
48-year-old man with a previous history of sudden loss of vision which subsequently resolved and presents now with near syncope, atrial fibrillation.
CXR

CXR shows LAE and LVE with cephalisation
Ashley Davidoff MD
BRAIN MRI Diffusion Sequence
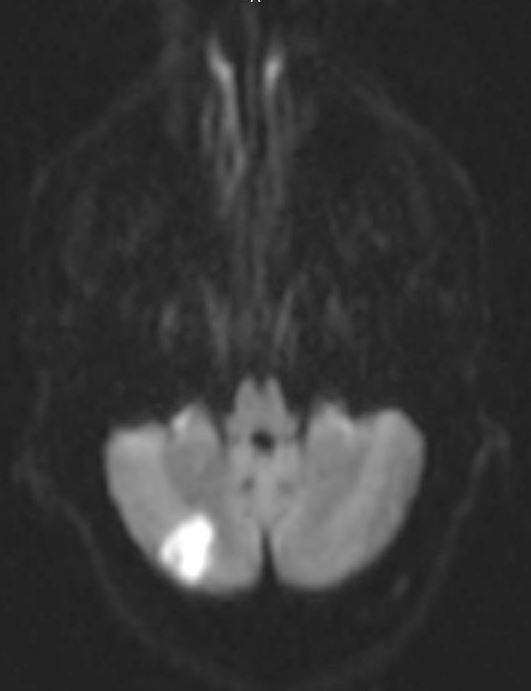
MRI showed acute embolic infarct involving the cerebellum.
Ashley Davidoff MD
Echocardiogram showed an enlarged left atrium, significant left ventricular hypertrophy, and moderate mitral regurgitation.
Correlation of Frontal CXR with Coronal MRI
Triangular Heart and “Straight Heart Border – A Large MPA and Atrial Appendage and LArge LA
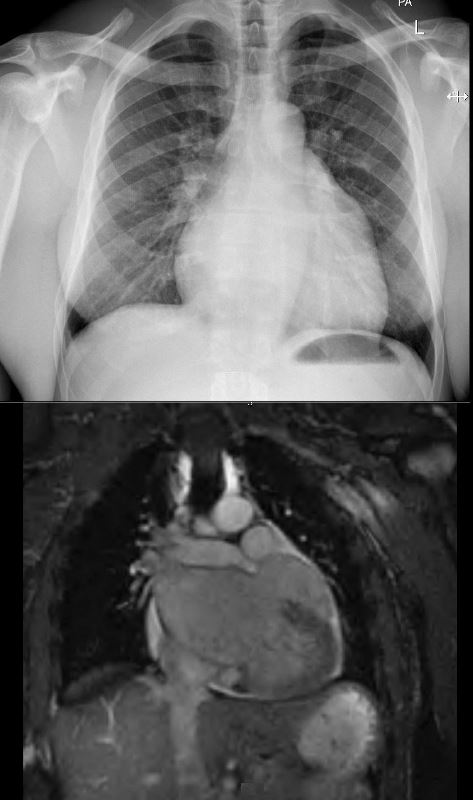
CXR shows triangular heart large MPA, LAE and enlarged left atrial appendage with cephalisation, most suggestive of mitral stenosis. Coronal MRI confirms the presence of LAE and very large left atrial appendage
Ashley Davidoff MD
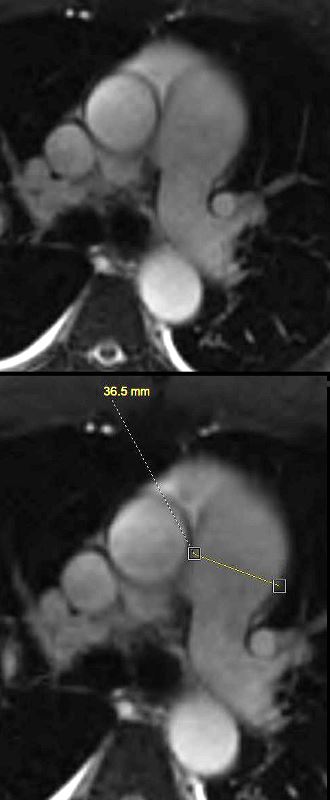
Axial MRI confirms the presence of an enlarged PA with a diameter of 36.5mm (normal up to 30mms)
Ashley Davidoff MD
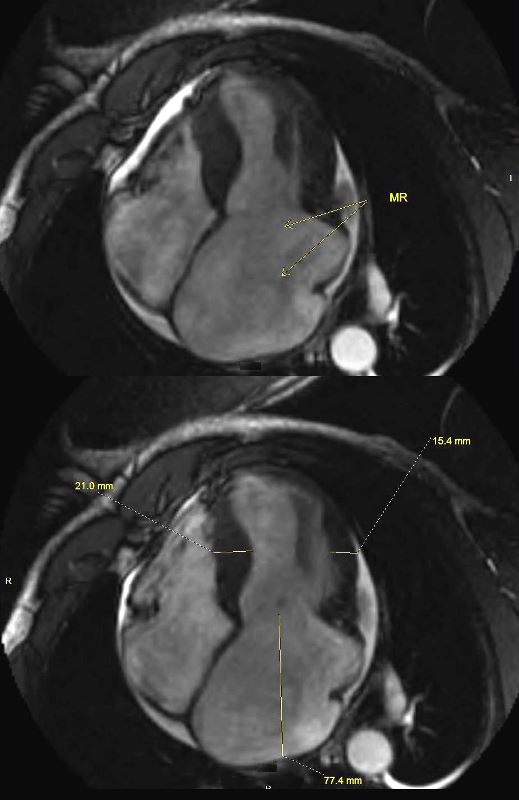
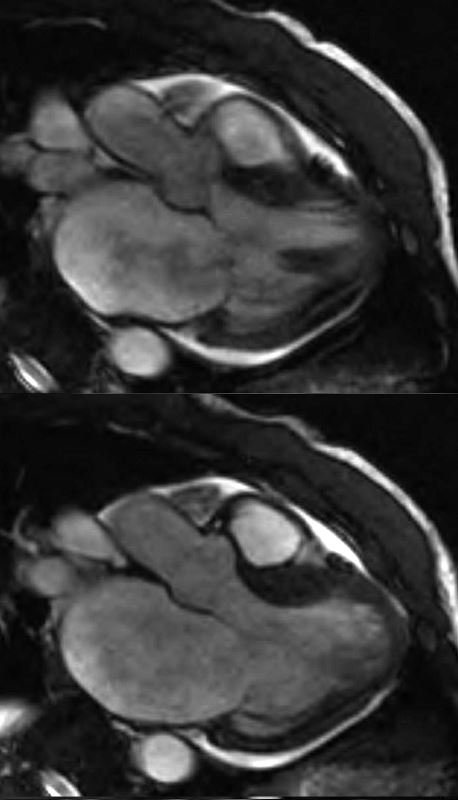
