
Symptoms
- complaining of dyspnea on exertion, fatigue,
- decreased exercise tolerance.
- 7 years ago.
- s/p DES x 2 to LCX
- echocardiographic evidence of HCM associated with
- chordal SAM and significant
- LVOT gradient. 137 mmHg;
- peak velocity of his MR is 8.4 m/s,
- corresponding to at least a LV systolic pressure of 283 mmHg.
- MRI 4 years ago
- 1.The LV is normal in size.
- symmetrical LV hypertrophy with
- slightly more prominent thickening at the base antero-septal wall.
-
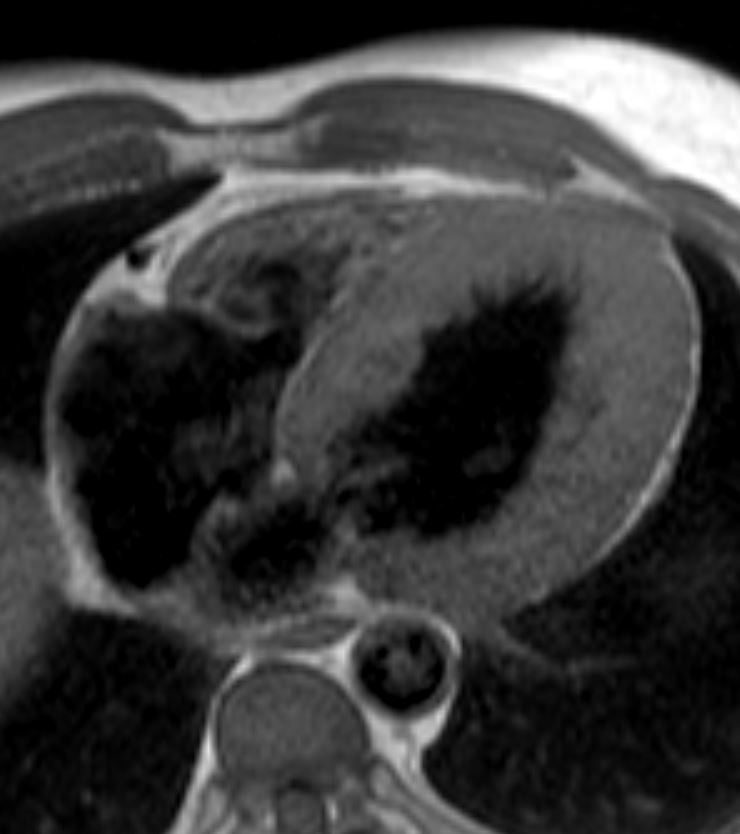
60M HOCM
Concentric Hypertrophy
Anomalous RCA from LCA
Ashley Davidoff
thecommonvein.net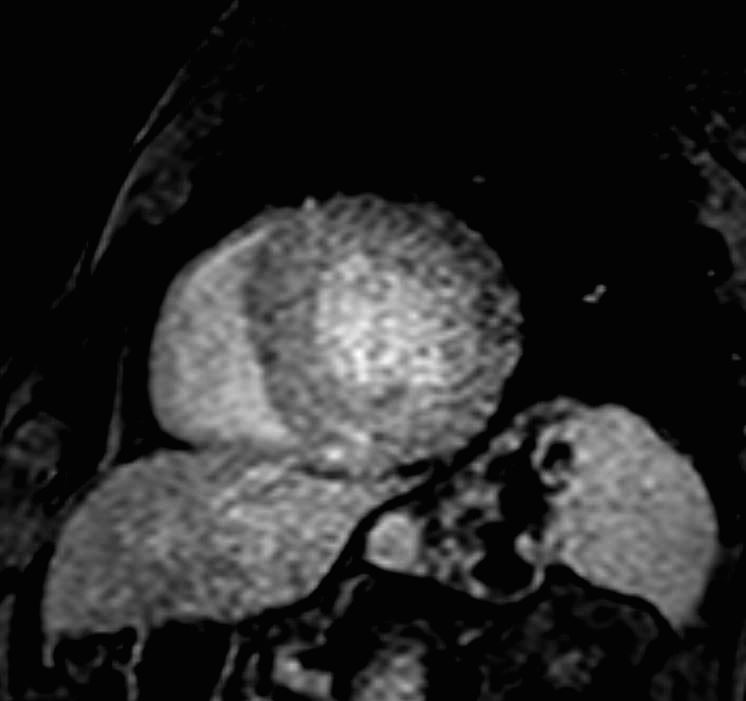
60M HOCM
Concentric Hypertrophy
Anomalous RCA from LCA
Ashley Davidoff
thecommonvein.net- maximal wall thickness is 16 mm
- normal left ventricle
- LVEF: 67 %.
- SAM
-
-
- flow acceleration through LVOT in systole with
- systolic anterior motion of the anterior mitral valve leaflet
- mild to moderate MR.
