
Echo 2018
Normal sized left
ventricular cavity with mildly depressed left ventricular
systolic function, with an estimated LVEF 45-50%. Right
ventricle appears normal in size with mildly reduced systolic
function. The aortic valve is thickened, calcified and
trileaflet with mild restriction. The AVA by planimetry was 2.29
cm2 (would consider obtaining a TTE to assess AV more
completely). There is mild central AI. The mitral valve leaflets
are normal with mild MR. The tricuspid valve is structurally
normal with trace TR. Pulmonic valve was not assessed. Color flow
Doppler did not reveal evidence for intracardiac shunt. There
were no masses, thrombi or spontaneous echo contrast (“smoke”) in
the left or right atria or their appendages – normal left atrial
appendage emptying velocities (40-60 cm/s). .
CTA
History of Dyspnea
CORONARY ANATOMY: There is no evidence for anomalous coronary
arteries. There is codominant coronary artery dominance.
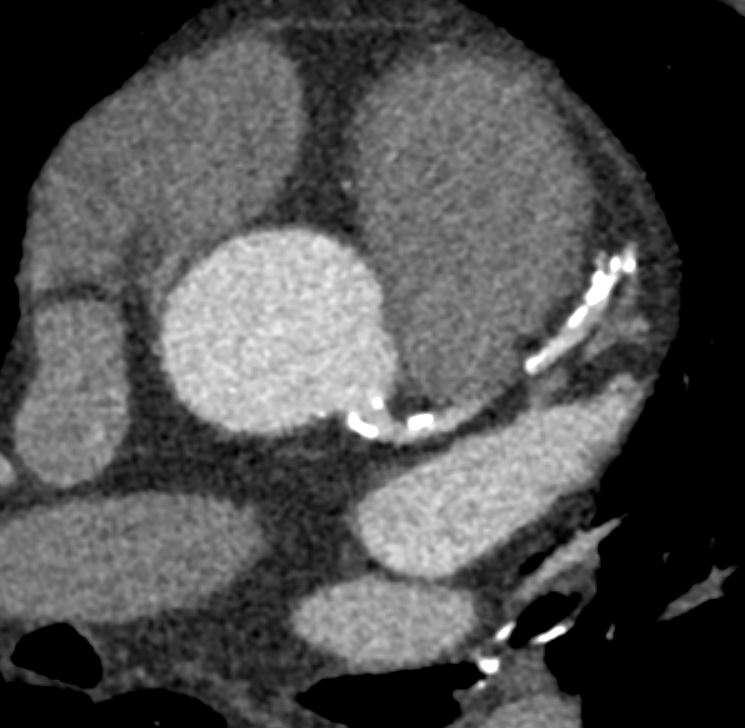
LM: The left main coronary artery is short, with the LAD and LCx
branching off rather proximally. There are coarse calcifications
within the LM and there is a suggestion of a hemodynamically
significant lesion at its origin.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
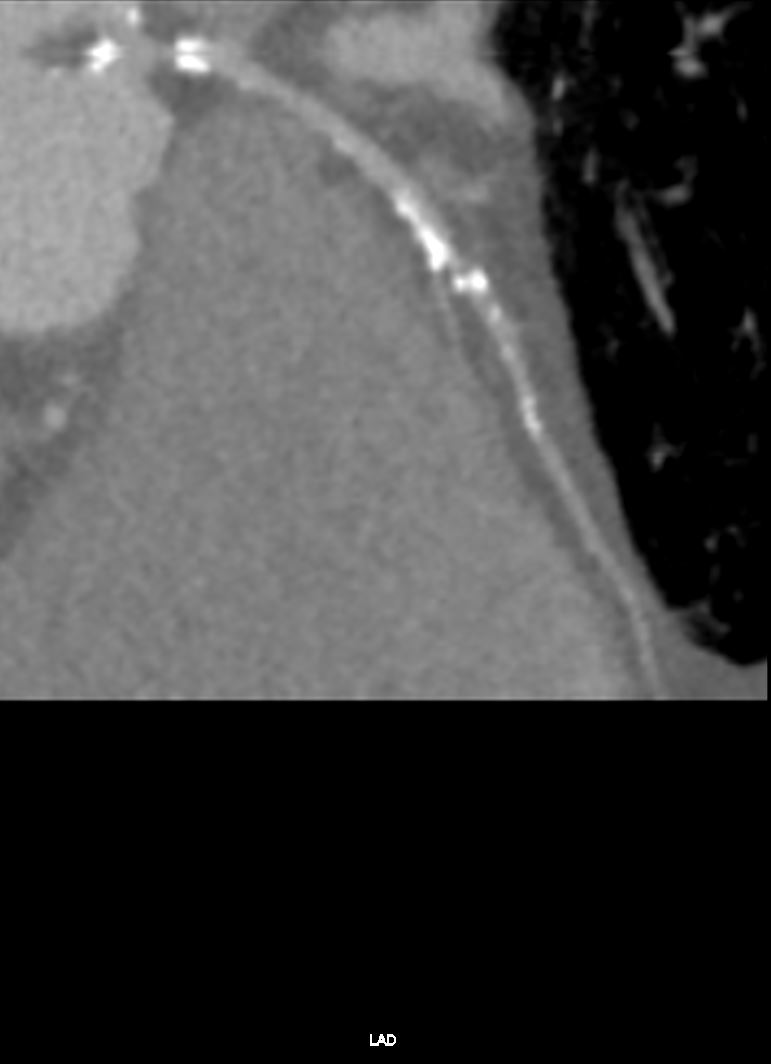
LAD: There are extensive coronary artery calcinations throughout theLAD, limiting evaluation.

LCx: Multiple within the left circumflex artery, with noted calcified
plaque but no occlusion identified. No significant proximal lesion
identified. Distally there is a prominent o’clock precluding optimal
visualization. 2 patent obtuse marginal (OM) branches are identified.
There is a branch that supplies the posterior left ventricle, which
is also supplied by the distal RCA.
RCA: The right coronary artery (RCA) has some calcified plaque with
no hemodynamically significant luminal narrowing, . The posterior
descending artery (PDA) originates from the right coronary artery.
The posterior left ventricular (PLV) branches originate from the RCA.
CALCIUM SCORE: The observed Agatston Calcium Score of 1112.62 is at percentile 84 % for subjects of the same age, gender, and race/ethnicity who are free of clinical cardiovascular disease and treated diabetes.

The Agatston score for each vessel is as follows:
LM:247.16; LAD: 596.24; LCx:184.18; RCA: 85.04;
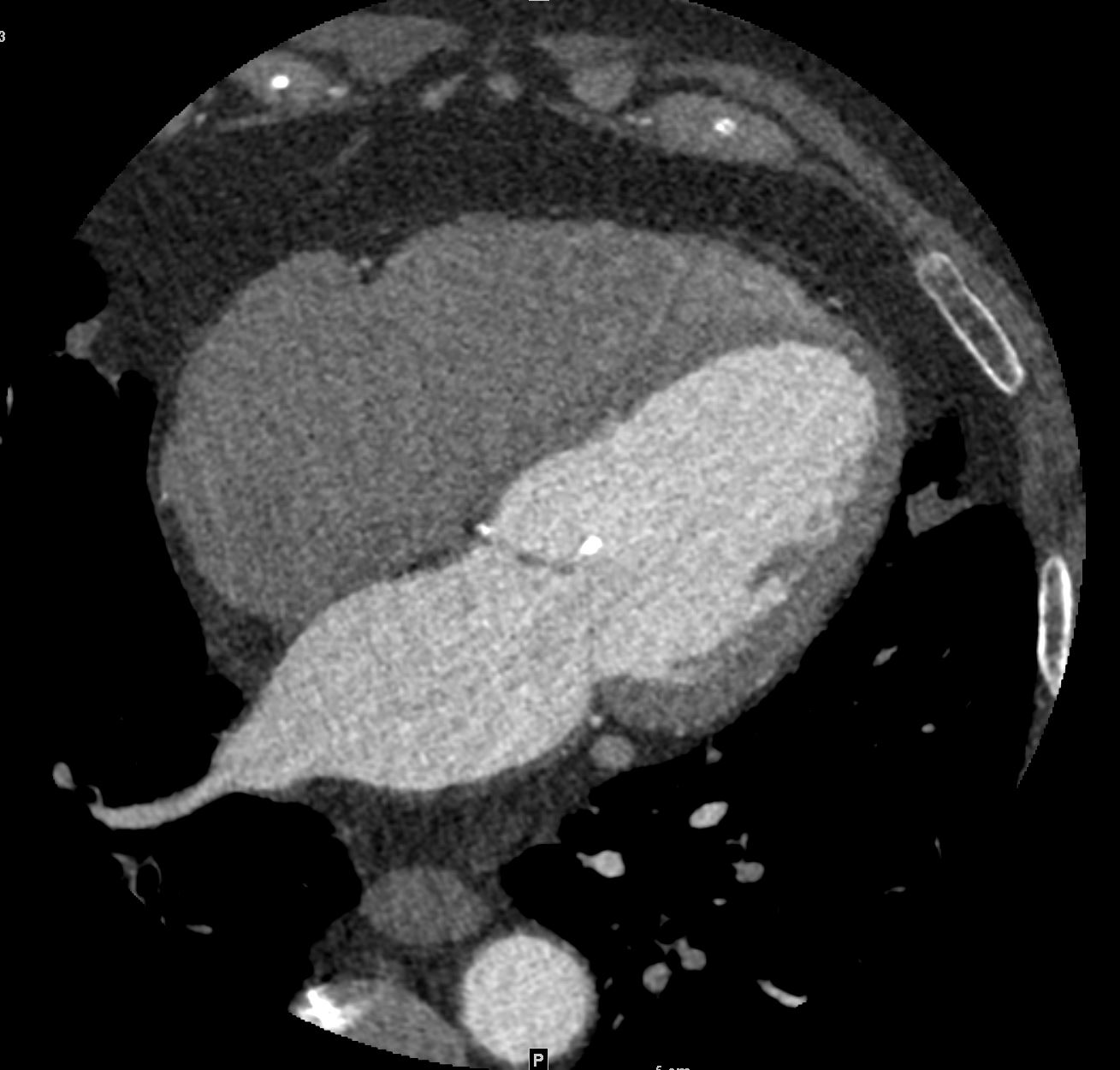
VALVES: Moderate to severe calcifications of the aortic valve and calcification of the anterior leaflet of the mitral valve



Cardiac Cath
Stable Angina
Aortic Valve Disease
CONCLUSIONS:
Mild nonobstructive coronary atherosclerosis
Right Dominant
Left Main: Normal
LAD:
Left Anterior Descending: Minimal luminal irregularities
LCX:
Left Circ: Normal
RCA:
RCA: Normal
INDICATIONS: