
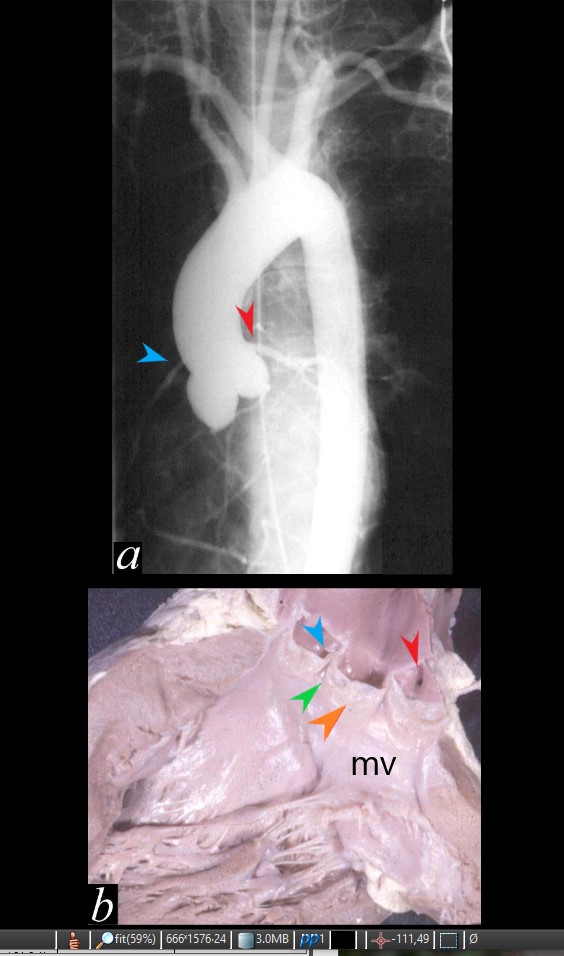
Aortogram in the LAO projection shows the inferior and rightward position of the RCA (blue arrow) and superior and leftward position of the LCA(red arrow)
Image b, shows the sinuses of Valsalva with right coronary ostium (blue) left coronary ostium (red) and non coronary cusp (orange). The membranous septum (green) lies between the right and non coronary cusp and the anterior leaflet of the mitral valve (mv) lies in fibrous continuity with the non and left coronary cusps
Ashley Davidoff MD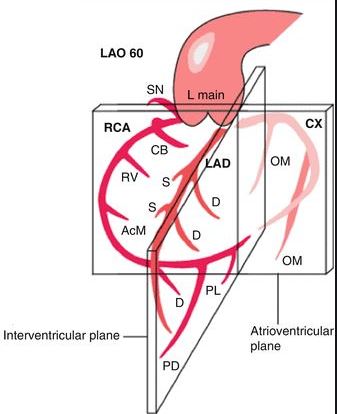
LCA in LAO
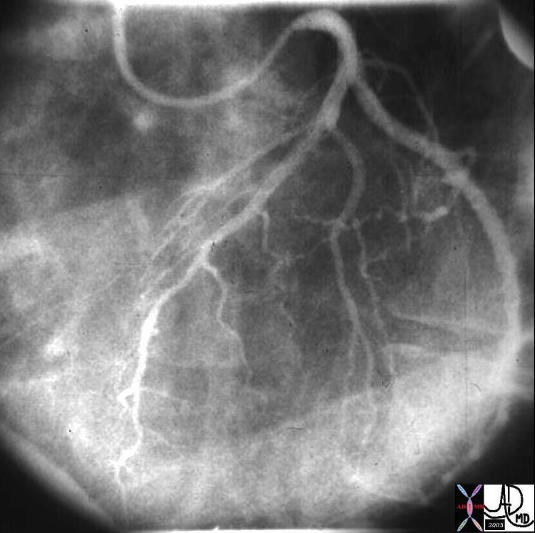
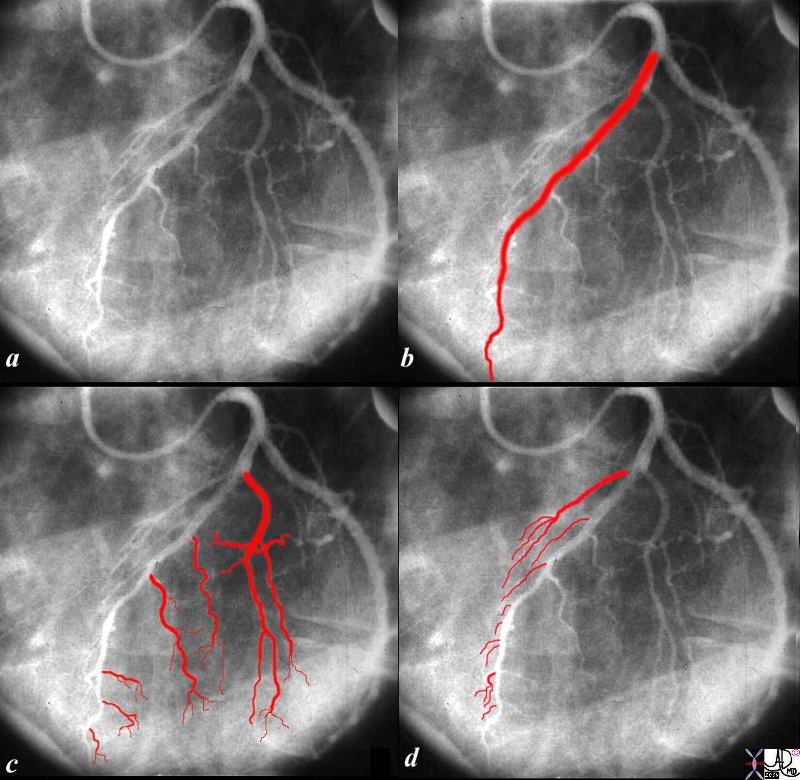
The angiogram of the left coronary artery in the LAO projection shows the LAD in b, diagonals in c and septal arteries coursing toward the diaphragm in d.
Ashley Davidoff MD

The left coronary angiogram is taken in the left anterior oblique projection showing the distal circumflex artery in (b) as a small tortuous almost insignificant vessel compared to the proximal circumflex.
