
Inflammation
The Common Vein copyright 2009
Definition
Inflammation is a protective physiological response initiated when the body is exposed to harmful stimuli, such as pathogens and irritants, or as a result of an autoimmune response. It may result in either a helpful or harmful process. When it is helpful to the body it is considered a healing process but when it is more harmful to the body it may be considered a disease or a disorder.
At a histological level, the process results in the stimulation of macrophages at the site of the injury, including dendritic cells, endothelial cells, and mastocytes, which release inflammatory mediators that generate a cascade of events within the body. These events may be categorized into a vascular and a cellular response, each of which ultimately serves to clear the body of invading pathogens or irritants and/or to begin the process repairing damaged tissue.
The vascular response is mediated largely by vasodilators, inflammatory mediators that cause an increase in blood flow to the injured region, leading to the characteristic redness and heat of inflammation. Vasodilators also cause increased permeability of vascular walls, allowing plasma to move into the surrounding tissue. This mechanism leads to swelling and serves to dilute the pathogen or irritant that triggered the response. There are also a variety of plasma-derived cascade systems that use different sets of mediators to develop and propagate the inflammatory response. These include the complement system, which increases removal of pathogens, the kinin system, which propagates vasodilation, the coagulation system, which initiates clotting at the site of injury, and the fibrinolysis system, which counterbalances clotting.
