
023H Takotsubo and a Police Visit
TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
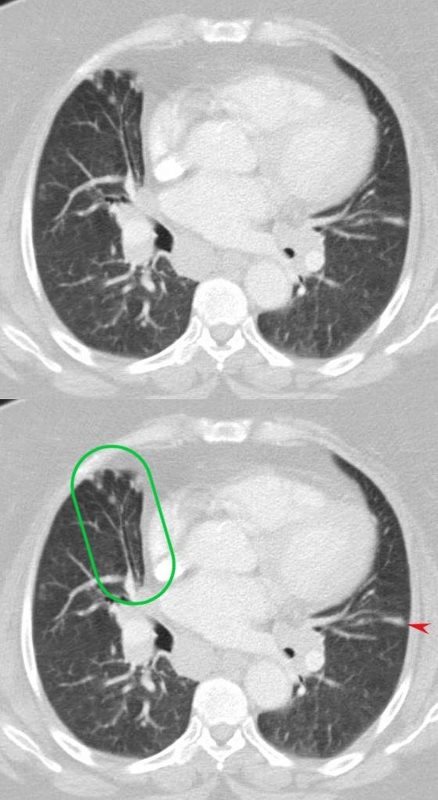
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
DAY 1
On admission
EKG showed ST elevation in V4 and V5.
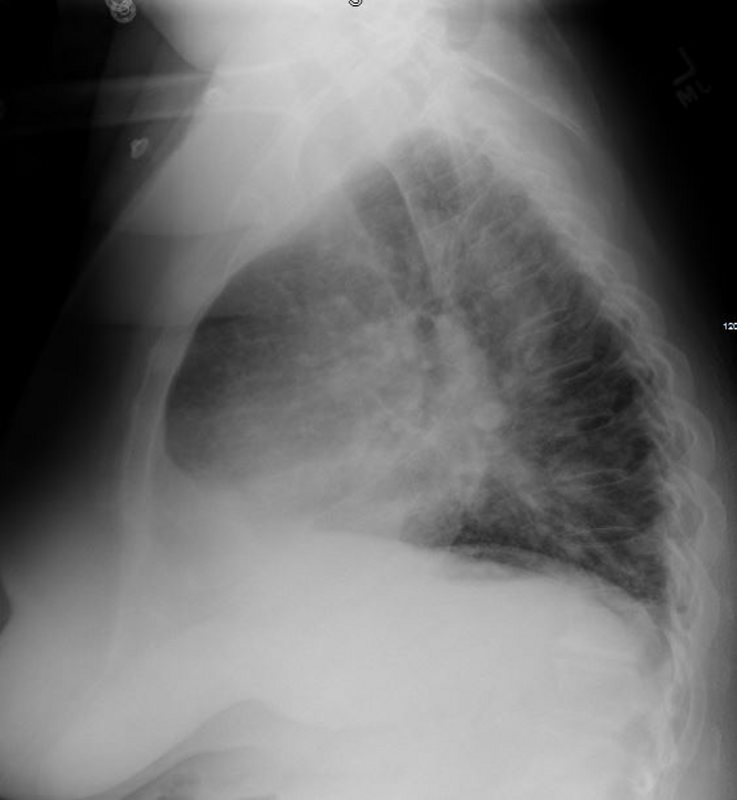
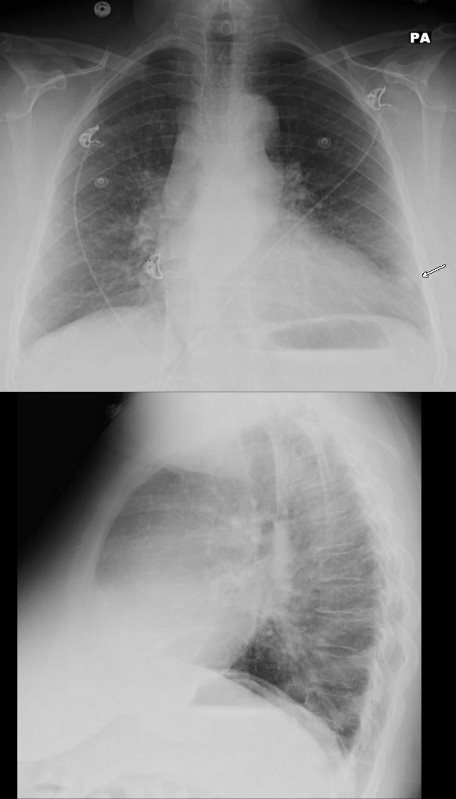
CXR showed LAE and LVE mild congestion, and left lower lung nodule.