The second marginal (2 in b) is so large that the distal circumflex seems insignificant. Since in this patient the RCA is dominant, the distal circumflex plays a small part in supplying the posterior and inferior portions of the LV.
The first obtuse marginal (1) overlaid in red in (c), arises from the anterior portion of the circumflex. The second obtuse marginal (2) is huge. The 3rd obtuse marginal (3) arises from the posterior portion of the circumflex artery. The last branch is a tiny posterior left ventricular artery. In (d) two small vessels are shown. The first, off the larger anterior portion is likely the S-A nodal artery and or left atrial branch, and the second arises from the smaller posterior portion and is a small left atrial branch.
Courtesy: Ashley Davidoff, M.D.
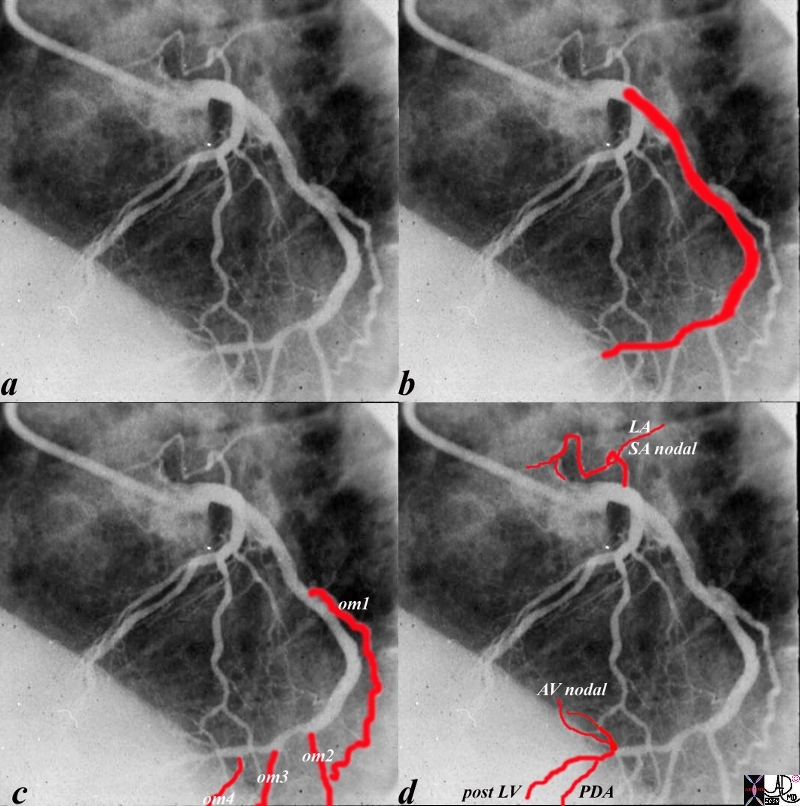