The cellular component of the inflammatory response occurs as a direct result of the vascular response and results in an increased concentration of leukocytes at the site of injury. Leukocytes, immune cells that include phagocytes, granulocytes, monocytes, and lymphocytes, are designed to destroy invading pathogens, making them invaluable components of the inflammatory response. Normally leukocytes are not provided much opportunity to move from blood vessels into tissue, as the flow of blood moves them swiftly through the blood vessels. Following the vascular response, however, the concentration of cells in the blood increases and the speed of blood flow decreases, allowing leukocytes to extravasate into surrounding tissue at an increased rate. Once in the tissue the process of chemotaxis gradually directs them toward the site of injury where they may finally go to work destroying pathogens.
Finally, inflammation may be classified as either acute or chronic. Acute inflammation is characterized by immediate onset in response to injury or the presence of pathogens and persists only as long as that injury or pathogen persists. In contrast, chronic inflammation is a delayed response to persistent foreign bodies, non-degradable pathogens, or an autoimmune response and can last for months or years.
Inflammation may be diagnosed by a variety of methods depending on the symptoms described by the patient. For instance, inflammation due to a puncture wound may only require a physical examination while abdominal pain caused by an inflamed appendix or an autoimmune disease would likely require a more in-depth battery of tests and imaging techniques.
Acute inflammation is typically treated with short-acting anti-inflammatory agents, such as ________, and antibiotics to prevent infection. Treatment of chronic inflammation is more complicated, often requiring longer-lasting anti-inflammatory drugs, such as steroids and _______. Finally, inflammation caused by autoimmune disease requires a more comprehensive treatment plan designed to reduce inflammation and prevent tissue damage over the course of a patient?s life.