Ashley Davidoff MD
Ashley Davidoff MD
Echo showed EF of 50% and apical hypokinesis.
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
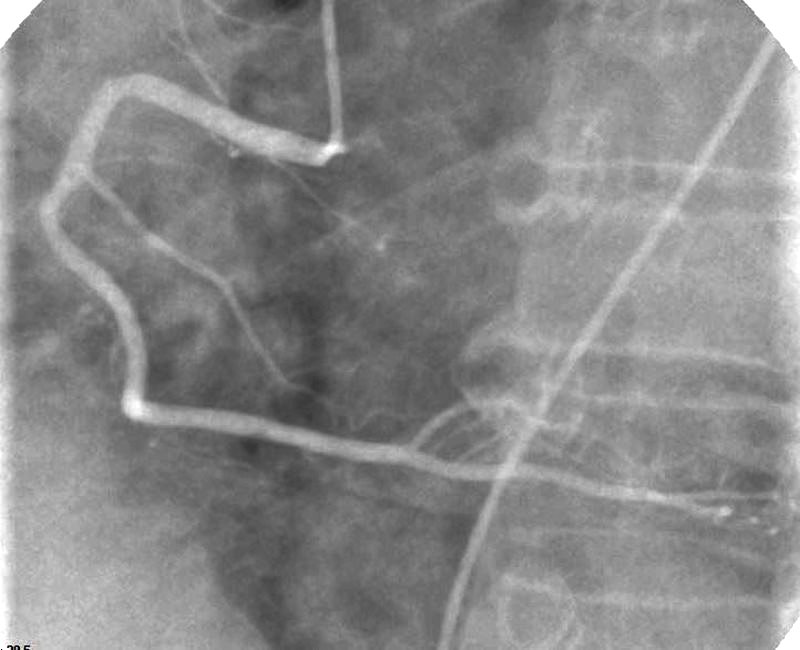
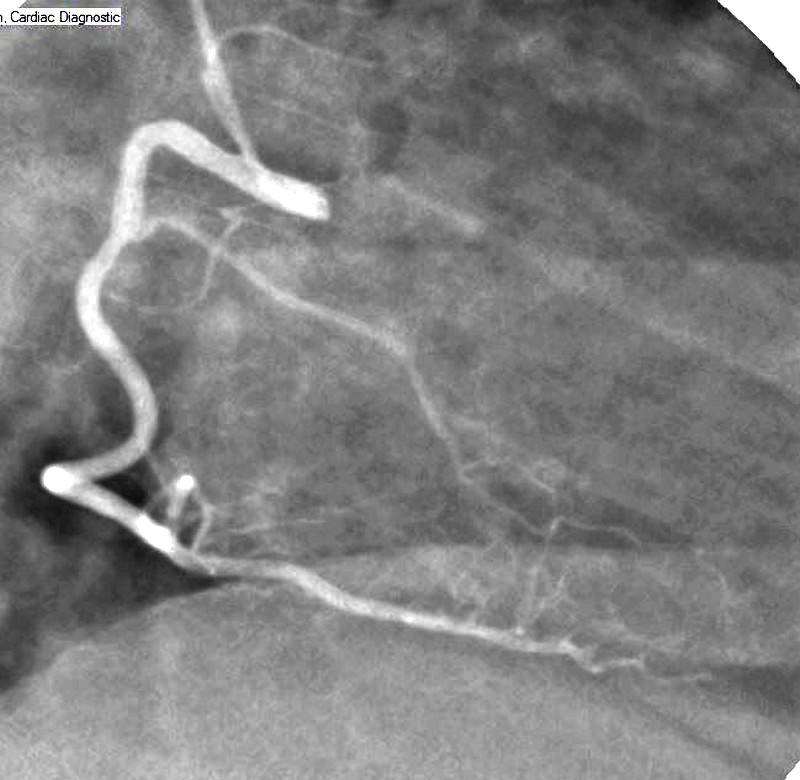
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
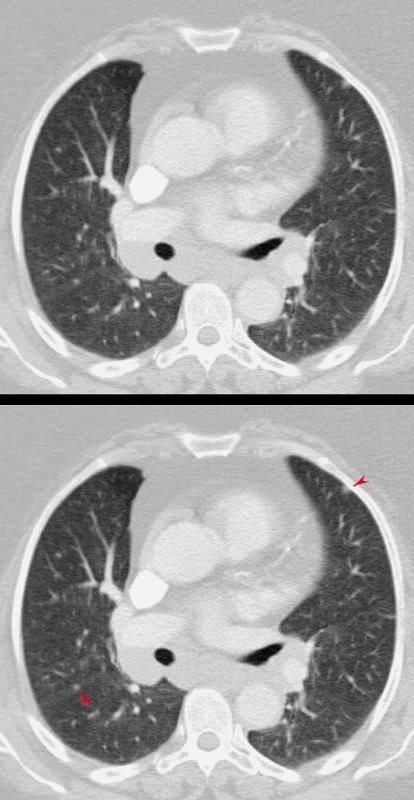
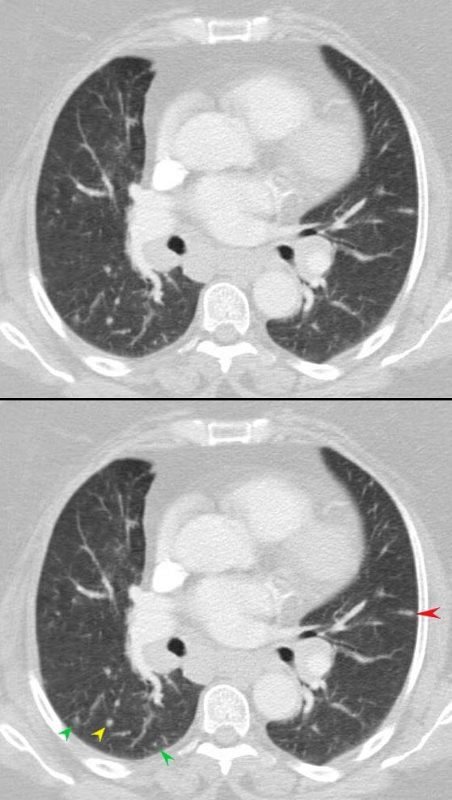
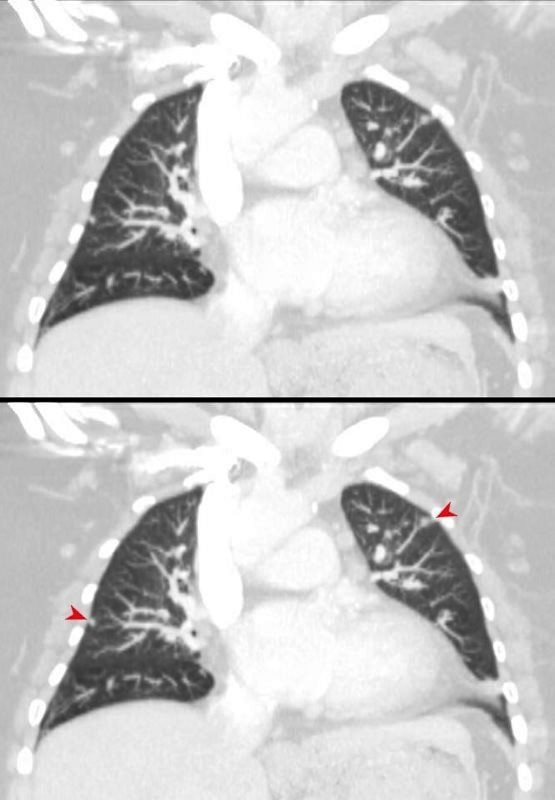
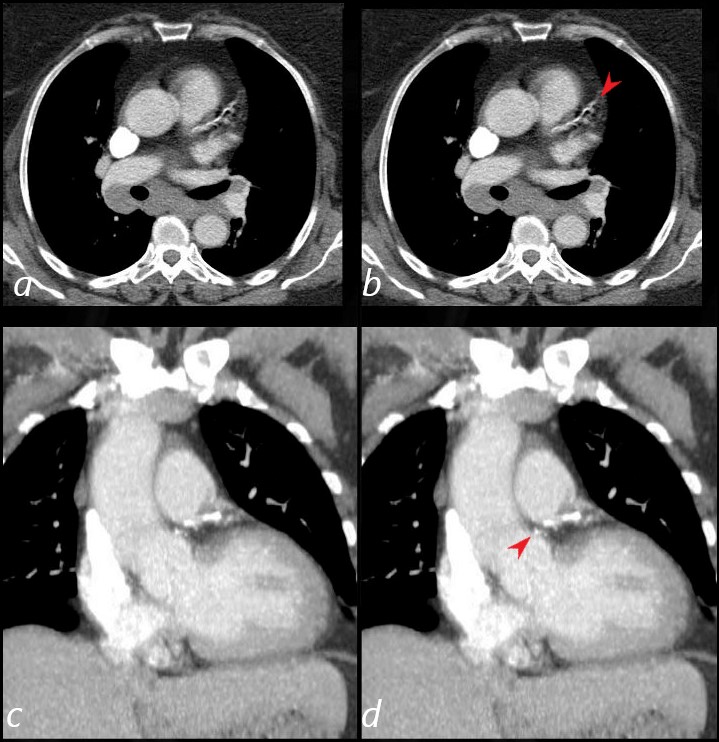
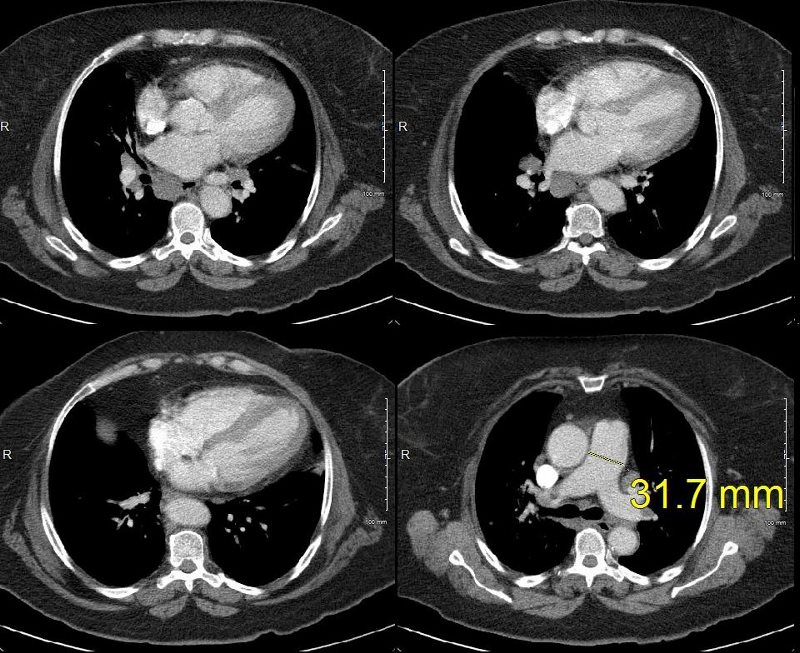
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
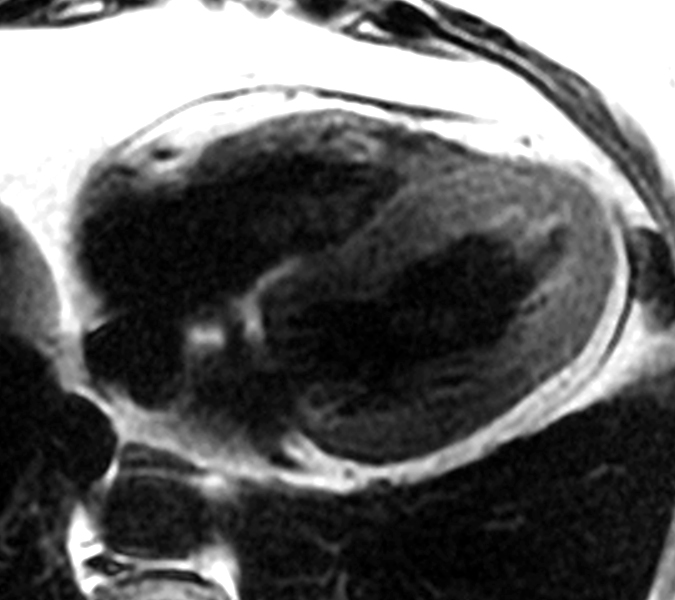
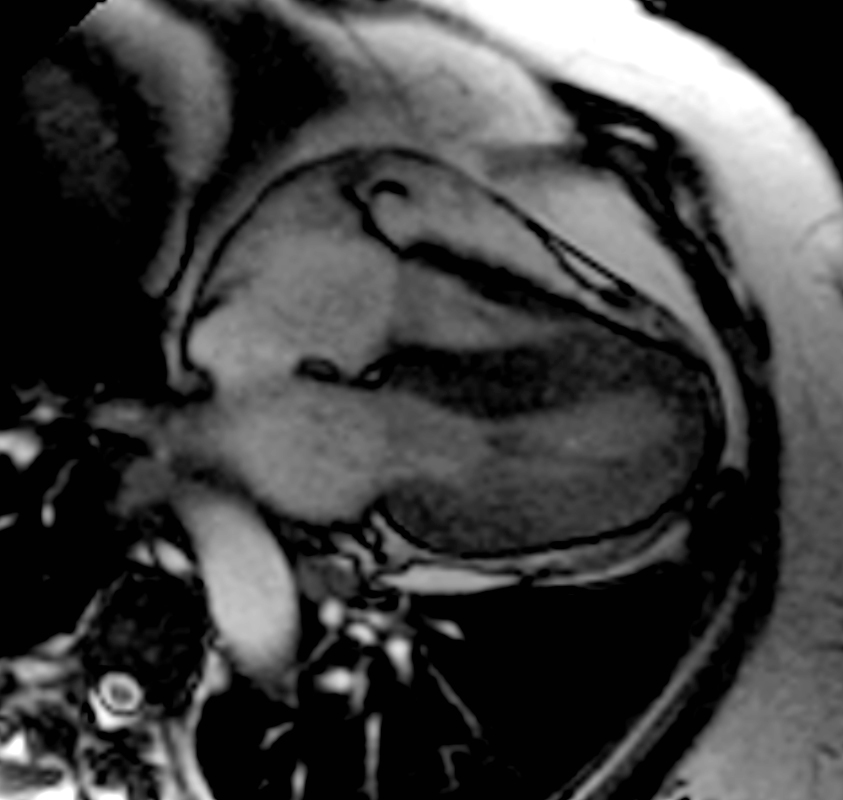