The angiogram of the LCA (a) shows the circumflex (b) arising from the left main coronary artery. In this left dominant system, there are 4 obtuse marginal arteries (c). Distally the circumflex continues and gives rise to the PDA, (d) AV nodal artery and posterior LV branches
Ashley Davidoff MD
RCA in LAO
RCA Dominant 80-85%
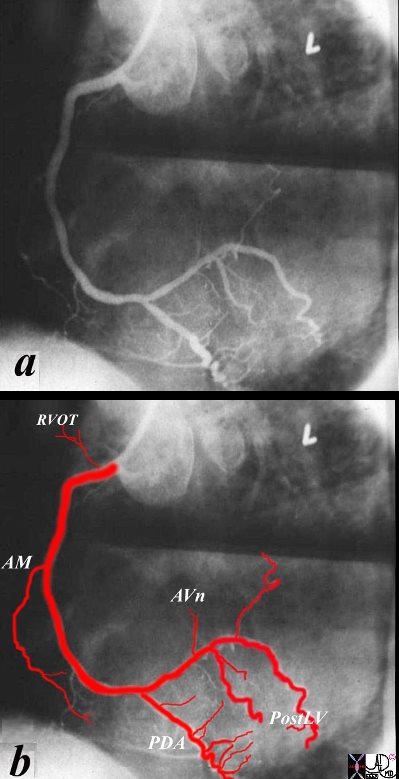
The angiogram of a dominant RCA shows the infundibular artery coursing to the RVOT, the acute marginal artery (AM), at the right margin of the heart, PDA and septal perforators,, A-V nodal (AVn) and posterior left ventricular branches (Post LV)
Ashley Davidoff MD
LCA Dominant in LAO
Dominant LCA 15-20% in LAO projection
AP Projection for Left Main

Ashley Davidoff MD
RAO projection
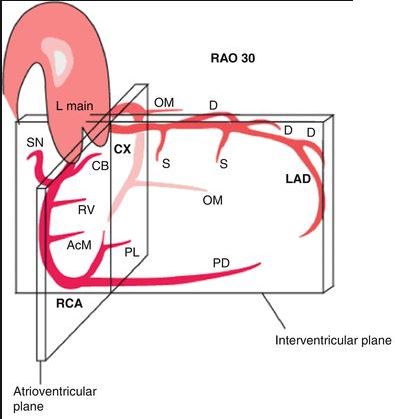
RAO projection of LCA
LAD thrown to the Horizon

TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
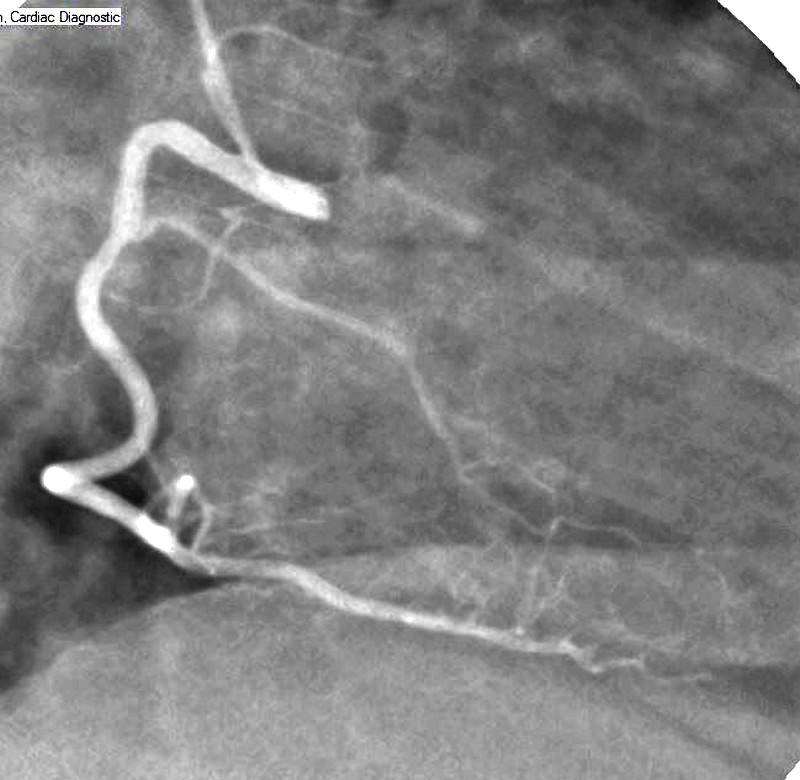
RAO projection of the RCA
RCA RAO PDA well Seen
TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD