
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
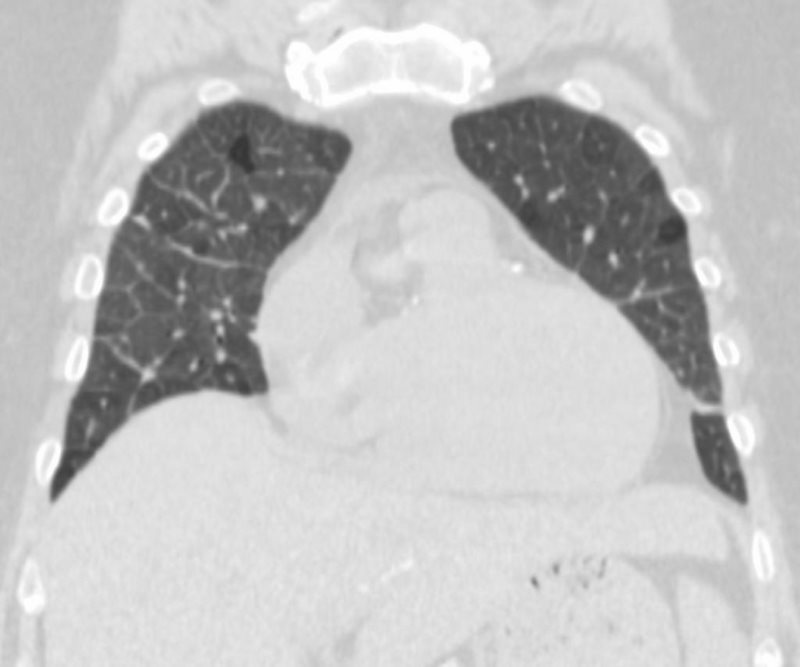
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
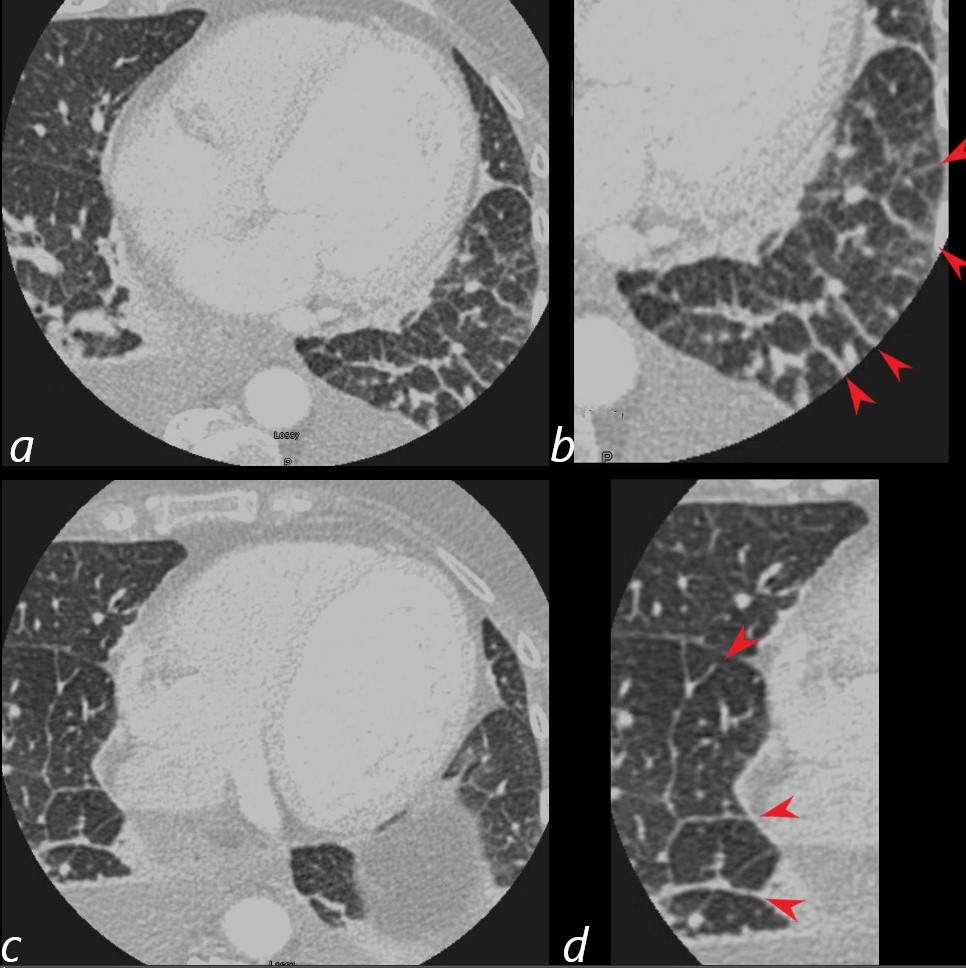
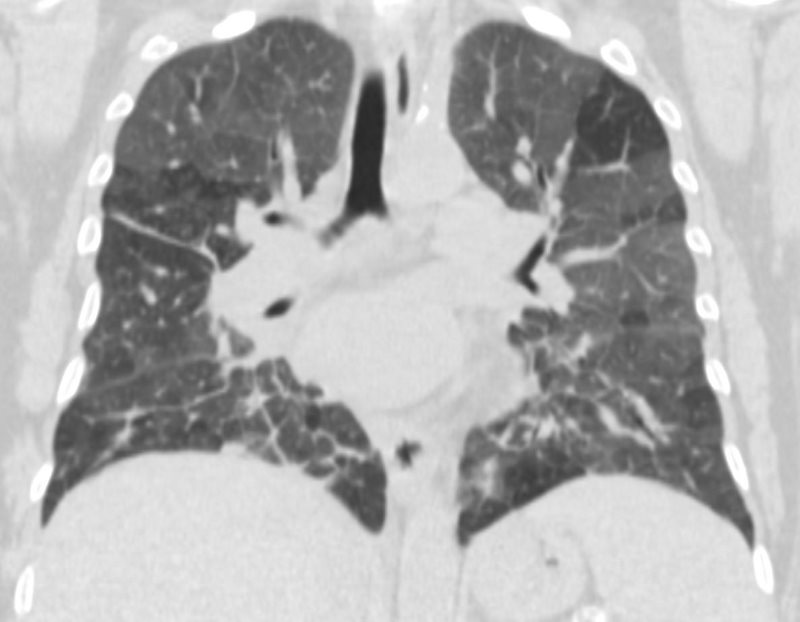
Lung windows confirmed the presence of prominent interlobular septa and LAE with bilateral complex effusions.
Ashley Davidoff MD
50-year-old male with CAD and CHF
The CXR showed LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
