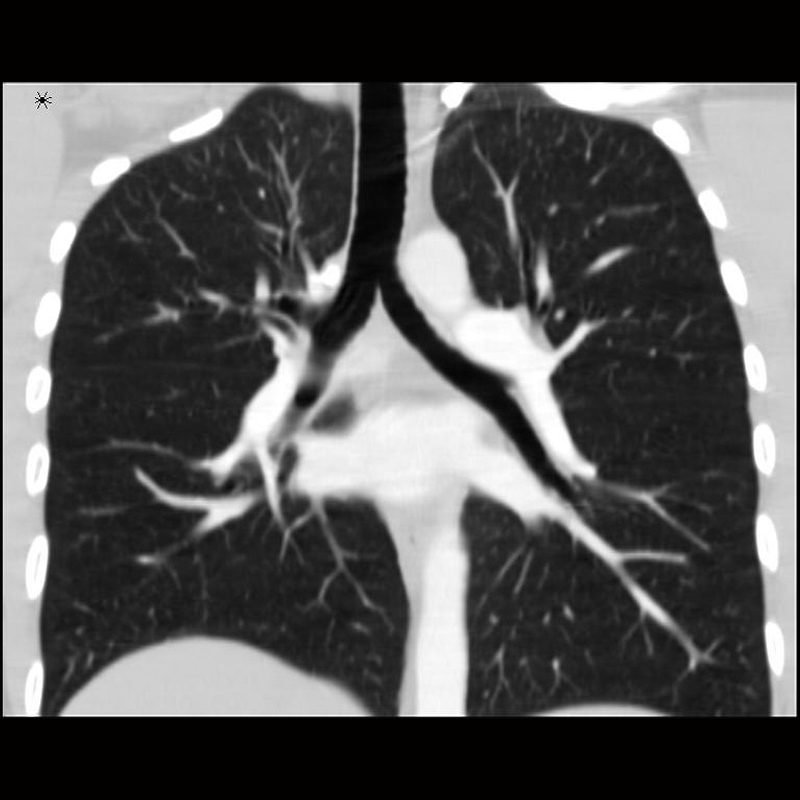
The right atrium is the most difficult chamber to assess unless it is very large in which case it will present on the frontal CXR with a very large right paravertebral border. The frontal CXR and coronal CT through the RA is from a 71 year old female with rheumatic heart disease with pulmonary hypertension and tricuspid regurgitation resulting in a giant right atrium (RAE). The RA accounts for the large bulge of the right border of the cardiac silhouette. The black arrowhead in the loer image points to the calcified mitral valve.
Ashley Davidoff MD
The Left Atrium
3 signs
-
- Carinal Angle
- Double Density
- Filling in of the Left Atrial Appendage Bay
The Carina and the Carinal Angle
 NORMAL FRONTAL CXR NORMAL ASYMMETRIC BRANCHING OF MAINSTEM BRONCHI
NORMAL FRONTAL CXR NORMAL ASYMMETRIC BRANCHING OF MAINSTEM BRONCHI
The normal CXR shows the characteristic asymmetric branching of the main stem bronchi. The right is short and stout and slightly more vertical while the left is long and thin and slightly more obtuse.
The normal carinal angle is between 40-80 degrees.
Ashley Davidoff MD
 ASYMMETRIC BRANCHING PATTERN ? RIGHT SHORT AND STOUT AND THE LEFT LONG AND THIN
ASYMMETRIC BRANCHING PATTERN ? RIGHT SHORT AND STOUT AND THE LEFT LONG AND THIN
CARINAL ANGLE ? 40-80 degrees
Ashley Davidoff MD
The Abnormal Carinal Angle

A dancer demonstrates a normal carinal angle (upper image) and as she continues to extend her left leg, (lower images) the angle becomes greater than 80 degrees and in terms of the carinal angle becomes abnormal.