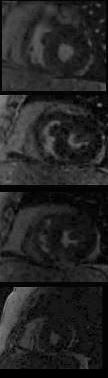
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
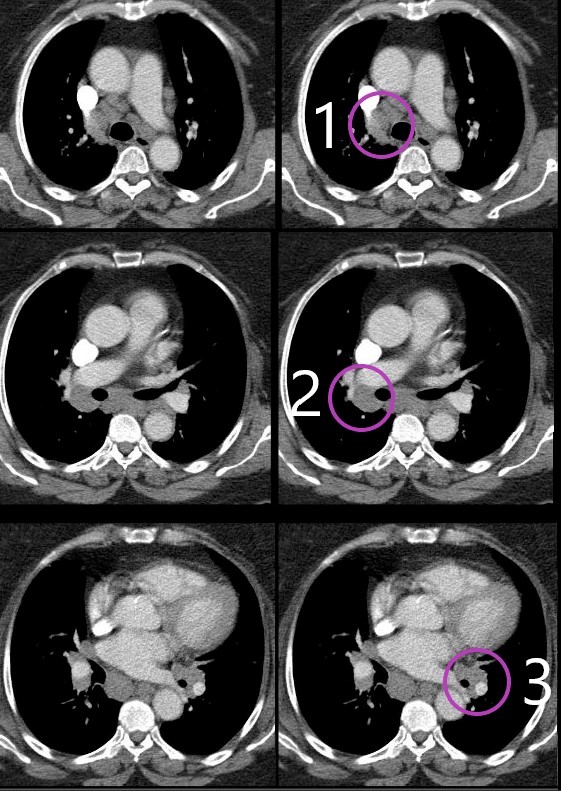
MEDIASTINAL AND HILAR ADENOPATHY
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
SARCOIDOSIS and TAKOTSUBO CARDIOMYOPATHY –
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
59-year-old female with a history of 1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house. EKG showed ST elevation in V4 and V5.
CXR showed LAE and LVE mild congestion, and left lower lung nodule.
