- 59 y.o. male.
- Hisotry of Paroxysmal atrial fibrillation of uncertain duration.
- walk several miles at slwo pace wihtout SOB or fatigue.
- No CP.
- No prioir presyncope or dizzines. RF: HTN/Obesity/OSA (using CPAP).
- ECG said to show AFibrillation
- VR 84.
- Cardioversion recommended.
- TTE said to show “dilated aorta”;
- 1 year ago
- asymptomatic episodes


- The basic rhythm was sinus with an average heart rate of 63 bpm and a range from 37 bpm – 128 bpm. Atrial fibrillation burden was 0%. There were 0 pauses of 3 seconds or longer. Supraventricular premature complexes were rare with rare couplets and rare triplets. There were 5 runs of supraventricular complexes up to 6 beats long. Premature ventricular complexes were rare with rare couplets and no triplets. There was 1, 4 beat run of ventricular tachycardia. No seconds or third degree heart block was detected. Patient trigger was activated during sinus rhythm.
- 2 years ago Stress Test
- negative for ischemia
- 1 year ago
- Hisotry of Paroxysmal atrial fibrillation of uncertain duration.
- CTA
-
- Severe atherosclerotic calcifications throughout all 3 coronary artery territories which limits evaluation of severity of luminal narrowing.
There is likely multifocal luminal narrowing, most severe in the LAD distribution, mild in the left circumflex, and moderate in the right coronary artery. 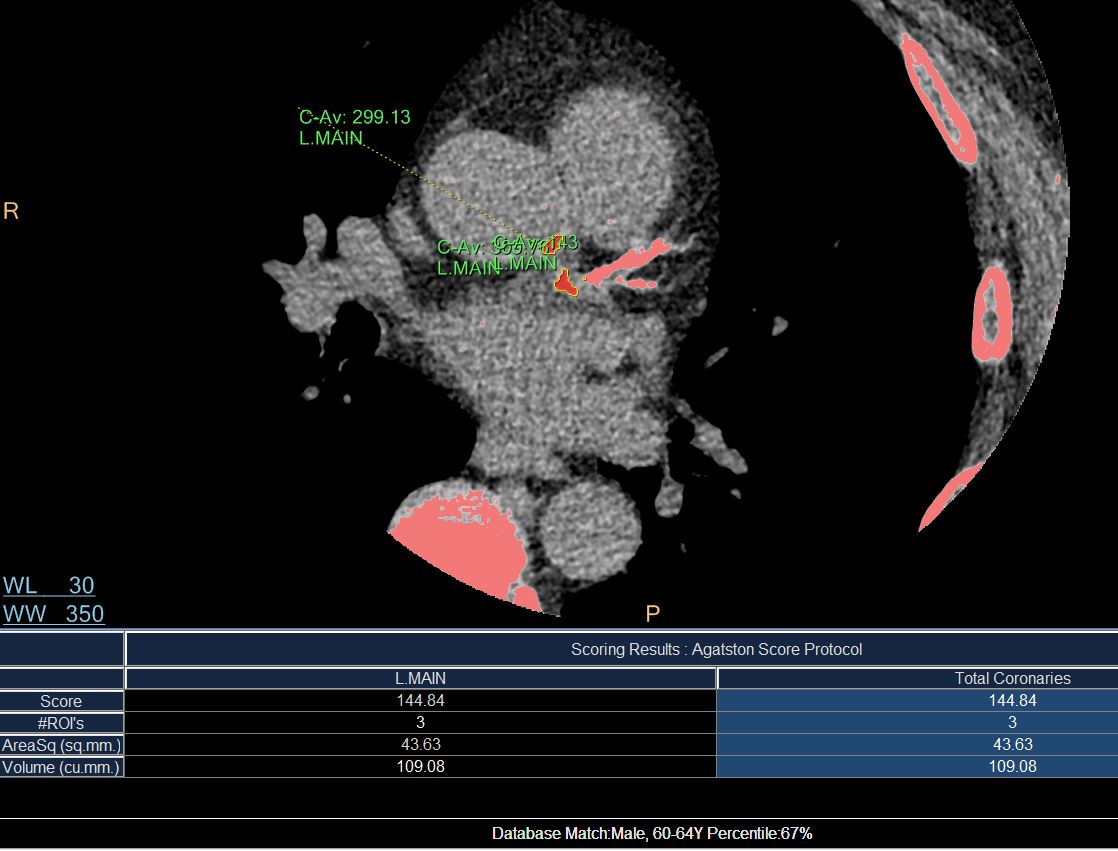
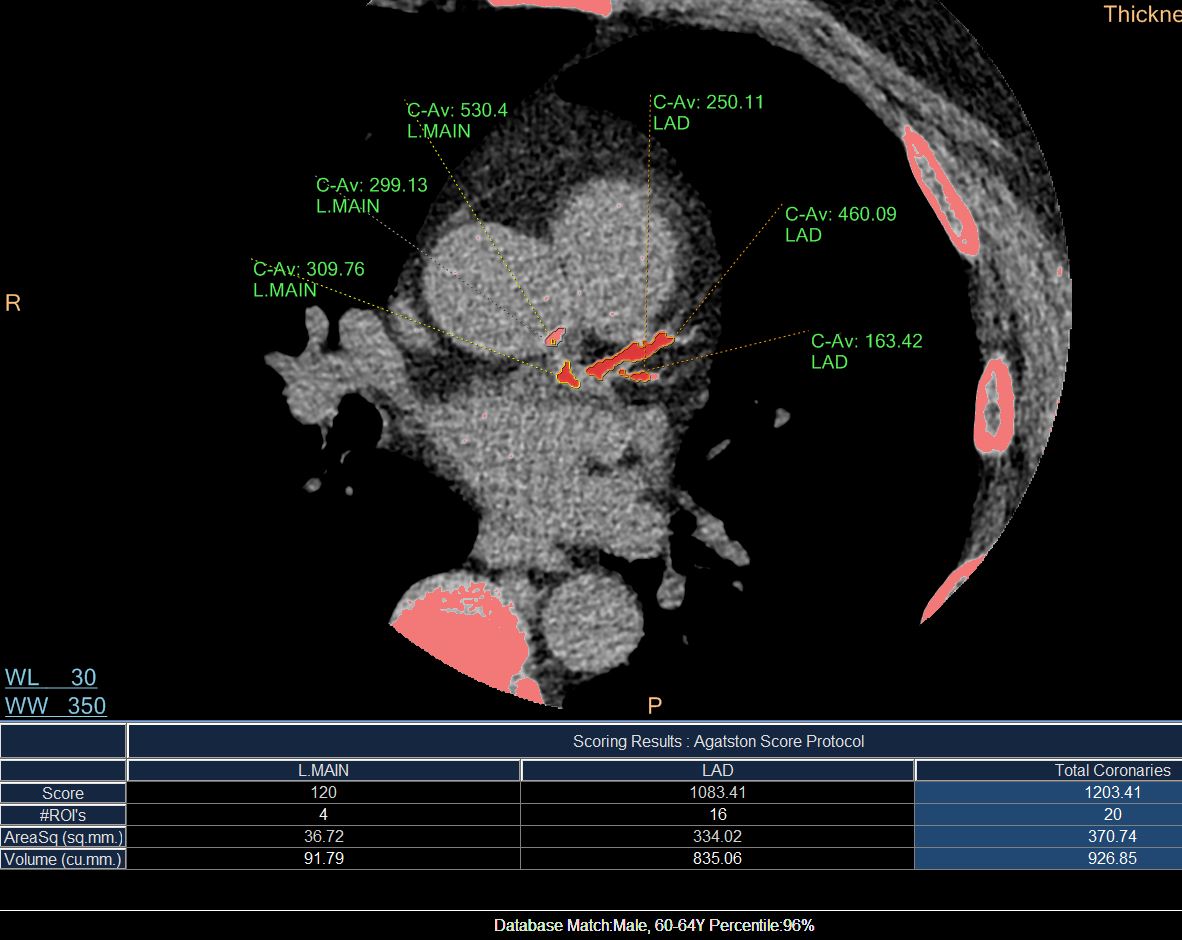
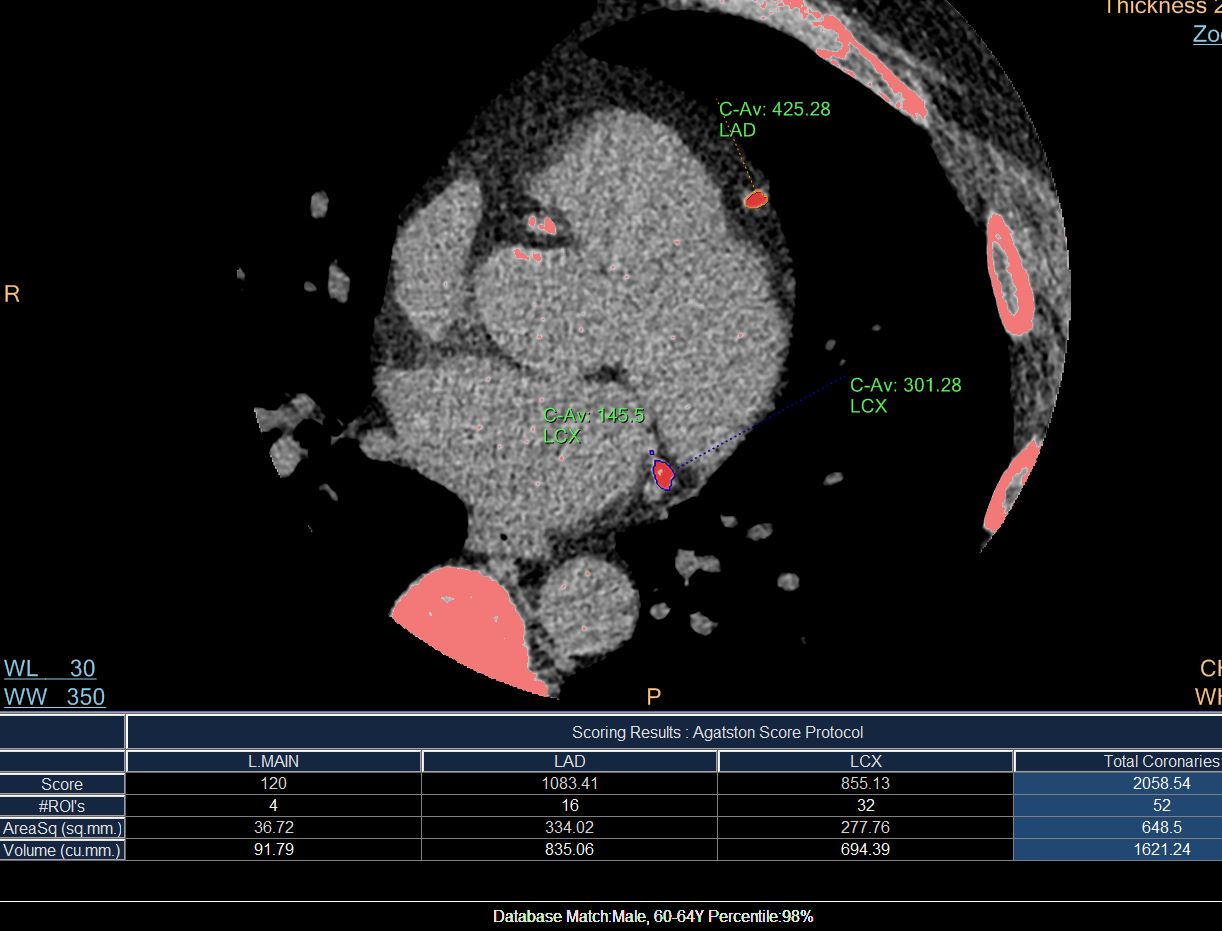

- Agatston Calcium Score = 2996.
- Severe atherosclerotic calcifications throughout all 3 coronary artery territories which limits evaluation of severity of luminal narrowing.
- LCX and RCA (Bone Window)
-
- Cardiac Cath
- cardiac risk factors of
- Fam Hx, htn, chol.
- Paroxysmal afib and is s/p DCCV 2 years ago. He then completed one month of Xarelto.
- recent ECG
- no atrial fibrillation,
- 5 runs of supraventricular complexes up to 6 beats long.
- rare premature ventricular complexes
- rare couplets and no triplets.
- cardiac risk factors of
- INDICATIONS:
Unstable Angina - Coronary angiography showed two vessel disease with a
- 60% mid-LAD lesion (flow limiting, FFR .76 after adenosine) and
- 70% mid-RCA lesion.
- Successful PCI of the mid-LAD and mid-RCA with DES stents.
- maintain on aspirin and plavix for a minimum of 3 months. If
anticoagulation needed, would then treat with plavix and
anticoagulant.CORONARY CIRCULATION:
Co-dominant
Left Main: Normal
LAD:
Mid LAD: Lesion 60 %
LCX:
Left Circ: Mild disease
RCA:
RCA: Lesion 70 %PROCEDURAL COMMENTS:
Engaged left coronary with an XB 3.5 guide. Crossed LAD with a flow wire. Resting FFR was 0.90 and was .76 after IV adenosine.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}