Ashley Davidoff MD

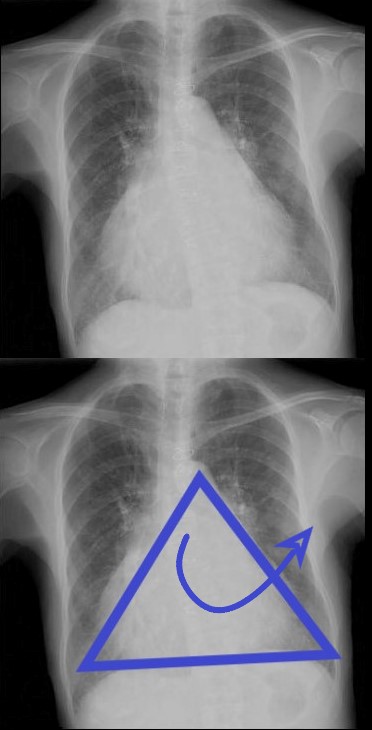
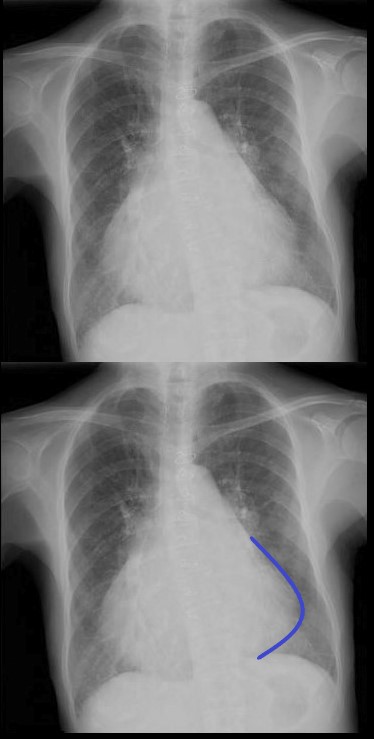
The frontal CXR demonstrates findings consistent with mitral stenosis including a widened carinal angle (teal blue and black arc), a double density (red arc) and an enlarged left atrial appendage (maroon arc).
The overall shape of the heart is triangular suggesting right ventricular enlargement. A mitral valve prosthesis is in position
Courtesy of Radiopaedia
71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
The frontal view shows an enlarged RA (light blue) characterized by a prominent right heart border. The right ventricle is enlarged as noted by the triangular shape of the cardiac silhouette, an the upturned (“proud breast”) appearance of the left heart border, both reminiscent of RVE. The left atrium is also significantly enlarged characterised by the widened carina and the straight heart border caused by a combination of atrial appendage enlargement and pulmonary hypertension. The LV (maroon) is normal in size
Ashley Davidoff MD
