
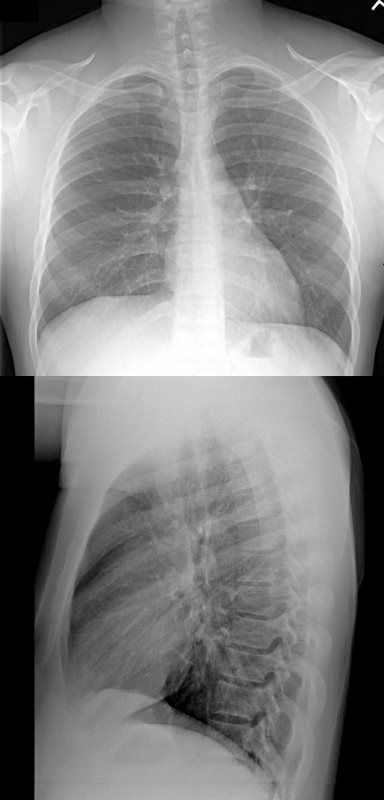
34-year-old male has a normal appearing CXR 1 year before presentation
Ashley Davidoff MD
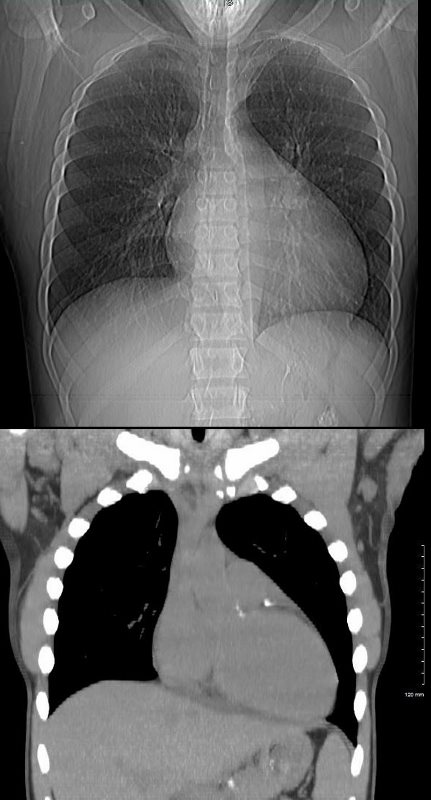
At the time of his first presentation with dyspnea his CXR showed perihilar infiltrates.

Ashley Davidoff MD
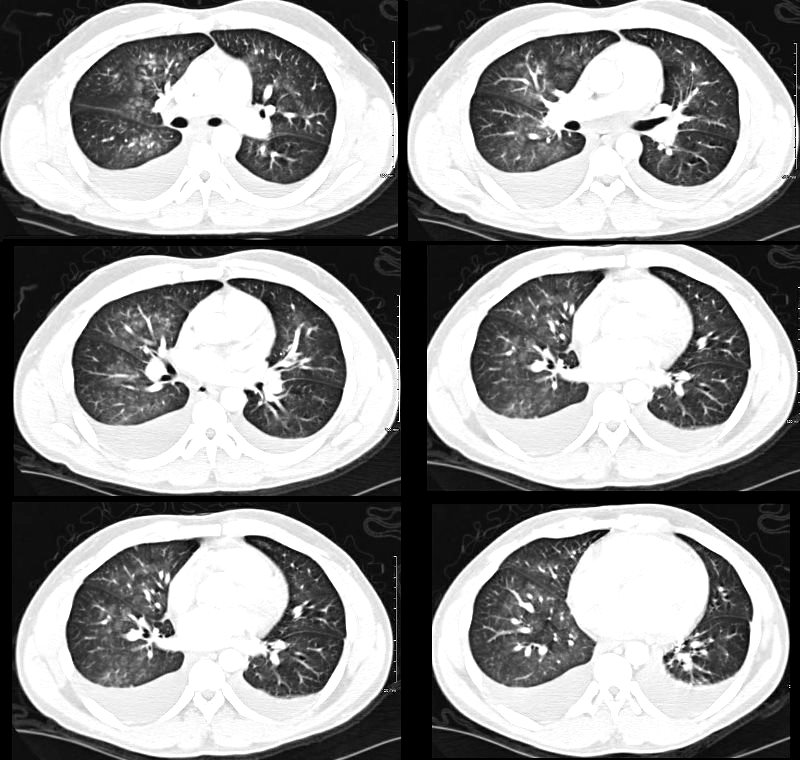
