
Heart failure with preserved ejection fraction (HFpEF).
Many causes
- Most common
- Aging
- Hypertension LVH
- Restrictive Cardiomyopathy
- Commonly caused by infiltration
- Structural Abnormality
- Thick Wall Small cavity
- Enlarged Left Atrium
- Physiology
- Low Cardiac Output
- Elevated End Diastolic Pressures
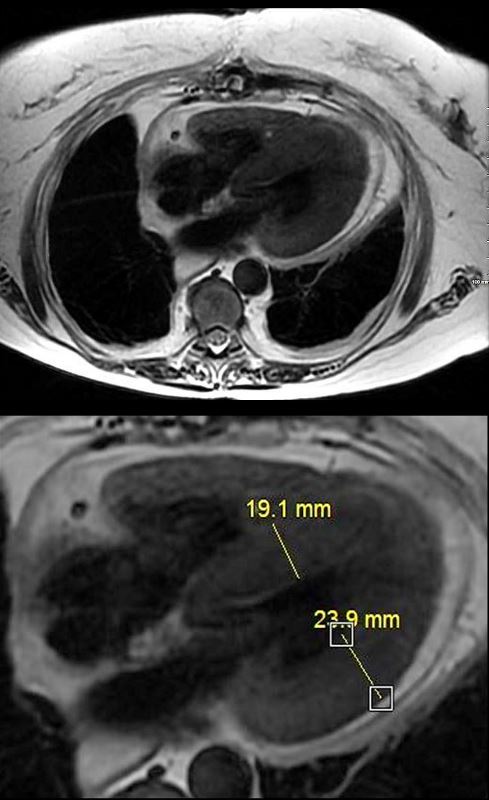
MRI with 4 chamber view from “black blood” T2 weighted imaging of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD
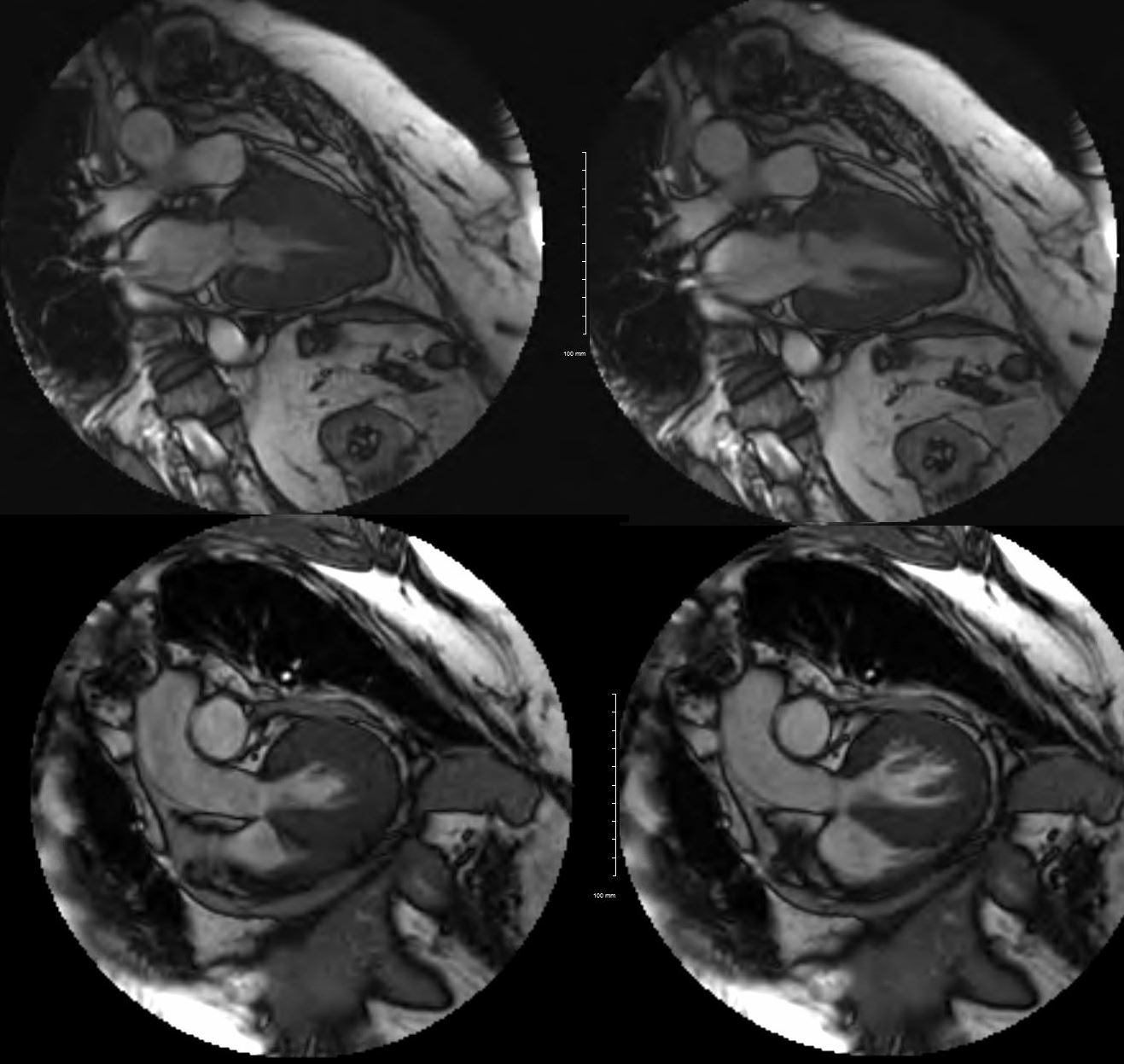
MRI with 2 chamber view in diastole of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. The images on the right are taken at peak systole and those