The MRI (systole above and diastole below) shows moderate mitral regurgitation, (arrows in top image showing turbulence )and bottom image showing significant left atrial enlargement (A-P dimension 77.4mms) LVH (septum 21 mms and free wall 15.4 mms) Calculated LV mass was LVH 95 gms/sq m) (normal = 50-86 g for males) On cine studies there was diffuse hypokinesis with EF of 39%,
Ashley Davidoff MD
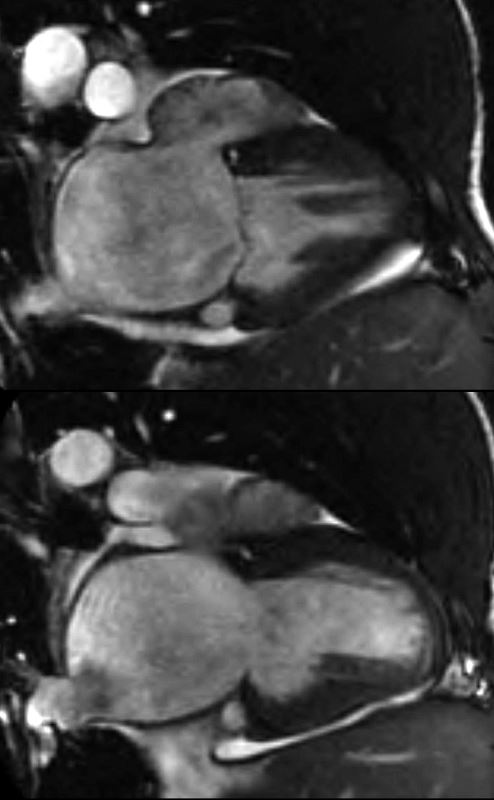
MITRAL REGURGITATION IN 2 CHAMBER VIEW
The MRI (systole above and diastole below) shows moderate mitral regurgitation, ( top systolic image showing turbulence with flow void) and both images showing significant left atrial enlargement. On cine studies there was diffuse hypokinesis with EF of 39%, Ashley Davidoff MD
MITRAL REGURGITATION IN 3 CHAMBER VIEW
The MRI (systole above and diastole below) shows moderate mitral regurgitation, ( top systolic image showing turbulence with flow void) and both images showing significant left atrial enlargement. On cine studies there was diffuse hypokinesis with EF of 39%, Ashley Davidoff MD
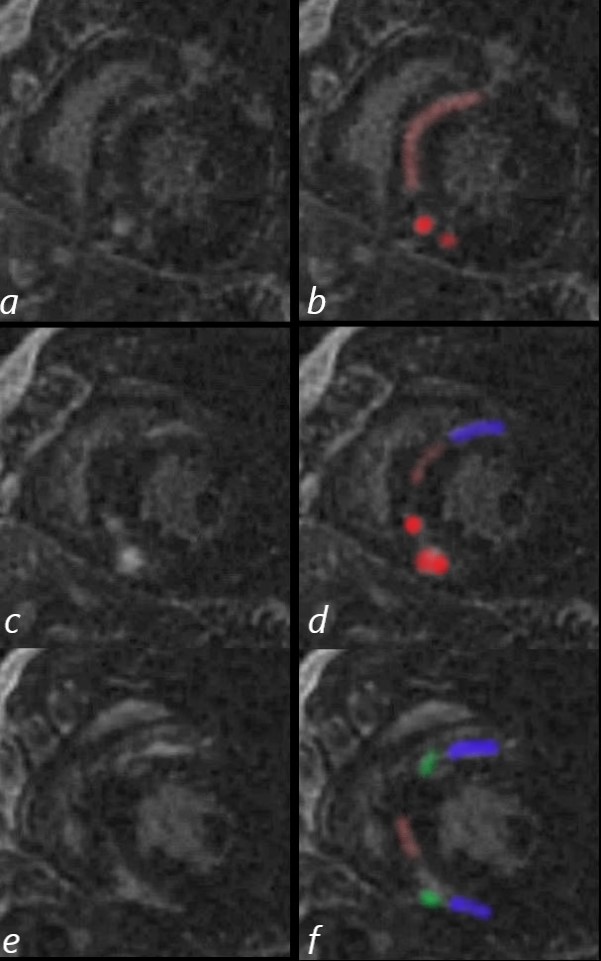
