
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
37-year-old female with a history of hypertrophic cardiomyopathy presented to the ER with pleuritic chest pain
CXR showed cardiomegaly with evidence of left ventricular enlargement and left atrial enlargement.

CXR shows cardiomegaly with evidence of left ventricular enlargement and left atrial enlargement.
Ashley Davidoff MD
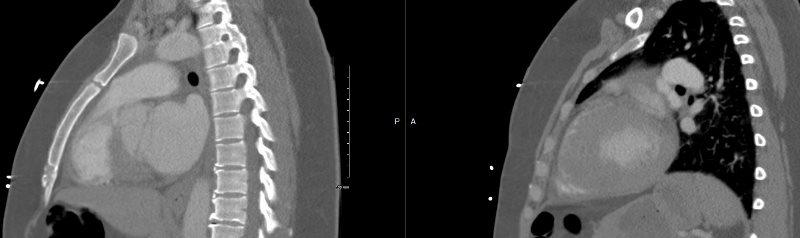
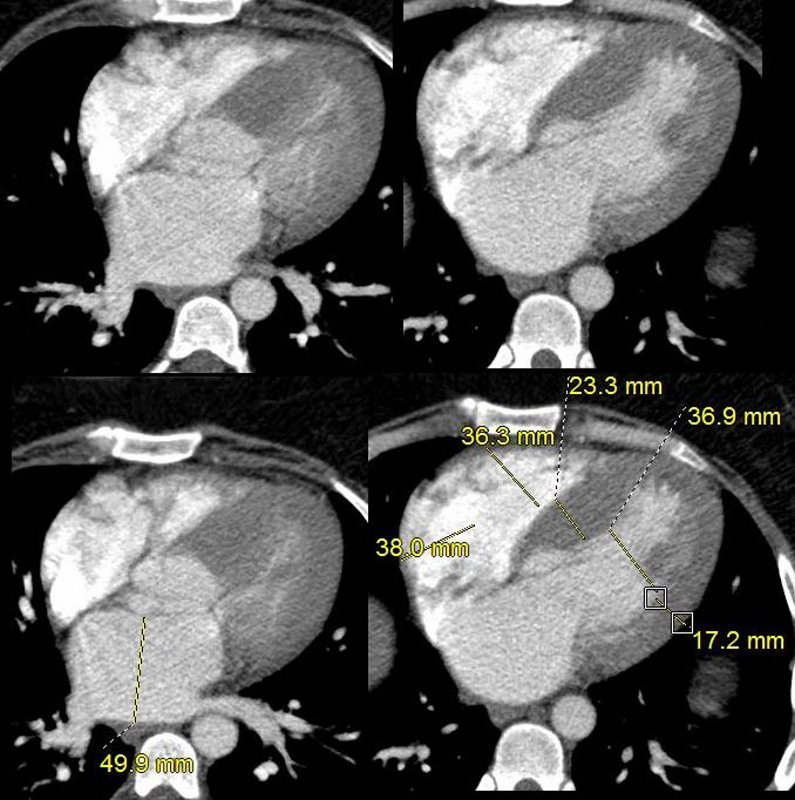
CTA showed no evidence of PE but confirmed the presence of LAE and LVH with asymmetric septal thickening and relative sparing of the apex.

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
A pyrophosphate scan was negative for amyloidosis

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
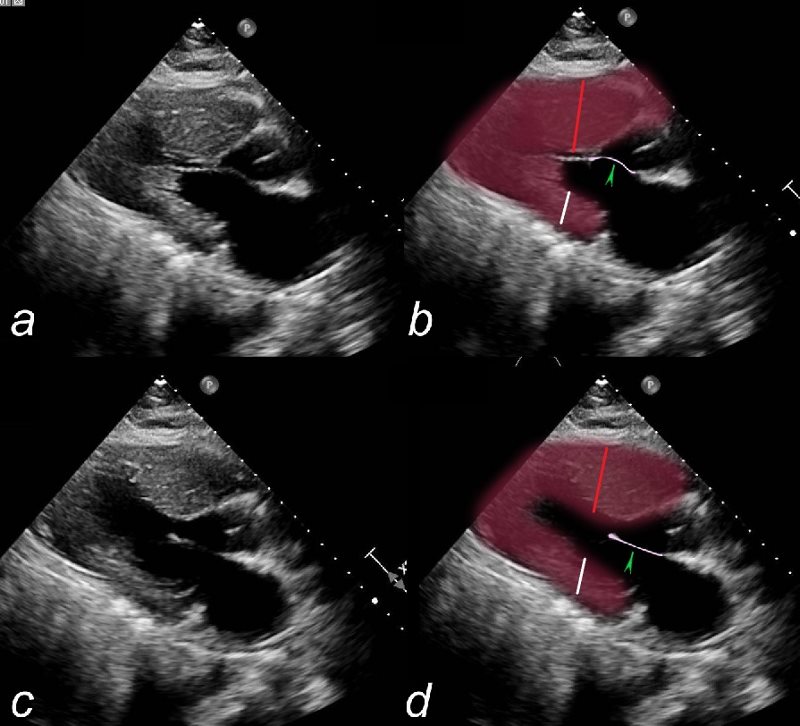
An echocardiogram confirmed the presence of an obstructive cardiomyopathy with systolic anterior motion of the mitral valve and late systolic mitral regurgitation. The left atrium was enlarged and the right atrium was mildly enlarged. The ejection fraction was normal and estimated to be between 64%. There was a resting gradient across the outflow tract of 40-68 mmHg. LV mass index was 156g/sq m
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Image a and b are in systole and show systolic anterior motion of the mitral valve into the LVOT (green arrowhead). In diastole the anterior leaflet is open (d green arrowhead)
Note also the relative thickness of the septal wall (red line) compared to the free wall (white line).
Ashley Davidoff MD

