Ebsteins Anomaly is a congenital disorder of the tricuspid valve and right ventricle caused by a failure of the normal resorbtion of the posterior and septal leaflets of the tricuspid valve from the posterior right ventricular wall, structurally resulting in adherence of the posterior leaflet posteriorly and caudally to the RV apex, associated with a large sail like maloriented anterior leaflet associated with abnormal chordae and chordal attachments.
The muscular wall of the posterior wall of the right ventricle is often abnormal and thinned, 9Uhl’s anomaly) and is considered atrialized, since structurally it appears to be part of the right atrium, but its EKG tracing is clearly ventricular. The rest of right ventricle is a small portion of the right ventricular sinus and right ventricular outflow making the functioning right ventricle small. Associated findings that sometimes occur include pulmonary stenosis, RVOT stenosis, PFO,ASD, and Wolf Parkinson White Syndrome.
The tricuspid valve can be stenotis normal functioning or regurgitant.
Ebsteins is mostly a right sided lesion but on rare occasions in the setting of corrected transposition, left sided Ebsteins is possible.
The structural deficiences are classified according to Carpentier’s Classification.
? Type A = RV volume is adequate
? Type B = large atrialized segment of RV; mobile anterior leaflet
? Type C = restricted movement of anterior leaflet; may cause infundibulum obstruction
? Type D = near-complete atrialization of the RV (Uhl’s syndrome)
Functionally the effects are dependant on the functioanl status of the tricuspid valve abd the presence of associated anomalies such as PFO ASD right ventricular outflow stnosis
Clinically these patients can present at birth in severe right sided failure if the tricuspid regurgitation is severe, or may present cyanotic if the outflow tract is stenotoc and there is right to left shunting through the ASD or PFO.
If the arrhythmias are a prominent part of the disease process then the patient can present with paroxysmal tachycardia, Wolff-Parkinson-White Syndrome.
If the patient presents in the first week of life the prognosis is usually poor. heart failure, sudden death, and paradoxical emboli are the three most common causes of death
The diagnosis is based on the the presence of tricuspid valve dysfunction, arrhyhmias. or cyaniosis. The auscultation may be typical with a loud early systolic sail sound caused by a flap of the large sail like anterior leaflet.
Imaging shows a lassical box shaped enlarged heart on CXR, with typical echocardiographic findings of a deformed tricuspid valve, posterior leaflet adherent to a thin posterior right ventricle, large sail like anterior leaflet, that may be regurgiant, normal or stenotic.
Medical treatment in the neonatal period includes PGE for the neonate in extremis, with supportive care of cyanotic infants. Indications for surgery include severe tricuspid valve regurgitation, moderate to severe cyanosis with polycythemia
, NYHA class III or IV congestive failure, massive cardiomegaly, or arrhythmias.
Surgery involves repair or replacement of the tricuspid valve, closure of the ASD.
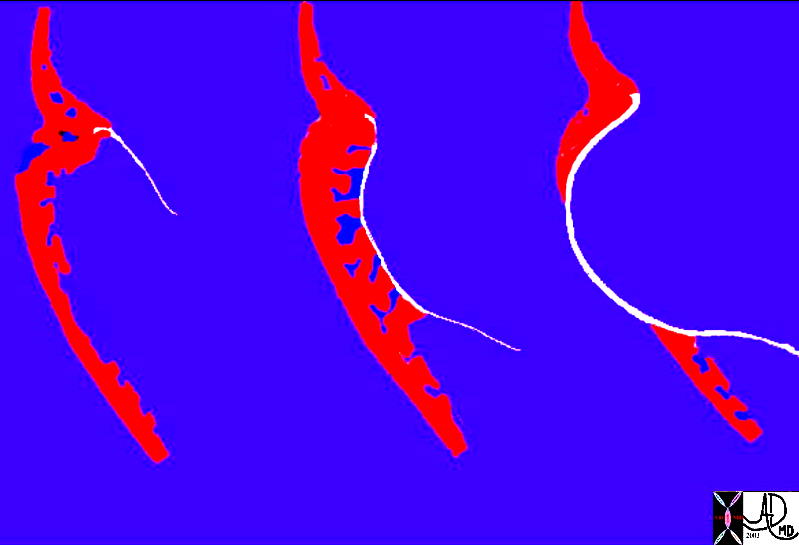
This image reflects the RV and the large anterior leaflet of the tricuspid valve in this pathologic specimen of Ebstein’s anomaly. The valve orifice is also maloriented in that it is directed cranially tothe RVOT rather than to the apex and body of the RV. Courtesy Ashley Davidoff MD. 01506 code cardiac heart RV Ebsteins anomaly TV large sail anterior leaflet congenital grosspathology
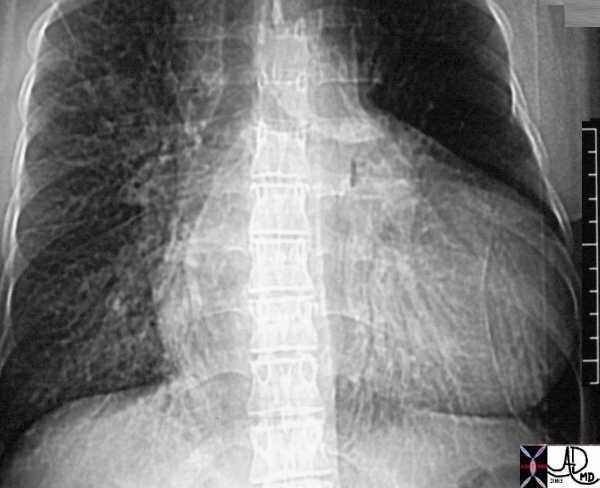
This large, box shaped heart is classical for Ebsteins anomaly, which is dominantly associated with a large right atrium Courtesy Ashley Davidoff MD 01486 code heart cardiac large box-shape Ebstein?s imaging radiology CXR plain film disease
20023
This 25 year old female has a very large heart which is almost rectangular in shape. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20023 code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
20019 20022
This young patient has a very large heart which is almost rectangular in shape, characterised by significant enlargement of the right atrium and coronary sinus with ground glass changes suggesting CHF. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20019 code heart right atrium (RA) coronary sinus fx enlarged box shape congestion dx Ebsteins anomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
32101
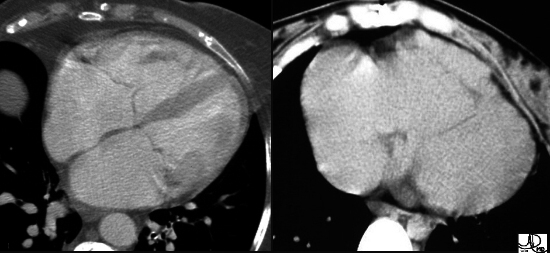
These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow. Can you identify RA and TV? – see next image if you need help.