Shapes of the Heart in Congenital Heart Disease
|
Shapes of the Heart in Congenital Heart Disease on CXR |
| 1 = normal heart 2 = LV enlargement 3 = RV enlargement 4 large mediastinum = snowman TAPVR 5 = small mediastinum = D?TGA TA Pulmonary atresia 6 = pulmonary bay P Atresia Tetralogy truncus TGA Coronal LTGA is 07197 heart shape cardiac CXR plain films Some of the images have been downloaded from the web with sources unknown and are used for education purposes alone 86774 s |
|
The Shapes of the Heart in Health and Disease |
|
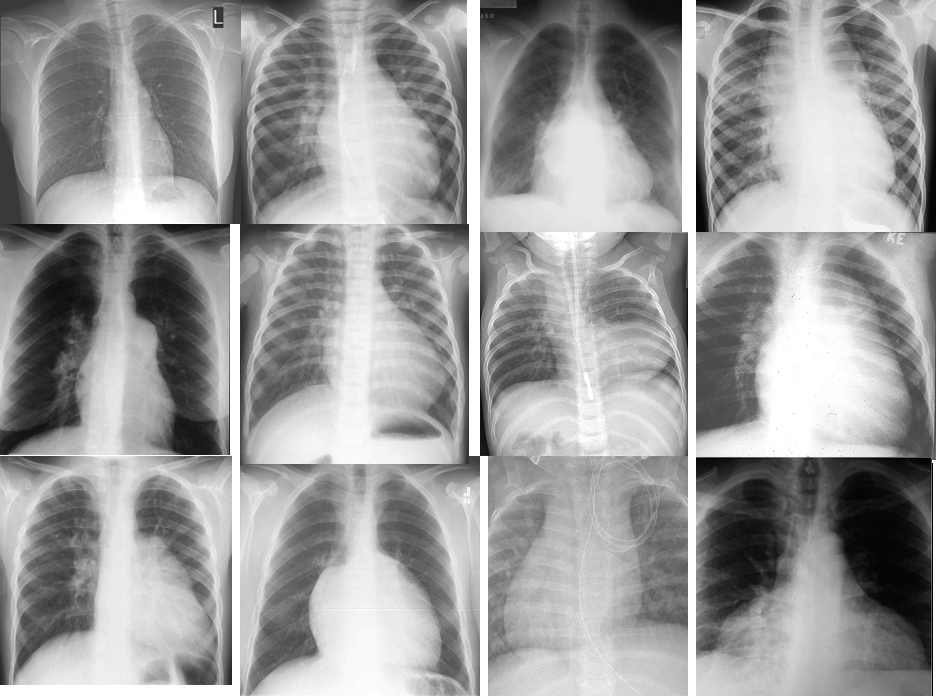
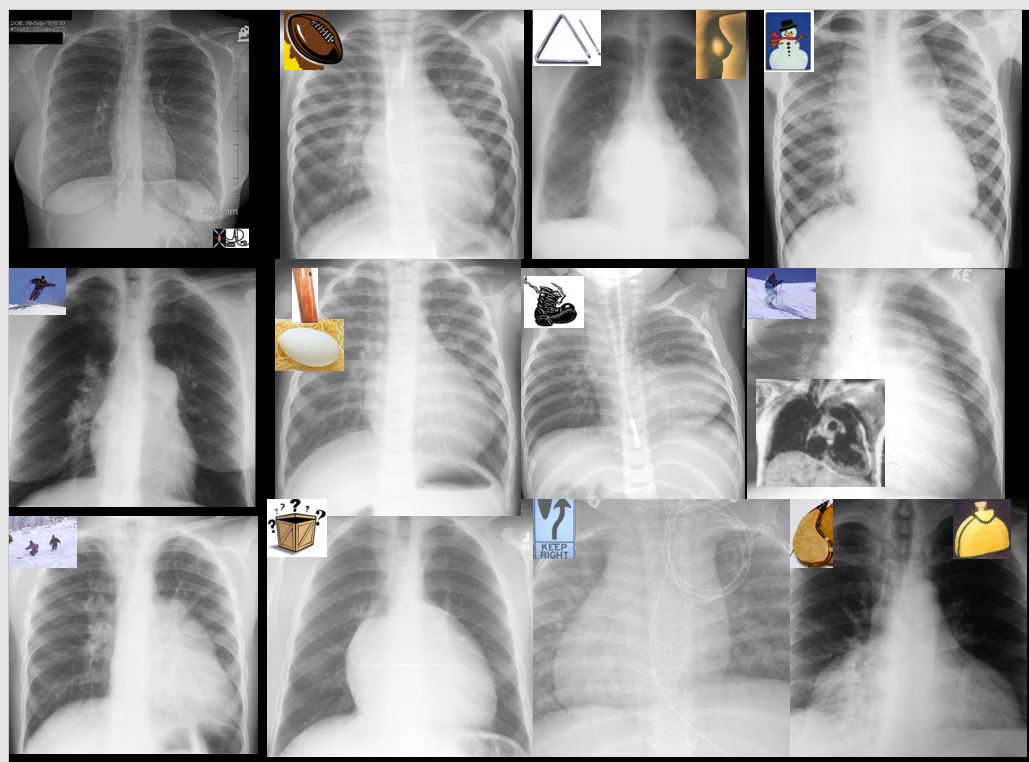
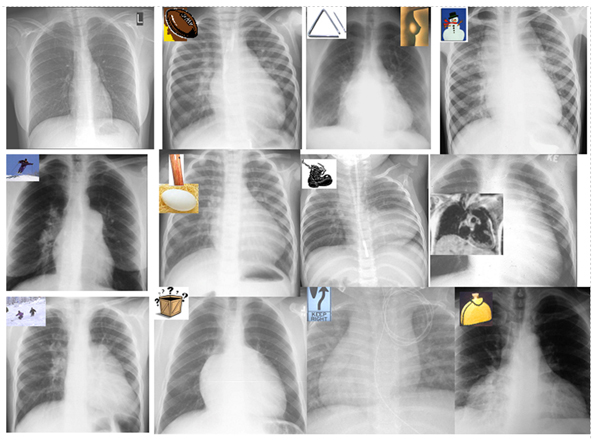
The collage of frontal views of the heart is a combination of images from a personal collection and borrowed from the internet for educational purposes only. From top left and across the rows they are The normal heart , the ?football? of LV enlargement the ?triangle? or ?proud breast? of RV enlargement, ?snowman? of total anomalous pulmonary venous return, ?egg on its side? of D transposition of the