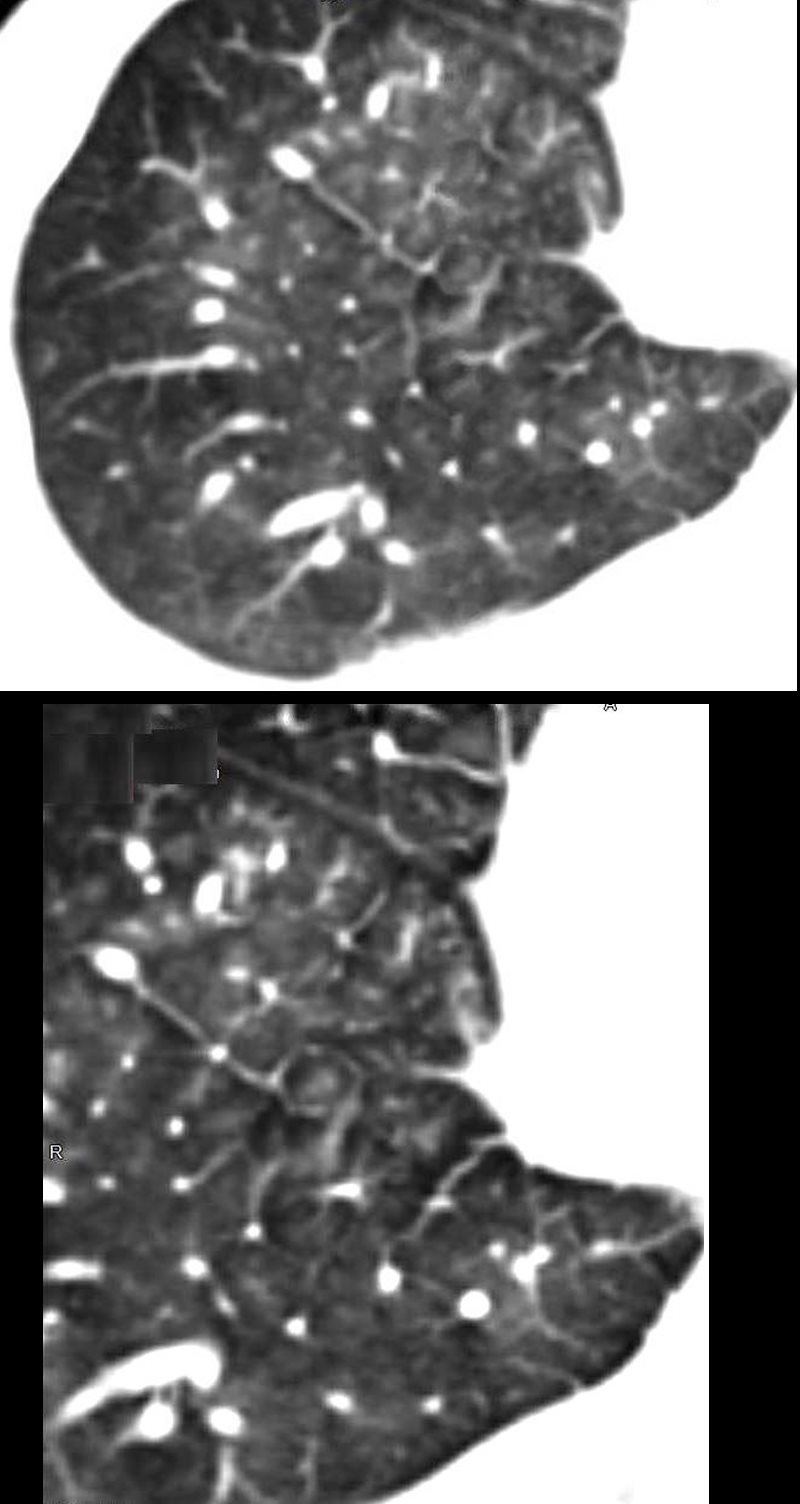
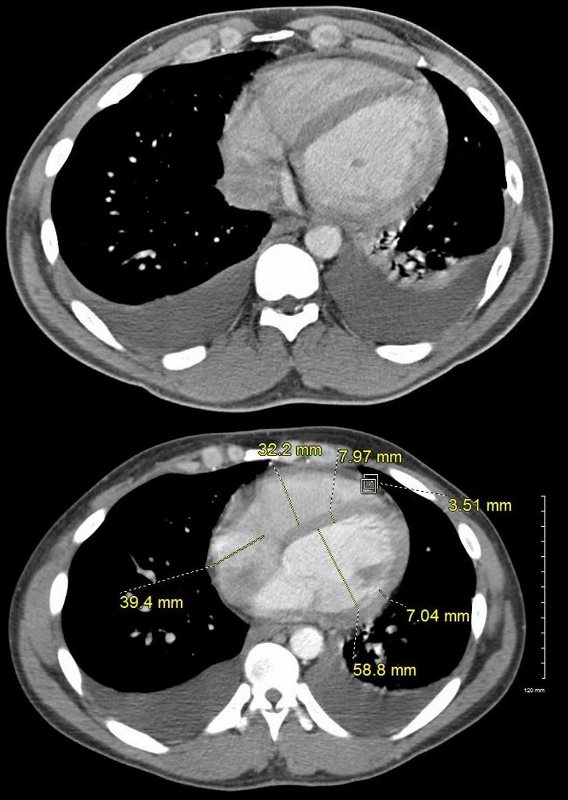
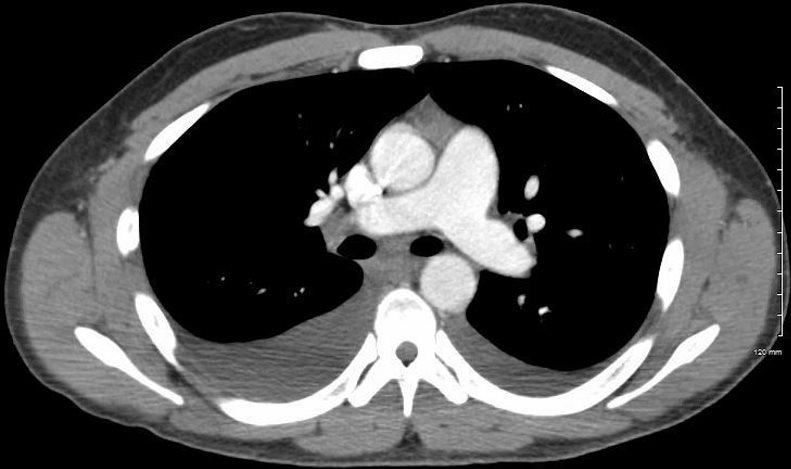
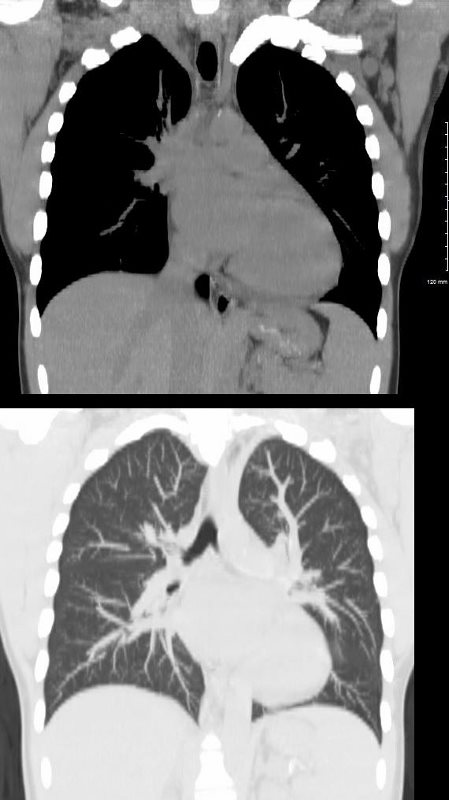
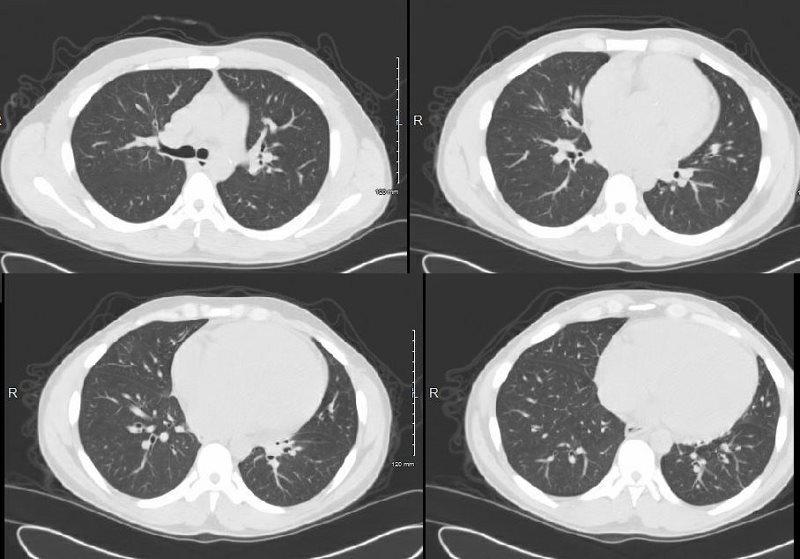
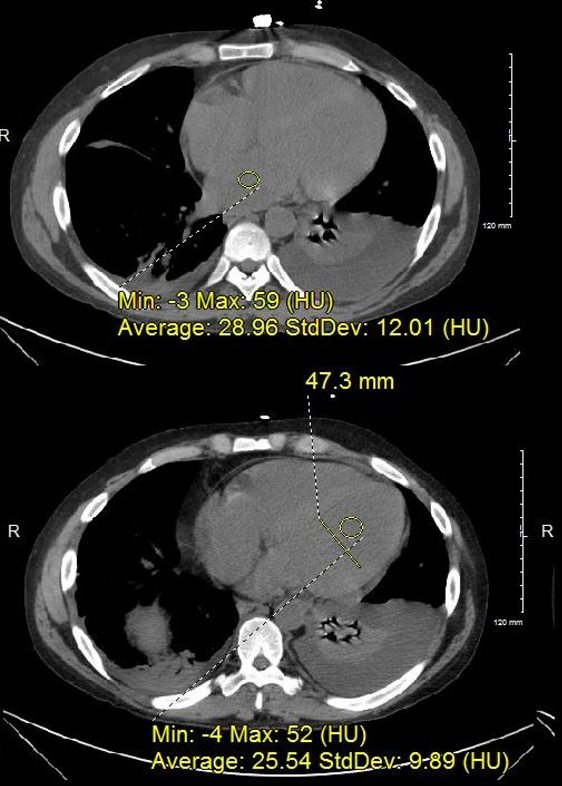
A CT confirmed progressive alveolar edema, with bilateral effusions (right greater than left), mild left ventricular dilatation, Kerley B lines and centrilobular densities and small pericardial effusion.

Ashley Davidoff MD
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD

DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
1 month after this admission a treadmill stress and rest gated SPECT study showed no evidence of ischemia with a calculated ejection fraction of 31%
A repeat CXR showed classical findings of left ventricular dilatation and left atrial enlargement but without CHF
CT showed early coronary calcification, LAE, LVE and resolution of the pericardial effusion with pulmonary hypertension. Lungs were clear.
