
Patient is a 55 year old lady who presented with acute onset of chest pain, ruled out for an MI and a CTA of the chest revealed a localized dissection just above the sinotubular junction. Her blood pressure was very high and required Esmolol at 300 and nicardipine at 12.5 for control of her blood pressure and pain. Additional risk factors, hypertension, hyperlipidemia, diabetes x 7 years on orals, end-stage renal disease due to DM and HTN, on hemodialysis x 3 years, GERD, history of CVAx2 in the past and left facial nerve palsy, ischemic optic neuropathy, goiter, latent TB. She is a never smoker. Preoperative hematocrit 36.3%. Predicted Euroscore II: 9.01%. STS score: N/A.
Operative findings: Transesophageal echocardiography revealed normal ejection fraction, no wall motion abnormalities, severe LVH, trace aoritc and mitral regurgitation. The site of dissection was only faintly visible on TEE. Postoperatively, findings were similar.
The was a 2cm horizontal acute dissection extending from the LCC/RCC commissure towards the RCA and just at the level of the STJ. There was another flap just above the LCA and about 1 cm above the STJ, ca 2 cm in length. No proximal or distal propagation seen.
There was evidence of old healed dissection between these flaps.
Severe adhesions of the aorta to the MPA/RPA corresponding to the site of old dissection.
Multiple pericardial adhesions.
Aortic valve was trileaflet with thin leaflets and good coaptation.
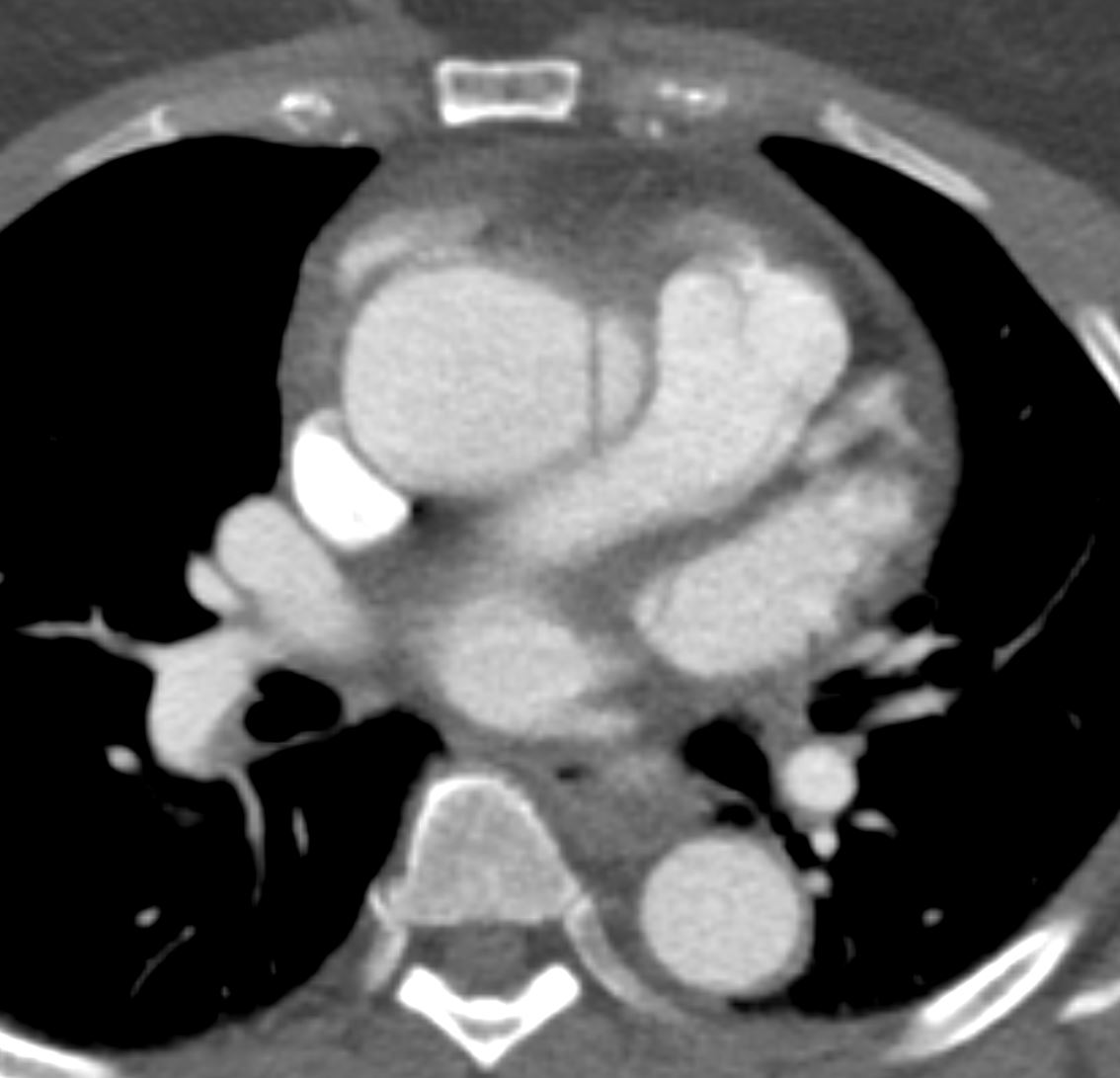
The axial images show an unusual medial tear of the aorta that almost appears to extend beyond the aorta and suggesting a motion artifact
Ashley Davidoff TheCommonVein.net dissection 001

The axial images show an unusual medial tear of the aorta that almost appears to extend beyond the aorta and suggesting a motion artifact. One image superior shows no dissection
Ashley Davidoff TheCommonVein.net dissection 002
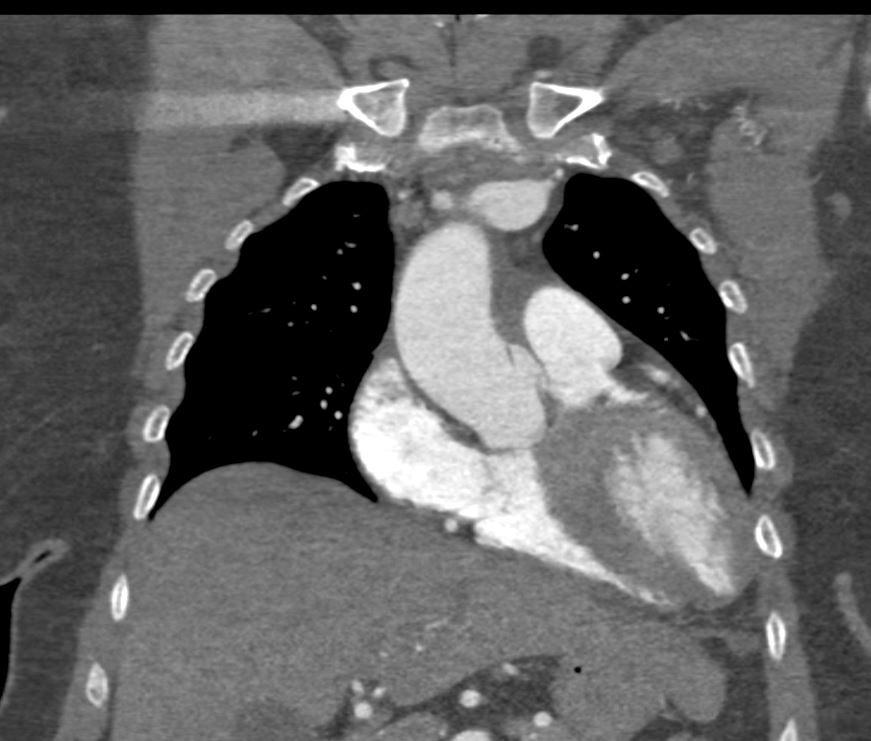
The coronal images are convincing for an aortic tear just above the left sinus of Valsalva
Ashley Davidoff TheCommonVein.net dissection 004