great vessels, the big mogul of skiing down the left heart border in pulmonary stenosis or pulmonary hypertension, ?boot shaped? heart seen in both pulmonary atresia and Tetralogy of Fallot, the long smooth mogul that has a differential diagnosis of L transposition, absence of the pericardium, and juxtaposition of the atrial appendages, the box shaped large heart of Ebstein?s anomaly, the D loop where the genetic instruction of keep right ? seems likely, and the water bottle? heart of a large pericardial effusion. 07197 Some of the images have been downloaded from the web with sources unknown and are used for educational purposes alone 86774b02 |

Assessing Chamber Involvement

71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
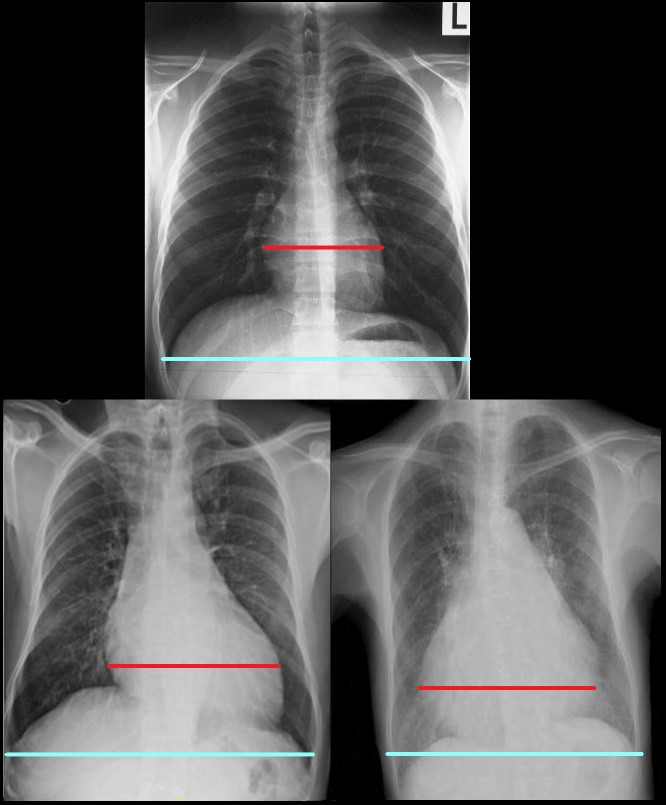
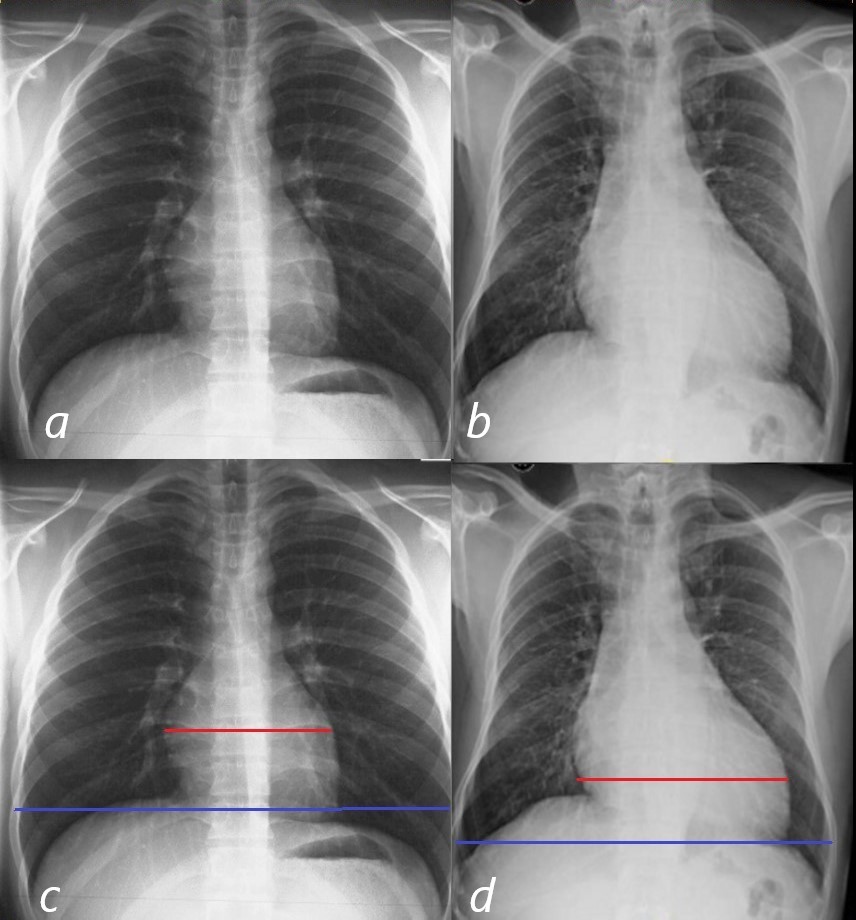
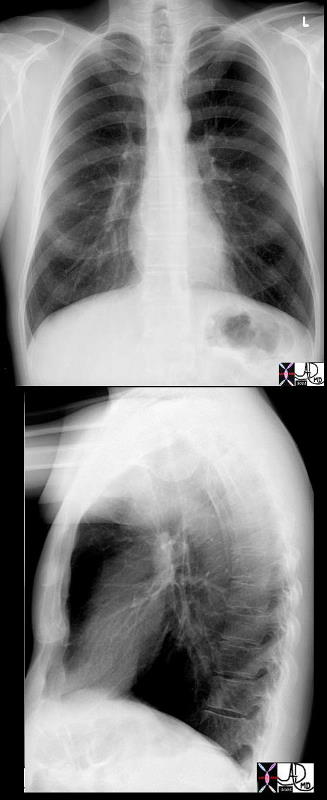
The lateral examination (a, and b) show normal ratios of the length of the retrosternal air space, (upper anterior white line 2/3, and normal 1/3 length of the anterior RV border (blue line).