Elevated troponin necessitated cardiac cath which showed normal coronaries and apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Echo showed EF of 50% and apical hypokinesis.
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
She has a past history of similar chest pain 2 years ago with negative cardiac workup. She has a history sarcoidosis (cutaneous, ocular and pulmonary). ACE level was 89 (normal 8-53)
3 years prior a CT showed hilar adenopathy and skin biopsy showed sarcoidosis. A CT 2 years prior to admission showed increasing hilar adenopathy and bronchiolectasis in the RUL and multiple upper lobe pulmonary nodules. Exercise tolerance test was negative 2 years ago.
Ashley Davidoff MD
DAY 3
Elevated troponin necessitated cardiac cath which showed normal coronaries.

Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD
{kind=link}
{kind=link}
Ashley Davidoff MD
LV ventriculography showed apical hypokinesis/dyskinesis consistent with Takotsubo heart. EF was 40%
Ashley Davidoff MD
Chest CT showed multiple non calcified nodules, increased since prior studies, and increase in mediastinal and hilar adenopathy, as well as abdominal adenopathy. Coronary calcification was present
MRI showed normal EF, with apical hypokinesis, findings consistent with Takotsubo heart.
TAKOTSUBO CARDIOMYOPATHY –
Ashley Davidoff MD
TAKOTSUBO CARDIOMYOPATHY –
Ashley Davidoff MD
Suboptimal study but no obvious ischemic disease
Ashley Davidoff MD
Thus this lady has a diagnosis of sarcoidosis (ocular skin and likely pulmonary)and Takotsubo cardiomyopathy precipitated by an acute emotional stress when the policE visited her home looking for men in her basement.
She presented with acute coronary syndrome, ST segment changes on EKG, mildly elevated troponins, CHF on CXR, with normal coronary arteriography and LV gram characteristic of Takotsubo cardiomyopathy
-
References and Links