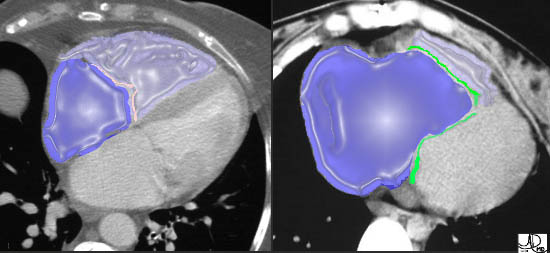
In both images, the RA is in royal blue overlay and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly.
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
32101
These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow. Can you identify RA and TV? – see next image if you need help.
In both images, the RA is in royal blue overlay and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly.
Courtesy of Ashley Davidoff M.D. 32101 32102
code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
32101
These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow. Can you identify RA and TV? – see next image if you need help.
In both images, the RA is in royal blue overlay and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly.
Courtesy of Ashley Davidoff M.D. 32101 32102
code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow. Can you identify RA and TV? – see next image if you need help.
In both images, the RA is in royal blue overlay and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly.
Courtesy of Ashley Davidoff M.D. 32101 32102
code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow. Can you identify RA and TV? – see next image if you need help.
In both images, the RA is in royal blue overlay and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly.
Courtesy of Ashley Davidoff M.D. 32101 32102
code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
32101
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
32101
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
20019 20022
This young patient has a very large heart which is almost rectangular in shape, characterised by significant enlargement of the right atrium and coronary sinus with ground glass changes suggesting CHF. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20019 code heart right atrium (RA) coronary sinus fx enlarged box shape congestion dx Ebsteins anomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
20019 20022
This young patient has a very large heart which is almost rectangular in shape, characterised by significant enlargement of the right atrium and coronary sinus with ground glass changes suggesting CHF. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20019 code heart right atrium (RA) coronary sinus fx enlarged box shape congestion dx Ebsteins anomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This young patient has a very large heart which is almost rectangular in shape, characterised by significant enlargement of the right atrium and coronary sinus with ground glass changes suggesting CHF. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20019 code heart right atrium (RA) coronary sinus fx enlarged box shape congestion dx Ebsteins anomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This young patient has a very large heart which is almost rectangular in shape, characterised by significant enlargement of the right atrium and coronary sinus with ground glass changes suggesting CHF. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20019 code heart right atrium (RA) coronary sinus fx enlarged box shape congestion dx Ebsteins anomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
20019 20022
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
20019 20022
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
20023
This 25 year old female has a very large heart which is almost rectangular in shape. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20023 code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
20023
This 25 year old female has a very large heart which is almost rectangular in shape. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20023 code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This 25 year old female has a very large heart which is almost rectangular in shape. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20023 code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This 25 year old female has a very large heart which is almost rectangular in shape. The pulmonary vessels, particularly at the right base are enlarged and congested. This patient has Ebstein’s anomaly. Courtesy Ashley Davidoff MD. 20023 code heart right atrium (RA) coronary sinus fx enlarged box shape lung pulmonary congestion dx dx Ebsteins anaomaly cardiac imaging radiology CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
20023
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
20023
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
01506
This image reflects the RV and the large anterior leaflet of the tricuspid valve in this pathologic specimen of Ebstein’s anomaly. The valve orifice is also maloriented in that it is directed cranially tothe RVOT rather than to the apex and body of the RV. Courtesy Ashley Davidoff MD. 01506 code cardiac heart RV Ebsteins anomaly TV large sail anterior leaflet congenital grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
01506
This image reflects the RV and the large anterior leaflet of the tricuspid valve in this pathologic specimen of Ebstein’s anomaly. The valve orifice is also maloriented in that it is directed cranially tothe RVOT rather than to the apex and body of the RV. Courtesy Ashley Davidoff MD. 01506 code cardiac heart RV Ebsteins anomaly TV large sail anterior leaflet congenital grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This image reflects the RV and the large anterior leaflet of the tricuspid valve in this pathologic specimen of Ebstein’s anomaly. The valve orifice is also maloriented in that it is directed cranially tothe RVOT rather than to the apex and body of the RV. Courtesy Ashley Davidoff MD. 01506 code cardiac heart RV Ebsteins anomaly TV large sail anterior leaflet congenital grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This image reflects the RV and the large anterior leaflet of the tricuspid valve in this pathologic specimen of Ebstein’s anomaly. The valve orifice is also maloriented in that it is directed cranially tothe RVOT rather than to the apex and body of the RV. Courtesy Ashley Davidoff MD. 01506 code cardiac heart RV Ebsteins anomaly TV large sail anterior leaflet congenital grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
01506
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
01506
)