-
-
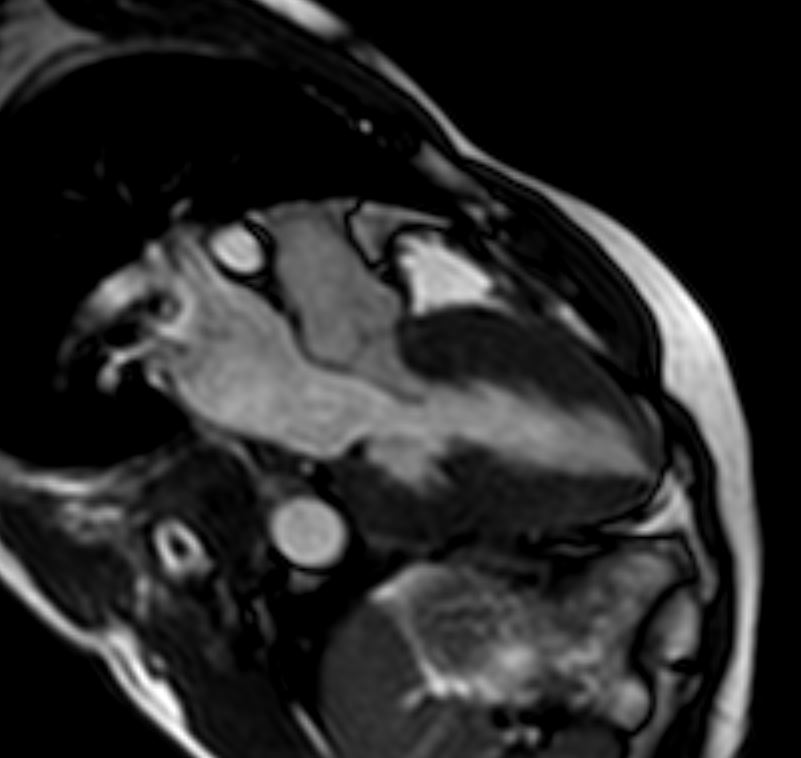
60M HOCM
Diastole – Mitral valve wide open Concentric Hypertrophy
Anomalous RCA from LCA
Ashley Davidoff
thecommonvein.net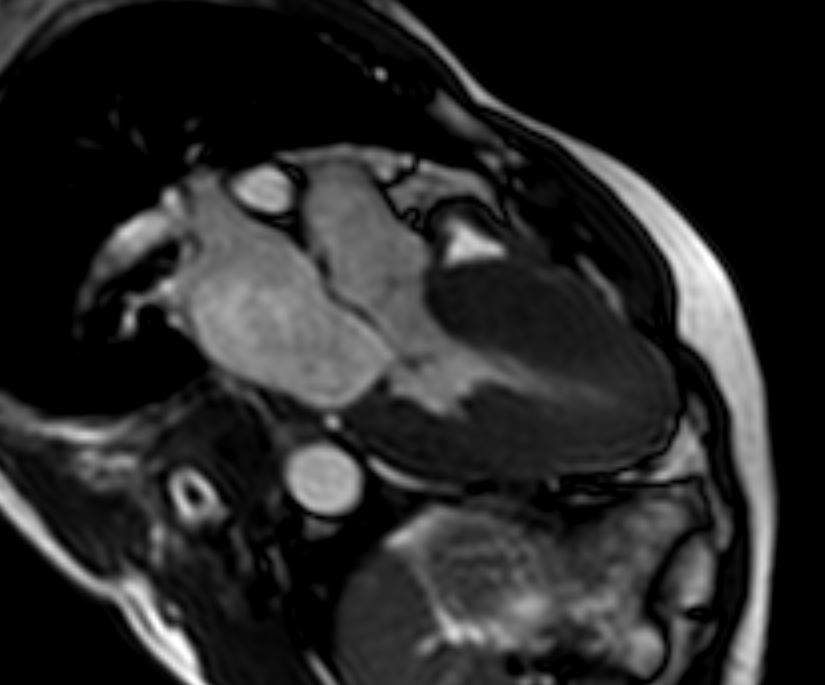
60M HOCM
Early Systole , LVOT open, Concentric Hypertrophy
Anomalous RCA from LCA
Ashley Davidoff thecommonvein.net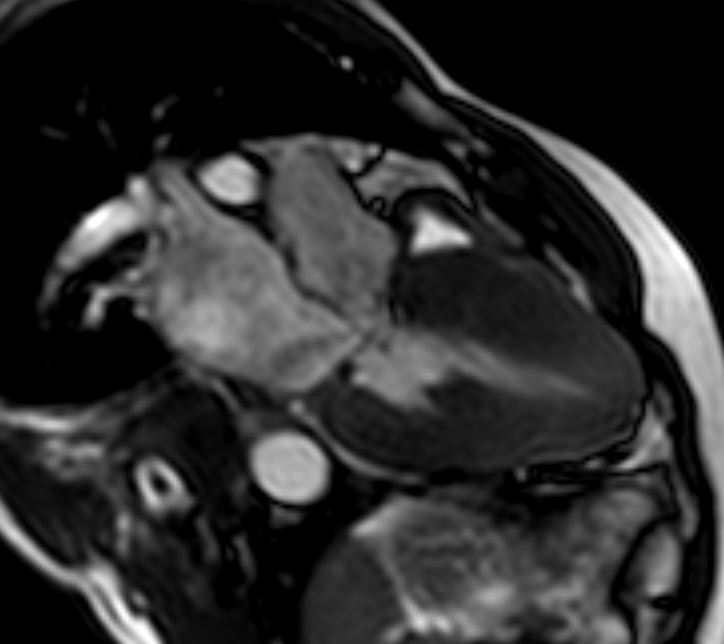
60M HOCM
Peak Systole, LVOT narrowed by systolic anterior motion of the mitral valve with associated mitral regurgitation – Concentric Hypertrophy
Anomalous RCA from LCA
Ashley Davidoff thecommonvein.net - LGE diffuse intermediate intensity signal of late gadolinium