{kind=link}
LVE- DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
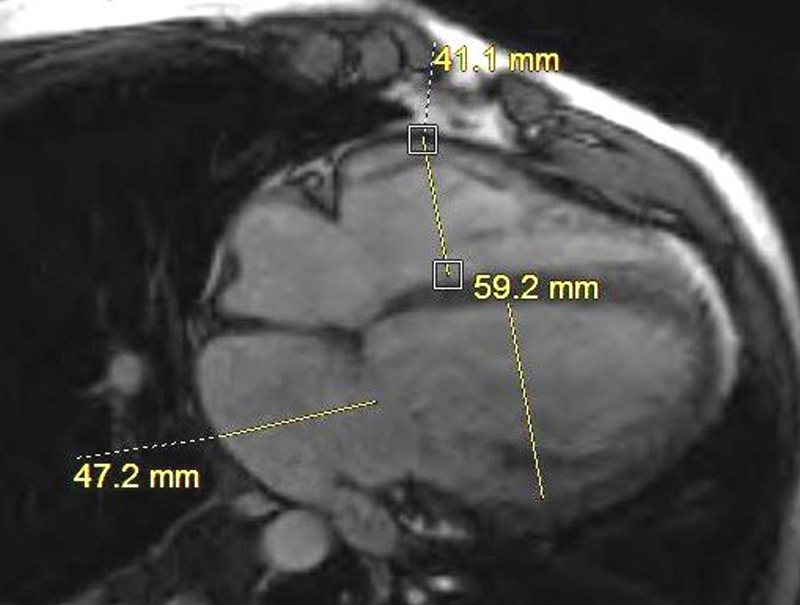
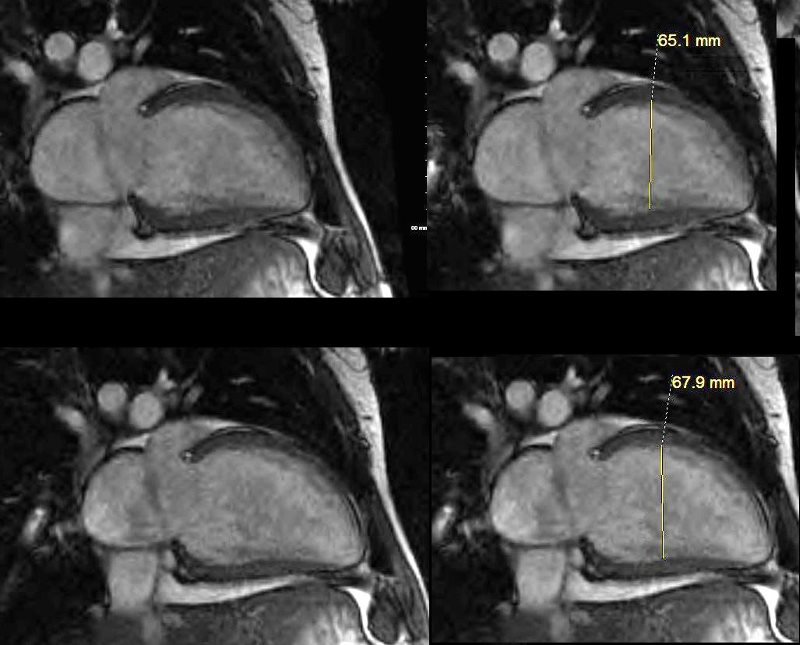
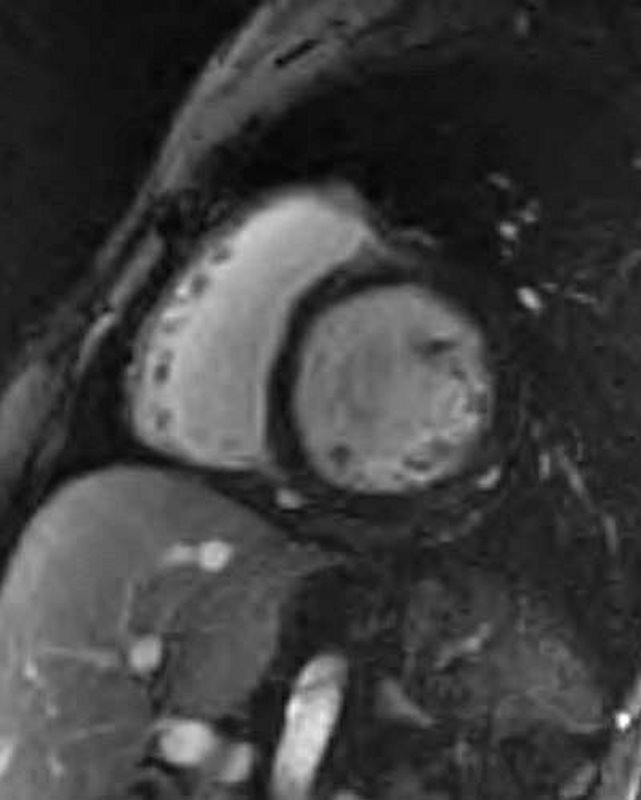
MRI confirmed the presence of a dilated cardiomyopathy, small pericardial effusion, without evidence of LGE, global hypokinesis and EF of about 20%
Ashley Davidoff MD
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
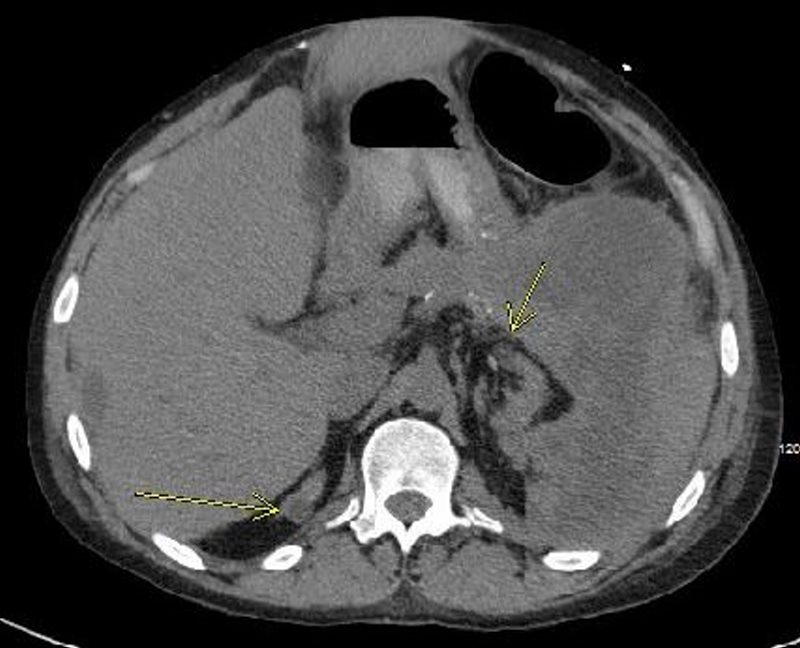
2 years later he presented with acute hemorrhagic pancreatitis that was felt to be related to his CRF
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
Serial CXRs over 3-4 days showed CHF with cephalization and early interstitial edema.

Ashley Davidoff MD
Echo showed improved LV function with EF of 50%, normal PAP, normal sized chambers, improved since the study performed 2 years earlier.