The cardiac MRI in short axis (native form (a,c,e) and with color correlative overlays (b,d,f) shows multifocal linear and nodular LGE at the hinge points (green f) in the subepicardial regions (blue d,f) at the base of the heart anteriorly and inferiorly, as well as mid myocardial linear LGE in the septum (pink d,f). The bright LGE is dominant in the nodular form (red b,d)
Sarcoidosis is thought to be most likely based on the multifocal nodular disease, as well as the subepicardial location. Distribution of LGE is not characteristic of Fabry disease. Amyloidosis is also considered as a less likely possibility
Ashley Davidoff MD
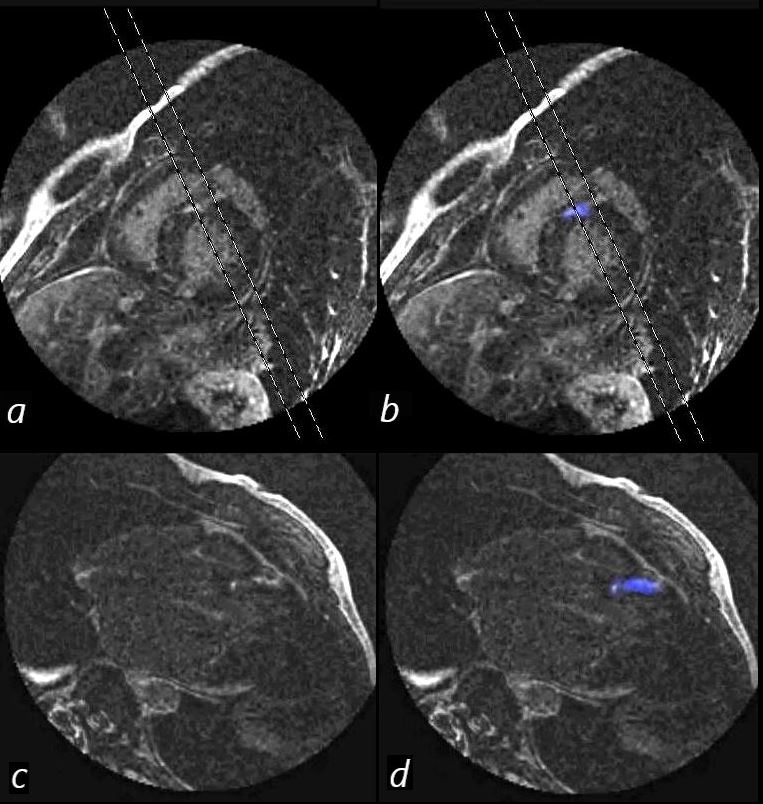
The cardiac MRI in short axis (a,b) is correlated with the long axis (c.d) . Linear subepicardial distribution in the anteroseptal region is demonstrated with blue overlay (b,d,f) .
Sarcoidosis is thought to be most likely based on the multifocal nodular disease, as well as the subepicardial location. Distribution of LGE is not characteristic of Fabry disease. Amyloidosis is also considered as a less likely possibility
Ashley Davidoff MD
References and Links
Case Studies Map