enhancement- sub-endocardium and mid-endocardium layer
- basal anterior wall,
- basal lateral wall and
- basal inferior wall with
- scattered high intensity foci in the base anterior wall
- suggestive of fibrosis
- consistent with hypertrophic cardiomyopathy.
-
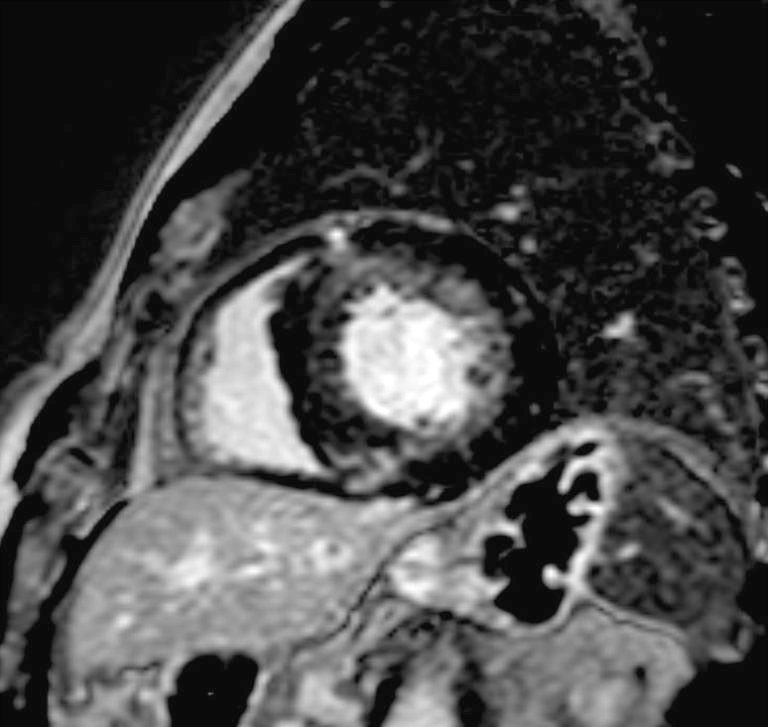
60M HOCM
LGE – sub-endocardium and mid-endocardium layer , basal anterior wall,
Ashley Davidoff thecommonvein.net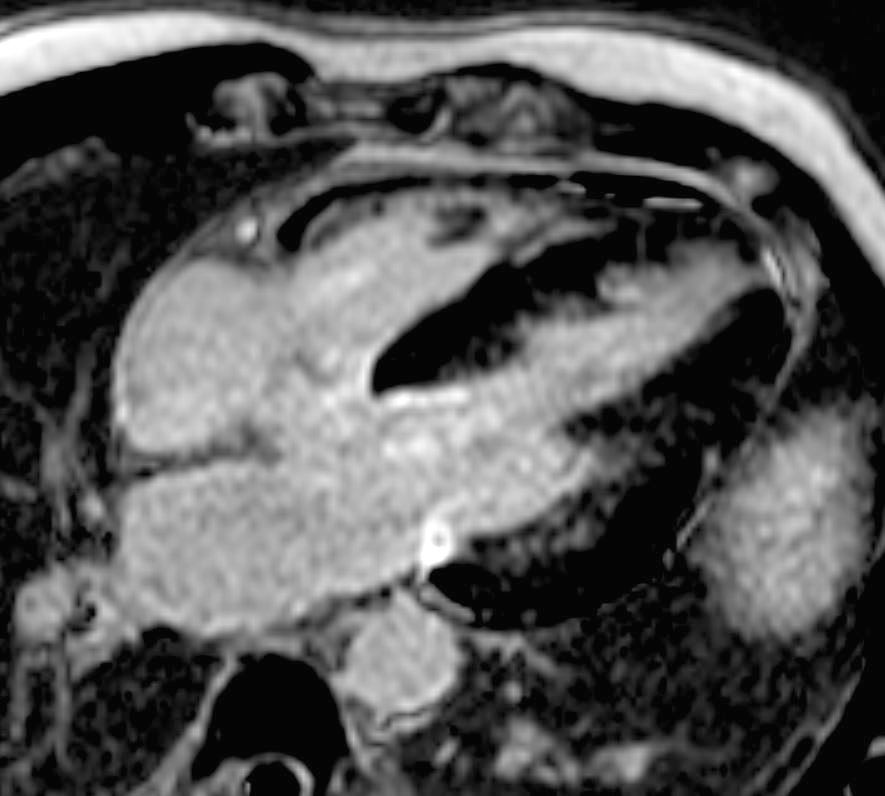
60M HOCM
LGE – sub-endocardium and mid-endocardium layer , basal anterior wall,
Ashley Davidoff thecommonvein.net
60M HOCM