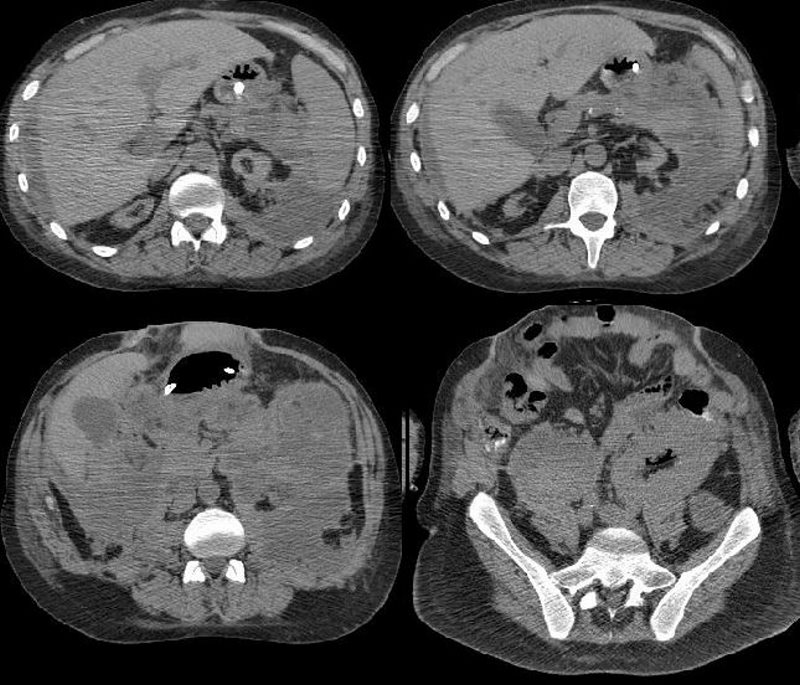
Repeat CT of the abdomen showed maturing pancreatic pseudocysts, mildly dilated LA, calcified medium sized vessels and calcification of the vasa deferentia
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD

DILATED CARDIOMYOPATHY, DIABETES, CRF, PANCREATITIS
Ashley Davidoff MD
-
Points of Interest
- Calcification of vasa deferentia
- Type of atherosclerotic calcification in diabetes
- Cardiogenic pulmonary edema and normal left atrial size
- Right sided effusion and CHF
- Acquired cystic disease of chronic renal failure
- CRF Diabetes and Cardiomyopathy
- Improvement in CM
- Frequency of no LGE in a dilated CM
- Etiology of pancreatitis in non alcoholic – ie CRF, Renal Tx and pancreatitis