In images c and d the anterior overlay shows an increase in the ratio of the RV (navy blue-line to the upper 2/3 of the retrosternal space (white line) indicating RVE. Posteriorly, there is an increase ratio of the distance between the upper left atrial length (red – of posterior border of the left atrium (LA) and the lower border of the LV (white line) indicating LAE. In addition the straight left main bronchus (b – teal arrow) is shifted upward and is almost horizontal (d teal arrowhead) indicating LAE. Inferiorly the ratio of the length of the LV (maroon line) when compared to the rest of the diaphragm (white) is normal , indicating no evidence of LVE
Ashley Davidoff MD
The Ovoid Cardiomegaly
The cardiothoracic ratio as measured on a PA chest x-ray, is the ratio of maximal horizontal diameter of the heart to maximal horizontal diameter of the inner edge of the thoracic cage. The normal ratio is less than .5
In this instance images a and d show a ratio that is less than .5 and heart size is considered normal. Images b and d are abnormal since the ratio is greater than .5 and by virtue of the shape of the heart LV enlargement is suggested
Ashley Davidoff MD
Be Careful – Good Inspiration vs Poor Inspiration

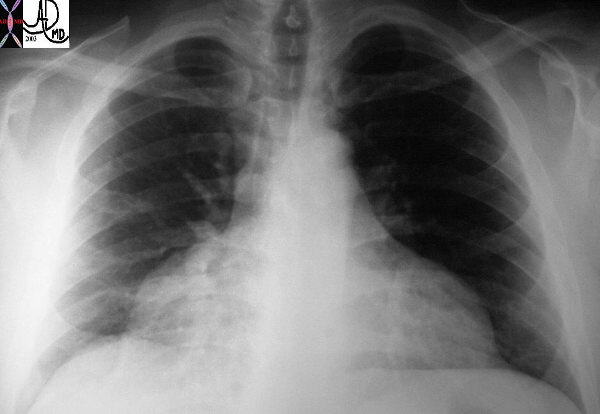
This a normal frontal chest X Ray of a 40 year old male with a good inspiration.
Ashley Davidoff MD
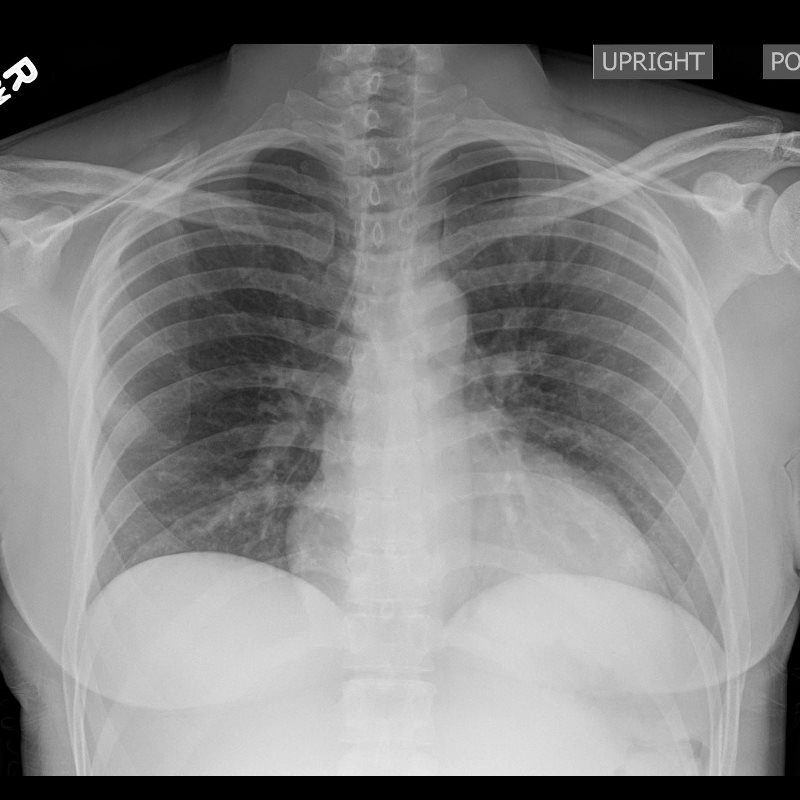
This a normal frontal chest X ray of a 40 year old male with a poor inspiration which results in the false appearance of cardiomegaly and crowding of the lung markings.
