
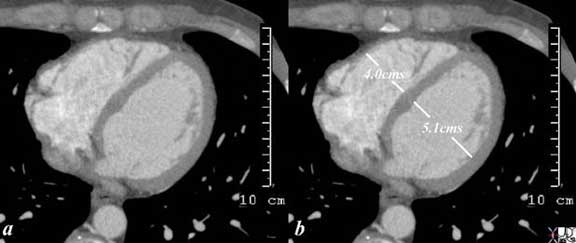
Description: This series of CT image shows a faint curvilinear lucency in the apical myocardium (a,b) as well as myocardial calcification. The lucency is thought to be a fatty deposition in infarcted myocardial tissue, and the calcification represents dystrophic calcification in the necrotic tissue. Included in the differential diagnosis is an apical aneurysm with calcification in clot. The calcification in the annulus is premature and unusual for this 56 year old male patient. Note the small bilateral pleural effusions. . 29601c code CVS cardiac heart MAC apical fat MI calcium myocardium apex cardiac imaging radiology CTscan
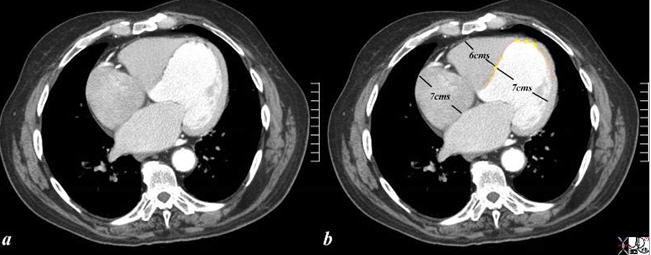
Description: This series of non contrast CT scans through the inferior aspect of the LV shows a thin lucency of fat density which is located on the endocardial side of the myocardium. This suggests that there is significant associated thinning of the myocardium. There are a few punctate dystrophic calcifications in the septal component of the lucency. (a,b) The lucent abnormality also extends to the apex and the free wall of the LV. In images c and d the apex bulges forming an apical aneurysm. The findings are consistent with previous infarction with fatty changes in the infarcted region. . 38325c code cardiac heart LV apex septum free wall lucent fat calcification MI aneurysm CAD IHD imaging radiology CTscan
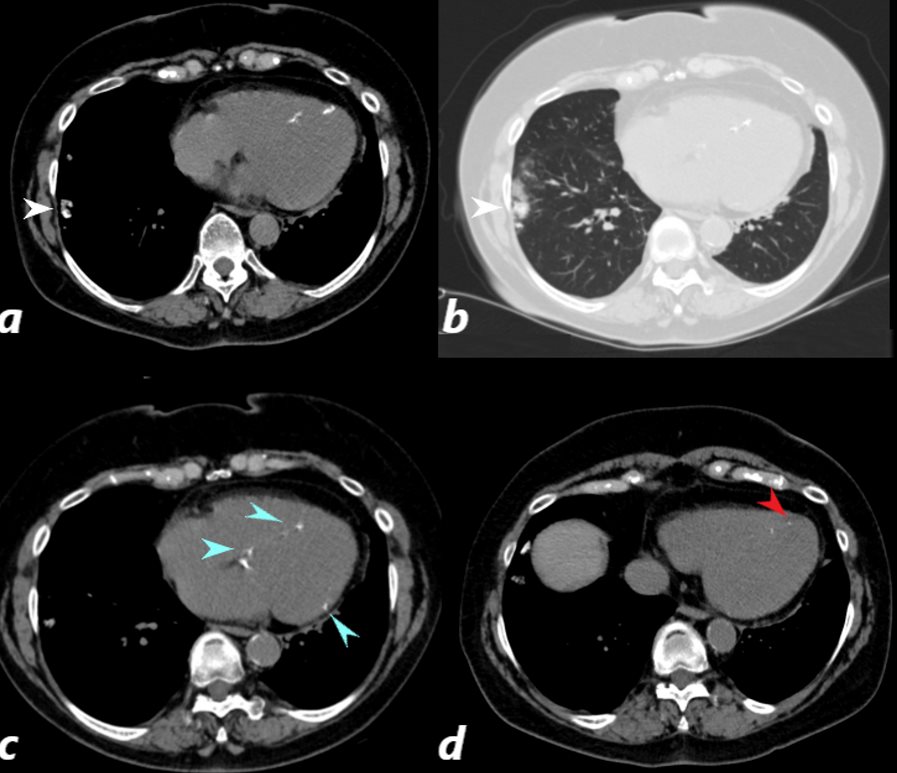
CT scan of a 67 year old female with anca positive vasculitis shows of dystrophic calcification in the lateral aspect of the right lower lobe (white arrow, a and b) )with focal nodular parenchymal consolidation, that likely reflects a site of prior small vessel infarct. Dystrophic calcification in the LV myocardium (blue arrows c) and a suggestion of fatty dysplasia in the left ventricular apex red arrow d) suggest changes from small vessel infarct.
Ashley Davidoff MD
Courtesy of: Ashley Davidoff, M.D heart-anatomy-P-047
Courtesy of: Ashley Davidoff, MD
aka 37758b01c01.8s
aka heart anatomy P 040