An echocardiogram confirmed the presence of an obstructive cardiomyopathy with systolic anterior motion of the mitral valve and late systolic mitral regurgitation. The left atrium was enlarged and the right atrium was mildly enlarged. The ejection fraction was normal and estimated to be between 64%. There was a resting gradient across the outflow tract of 40-68 mmHg. LV mass index was 156g/sq
Ashley Davidoff MD
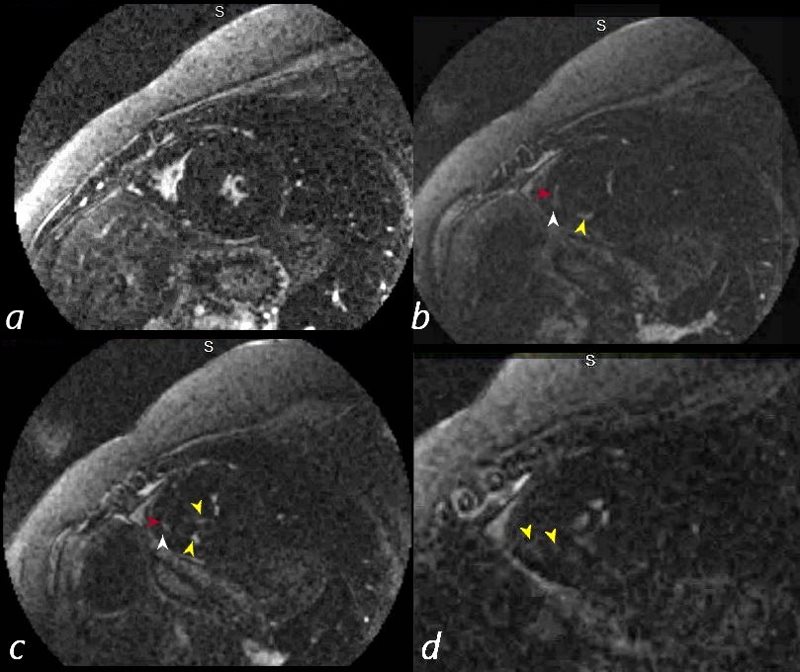
MRI confirmed the findings of the echo showing asymmetric septal hypertrophy, systolic anterior motion of the mitral valve with mitral regurgitation. The LA was 5.2cms, septal wall in diastole was 27.6mms and free wall was 16.8 mms. LV cavity size in diastole was normal. RA and RV were normal. EF was 70% and LV mass was 130g/ sq. m

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD

Ashley Davidoff MD

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD

RELATIVE SPARING OF THE APEX
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
37-year-old female with a history of hypertrophic cardiomyopathy presented to the ER with pleuritic chest pain
CXR showed cardiomegaly with evidence of left ventricular enlargement and left atrial enlargement.
CTA showed no evidence of PE but confirmed the presence of LAE and LVH with asymmetric septal thickening and relative sparing of the apex.
A pyrophosphate scan was negative for amyloidosis
An echocardiogram confirmed the presence of an obstructive cardiomyopathy with systolic anterior motion of the mitral valve and late systolic mitral regurgitation. The left atrium was enlarged and the right atrium was mildly enlarged. The ejection fraction was normal and estimated to be between 64%. There was a resting gradient across the outflow tract of 40-68 mmHg. LV mass index was 156g/sq m
MRI confirmed the findings of the echo showing asymmetric septal hypertrophy, systolic anterior motion of the mitral valve with mitral regurgitation. The LA was 5.2cms, septal wall in diastole was 27.6mms and free wall was 16.8 mms. LV cavity size in diastole was normal. RA and RV were normal. EF was 70% and LV mass was 130g/ sq. m
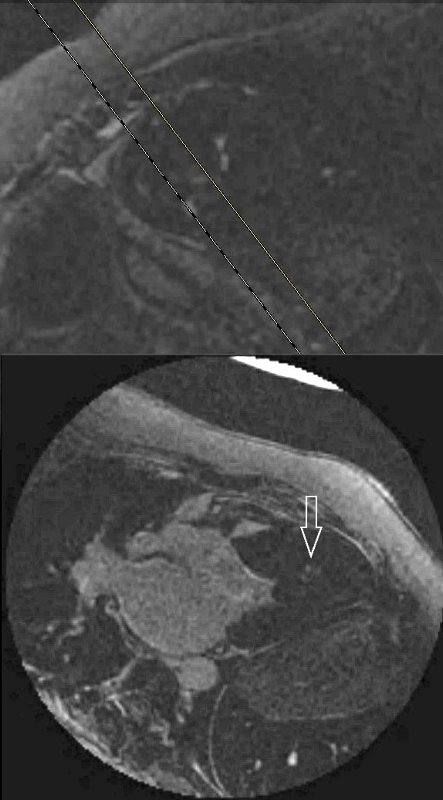
Nodular LGE was noted in the mid myocardium in the inferoseptal region at the hinge points and at the antero-apical regions
Ashley Davidoff MD
Nodular LGE was noted in the mid myocardium in the inferoseptal region at the hinge points and at the antero-apical regions
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD

ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD
ASYMMETRIC HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
Ashley Davidoff MD