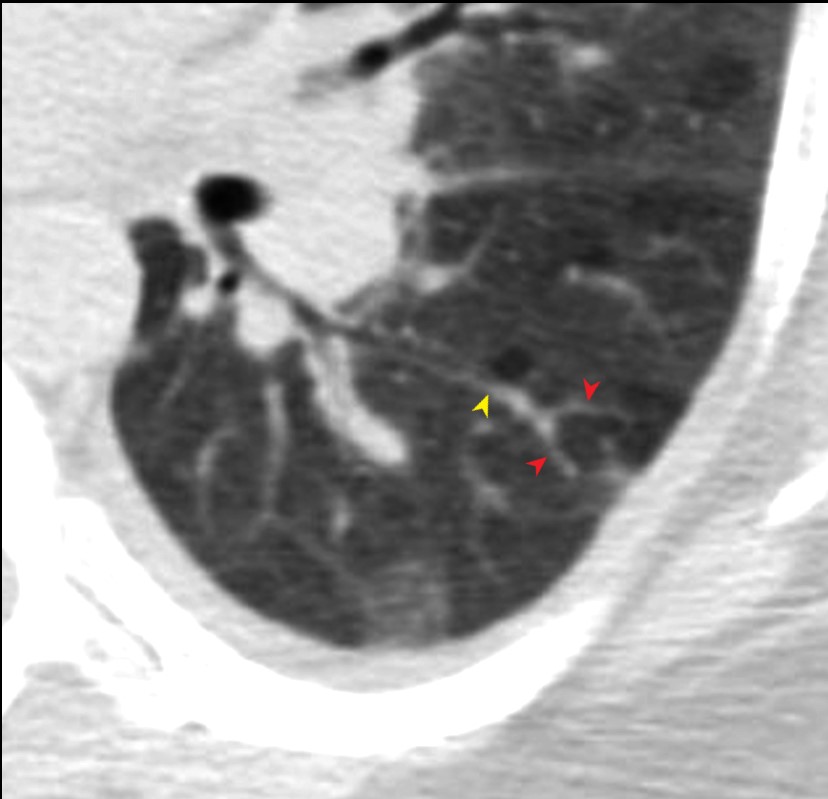
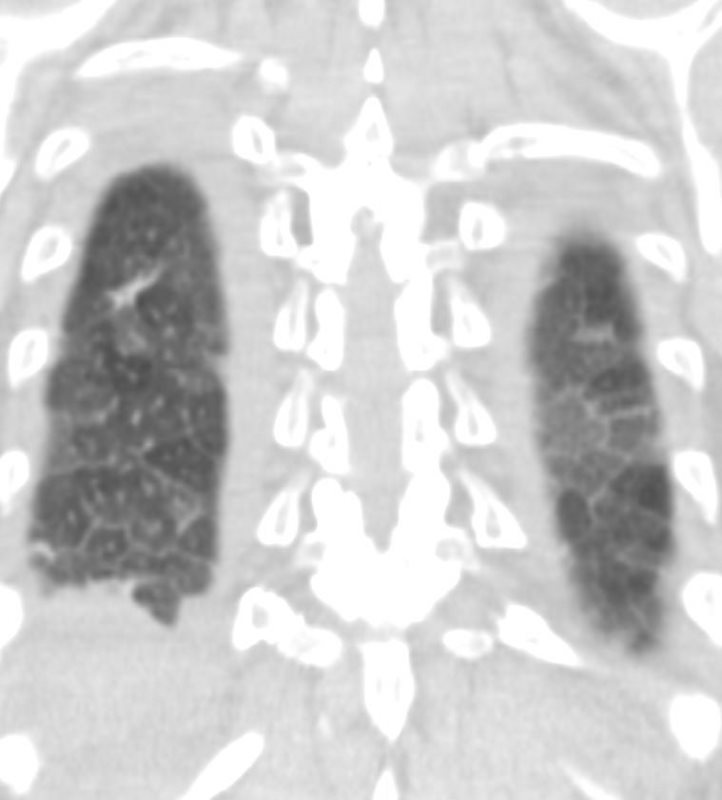
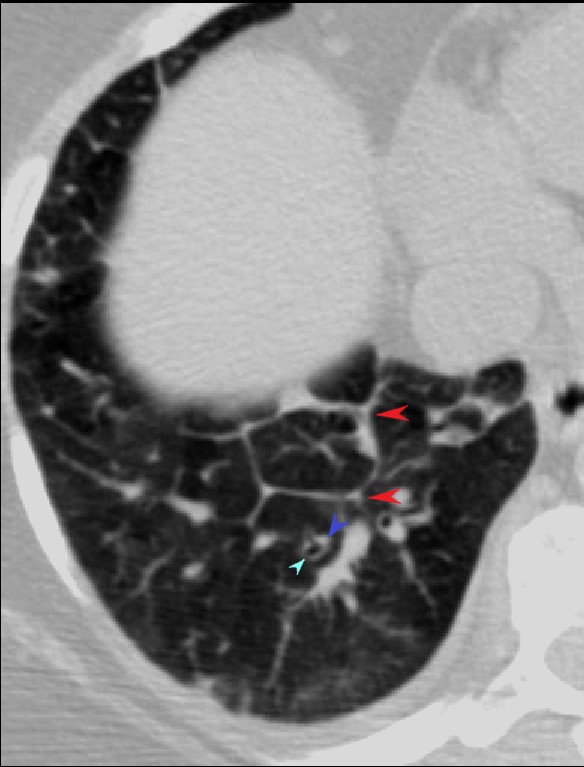
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
CHF, INTERSTITIAL EDEMA KERLEY A and B
Ashley Davidoff MD
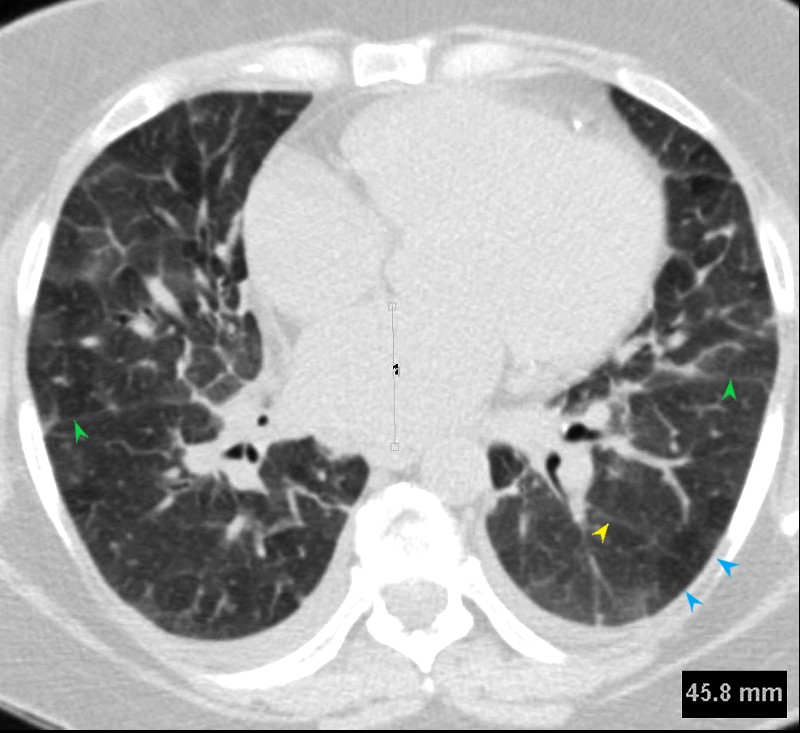
Fissures are indicated by the green arrows)
CHF, INTERSTITIAL EDEMA KERLEY A and B
Ashley Davidoff MD
Ashley Davidoff MD

Ashley Davidoff MD
50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD
50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD
CHF, INTERSTITIAL EDEMA KERLEY A and B
50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD
Acute Eosinophilic Pneumonia (AEP)can cause features reminiscent of interstitial edema due the extension of the inflammatory process into the Interstitium resulting in Kerley B lines and interstitial edema.