LGE – sub-endocardium and mid-endocardium layer , basal anterior wall,
Ashley Davidoff
thecommonvein.net
- sub-endocardium and mid-endocardium layer
-
- s/p recent coronary angiography in 3years ago
- clean coronaries with
- patent stent as well as
- anomalous RCA arising from his LMCA.
- s/p CTA 3 years ago
- non-obstructive CAD and
- anomalous origin of RCA with acute angle at takeoff
- interarterial course.
- preserved global systolic LV function.
-
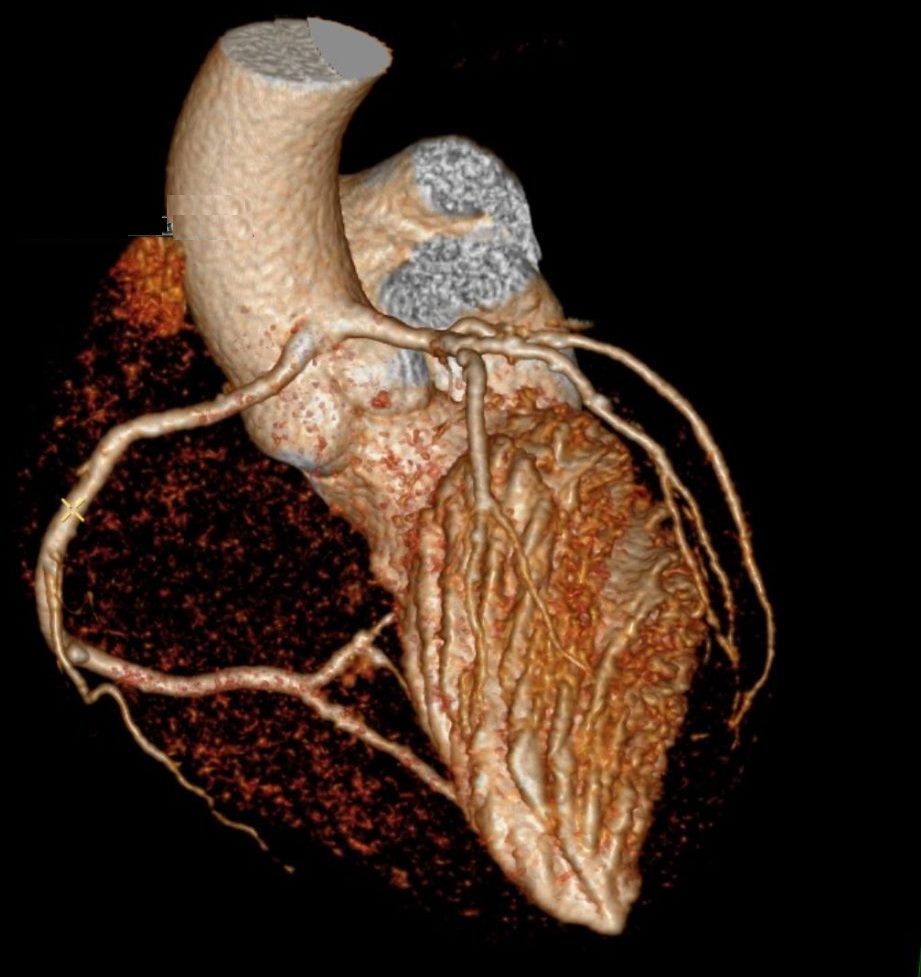
60M HOCM Anomalous Origin of the Right Coronary Artery From the Left Coronary Artery Sinus
Ashley Davidoff
thecommonvein.net