on the left are peak diastole. It would appear that volume in the cavity at peak systole on both views is about 1/2 the original volume suggesting an EF of about 50%
Her cardiac Index was 2.8 L/min/m2 ( normal range for CI is 2.5 to 4 L/min/m2.) Her left atrium was normal in size
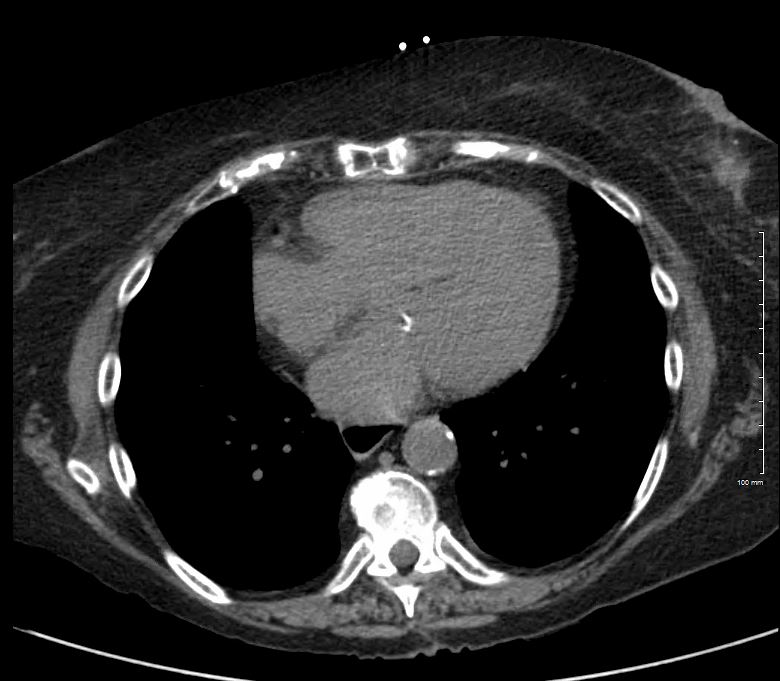
The axial image through the region of the AV valves shows normal sized atria. Constriction would be unlikely in the face of a normal sized right atrium. Note the flattened surface of the right atrium and all the signs of restrictive disease are not present including normal sized left atrium.
Ashley Davidoff MD
References and Links
Wiki
Radiopaedia