Ashley Davidoff MD
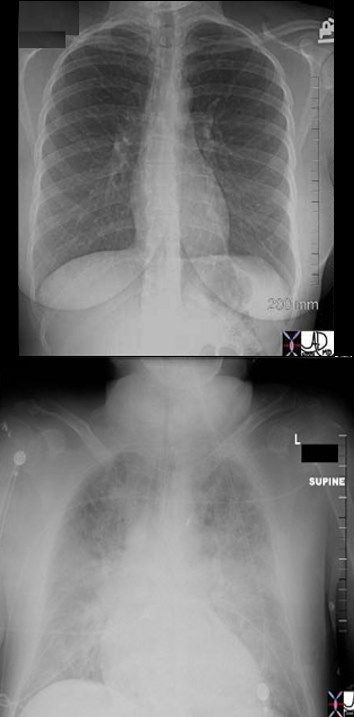
 CXR- NORMAL and MITRAL STENOSIS
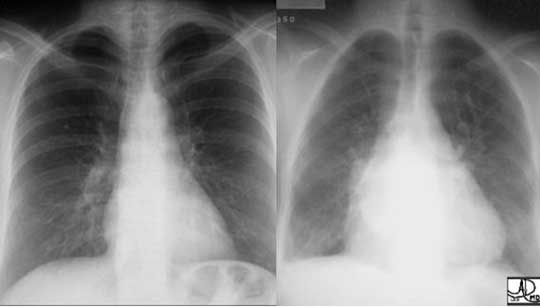
CXR- NORMAL and MITRAL STENOSIS
Two different patients showing the normal patient on the left and the CXR of a patient with an enlarged triangular shaped heart on the right. The triangular heart with upturned apex is characteristic of right ventricular enlargement, and the elevation of the carina and a double density seen on the right side of the heart suggests left atrial enlargement. These findings are consistent with rheumatic mitral stenosis.
Ashley Davidoff MD
Small Heart
The P-A view of the chest shows hyperinflated lung volumes. Note that more than 10 posterior ribs can be visualized. The lateral view of the chest shows hyperinflated lung volumes in this patient with acute asthma, characterized by flattening of the hemidiaphragms and increased aeration of the retrosternal air space.
Courtesy of Ashley Davidoff M.D
Shapes of the Heart
The Left Ventricle
The LV is ovoid in shape and points toward the left. It also assumes the shape of a football or rugby ball. When it enlarges it enlarges downward and to the left as well as posteriorly.
Ashley Davidoff MD
32079 shape LV
Shape of the Heart
The LV is oval in shape and when it enlarges it advances down and leftward and posteriorly. The oval shape is reminiscent of a rugby ball or a football.
In this instance images a and show a normal shape and size of the left side of the heart . Images b and d are abnormal The heart is enlarged and shows downward and leftward vector
Ashley Davidoff MD
30397 b03L
The Right Ventricle
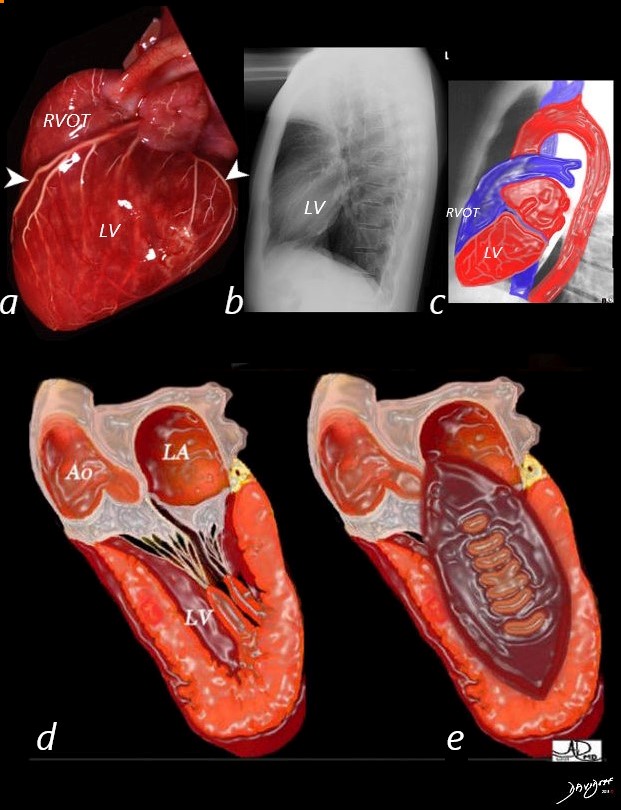
A lateral projection of an anatomic specimen of a normal heart with coronary barium angiogram (a) shows the posterior positioning of the LV in relation to the right ventricular outflow tract (RVOT) (“backroom boy”)
The front arrowhead points to the LAD and the back arrowhead points to the 3 rd obtuse marginal artery.
The lateral CXR of a normal heart (b) and correlative diagram (c) exemplifies the posterior positioning of the LV in relation to the RVOT.
The artistic rendition of the LV (d) demonstrates the “all muscle” concept, while the football ovoid shape of the LV pointing down and leftward (d) demonstrates the “loves football” concept
Ashley DAvidoff MD
32079 buzz LV.8
The artistic rendition of the right atrium and right ventricle. The spatial relationship is best viewed conceptually by tacking the thumb of your right hand and placing it in the middle of the right atrium, and your palm will be aligned with the RVOT
Davidoff art Courtesy Ashley Davidoff copyright 2019 06566b12b13.4kb05i.8s
With a black triangle for a nose and a white spot for the eye, Snoopy’s face becomes real – you almost want to pet the beagle like face.
Ashley Davidoff MD 32084
Ashley Davidoff MD
heart-0078

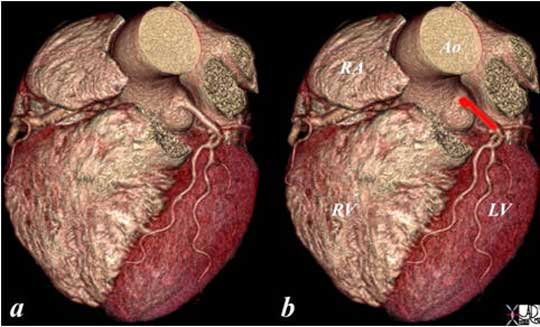
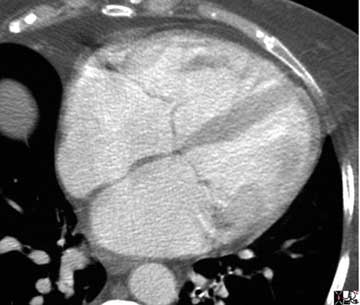
This is an external and frontal view of the heart. The vessel that you see coursing straight down the center of the heart is the left anterior descending artery, (LAD) that runs anterior to the ventricular septum (vertical limb of the cross) separating the right and left ventricles. Conceptualize the triangular shape of the right ventricle, and the ovoid almost football shape of the left ventricle.
Courtesy of Ashley Davidoff M.D. 32078
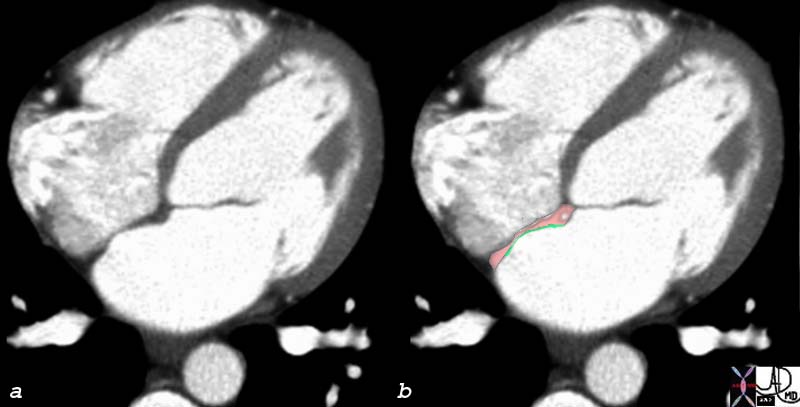
The volume rendering of the normal left main coronary artery (red overlay) is seen in image (b). The left atrial appendage and right ventricular outflow tract have been digitally removed to expose the left main coronary artery.
Courtesy: Ashley Davidoff, M.D.
76287c01 heart cardiac atrial septum septum primum fossa ovalis bulging septum primum (green) LV left ventricle MV mitral valve open diastole diastolic phase atrial septum normal anatomy
CTscan
Courtesy Ashley Davidoff MD
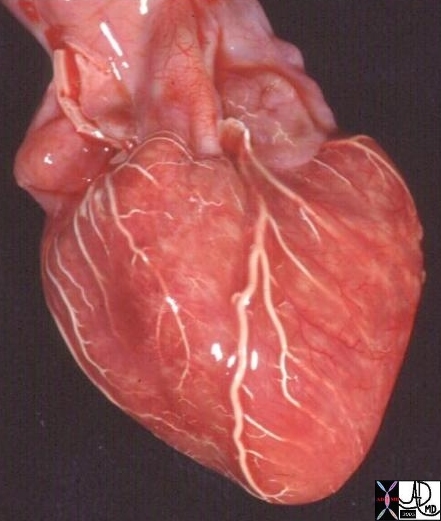
15009c cardiac heart coronary artery normal anatomy gross pathology LAD diagonal artery acute marginal artery conal artery arc of Vieussens Courtesy Ashley Davidoff MD
15009c

X-ray shows the typical appearance of a “water bottle heart? characteristic of a pericardial of a large pericardial effusion.
Ashley Davidoff MD

X-ray shows the typical appearance of a “water bottle heart? characteristic of a pericardial of a large pericardial effusion.
Ashley Davidoff MD
In Congenital Heart Disease
The collage of frontal views of the heart is a combination of images from a personal collection and borrowed from the internet for educational purposes only. From top left and across the rows they are: the normal heart , the “football” of LV enlargement, the “triangle” or “proud breast” of RV enlargement, “snowman” of total anomalous pulmonary venous return, the big mogul of skiing down the left heart border in pulmonary stenosis or pulmonary hypertension, “egg on its side” of D transposition of the great vessels, “boot shaped” heart seen in both pulmonary atresia and Tetralogy of Fallot, the long smooth mogul that has a differential diagnosis of L transposition, absence of the pericardium, and juxtaposition of the atrial appendages, the box shaped large heart of Ebstein’s anomaly, the D loop where the genetic instruction of keep right ” seems likely, and the water bottle” heart of a large pericardial effusion. Courtesy of: Ashley Davidoff, M.D.

Ashley Davidoff MD

The PA chest X-ray shows the apex pointing rightward and most of the heart is in the right chest. Note also that the stomach bubble is in normal position, and so situs solitus is present. This is a case of isolated dextrocardia, caused by an arrest of development, and not associated with situs inversus, but subject to a higher incidence of other congenital anomalies.
Ashley Davidoff, M.D.

The CXR and bronchogram is from a 30-year-old male who presents with a long standing history of a productive cough, sinus headaches, and infertility. The bronchogram shows inversion of the bronchi with the long thin bronchus characteristic of the left bronchus being right sided and short “fat ” bronchus characteristic of the right being left sided. Situs inversus and dextrocardia exist. However the history of sinusitis and infertility make the diagnosis of Kartagener’s syndrome likely.
Ashley Davidoff, M.D.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CXR ? NORMAL AND PULMONARY EDEMA
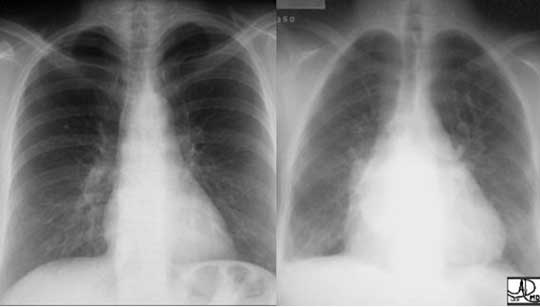
Normal (upper)and Pulmonary Edema (lower)
The patient with acute myocardial infarction may have a normal chest examination but if there is extensive myocardial damage to impede pump function, pulmonary edema (right) results.
Courtesy of: Ashley Davidoff, M.D.
Links and References
TCV and
Basic Approach to the CXR – TCV
CXR and CHF
CXR Technique
Right Atrium
Right Ventricle
Pulmonary Artery
Left Atrium
Left Ventricle
Aortic Valve
Aorta
References and Links