Celsus 200 years ago ? rubor calor dolor tumor laesio function (Virchow (1821 -1902
Hyperemia calor

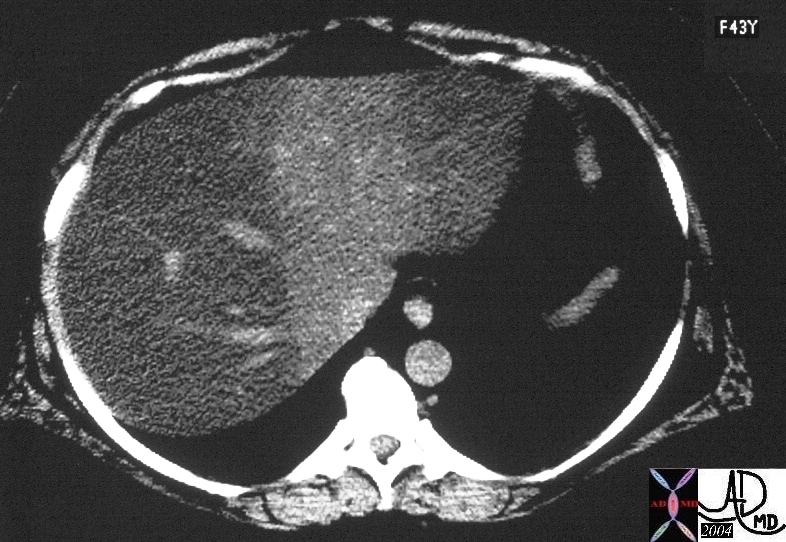
Radiation Hepatitis ? Hyperemia
The straight line and the hyperemia are characteristis features radiation induced change22975 Courtesy Ashley Davidoff MD
Principles
Acute Inflammation
Hallmarks ? Celsius
Tumor
Rubor
Calor
Dolor
Laesio Functio
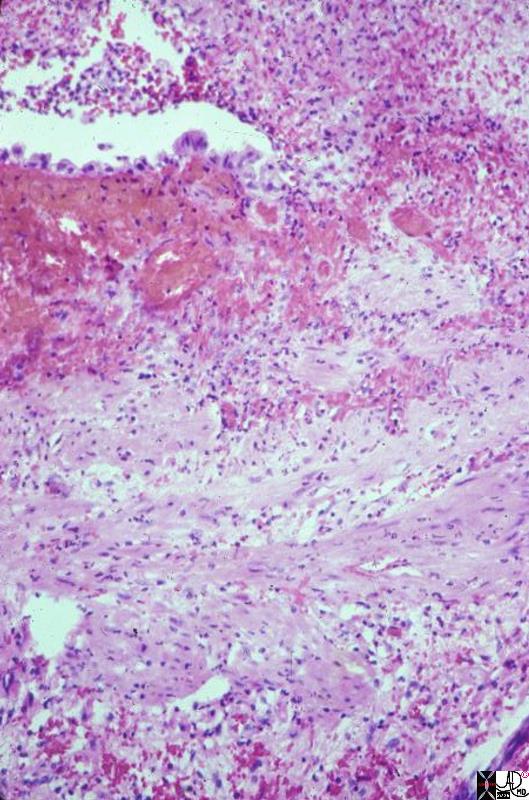
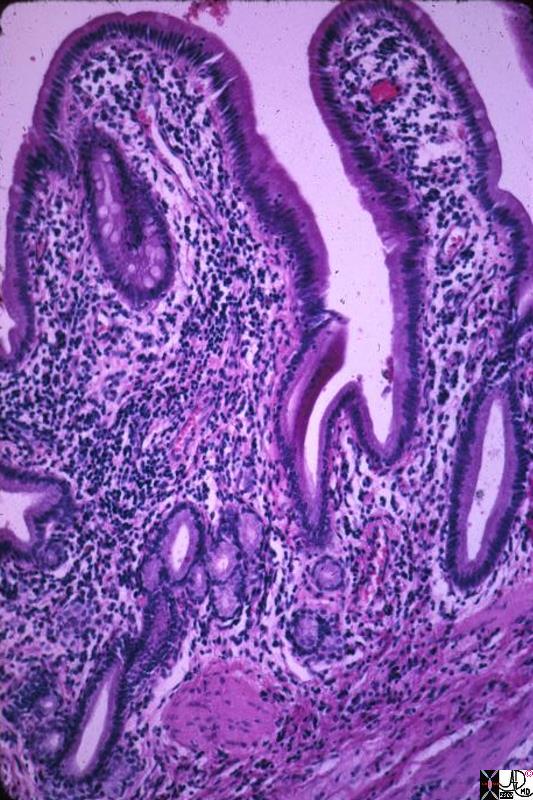
Acute Cholecystitis
This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall.11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD
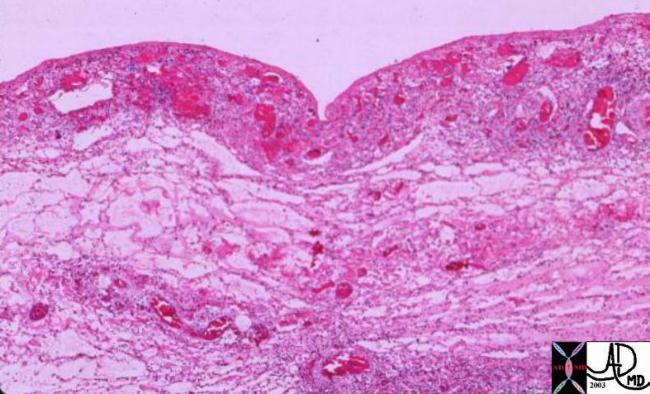
Hemorrhagic Congestion in the Gallbladder Wall
00151 gallbladder wall inflammation acute cholecystitis histopathology
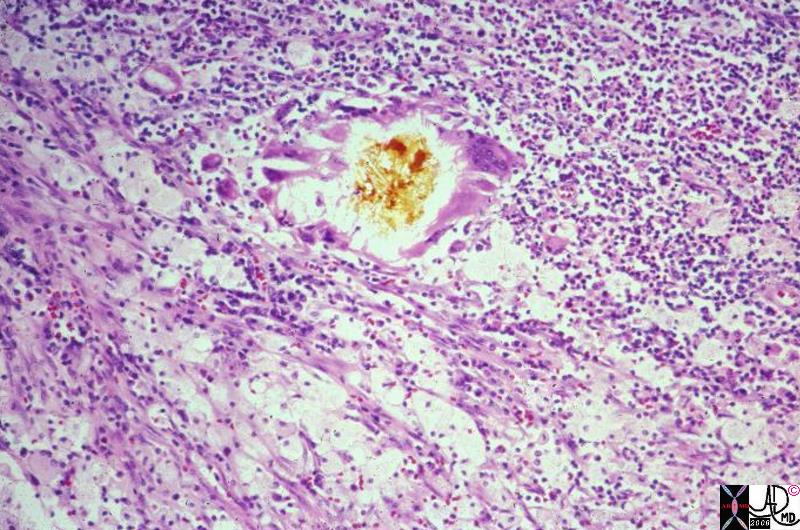
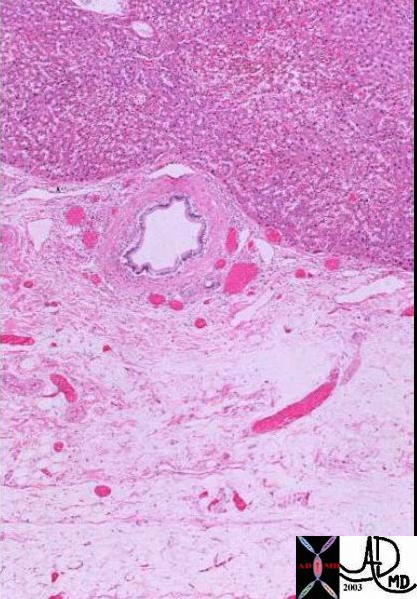
Bile Inciting Inflammation
This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The ?granulomas? are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD

Acute Calculous Cholecystitis
This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 ? 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction.11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD
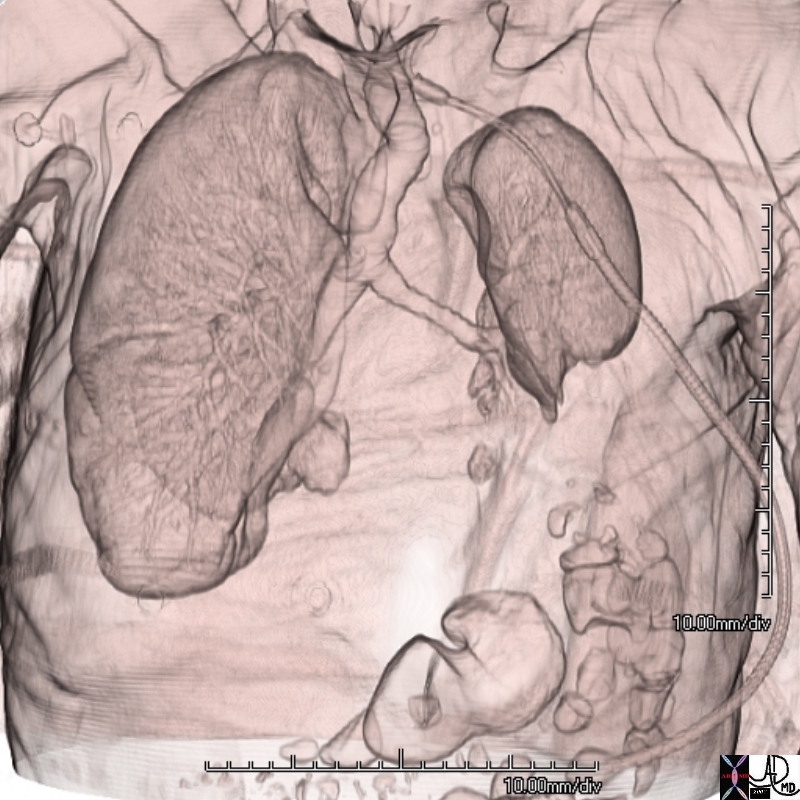
Cystic Arterioles in the Submucosa ? Hyperemia
82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
Cystic Arterioles and Venules in the Submucosa
82006c05.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
Arteries, Veins and Lymphatics in the Gallbladder Fossa
00140 gallbladder wall gallbladder fossa normal artery duct liver interface histopathology
Swelling
Transudation and Exudation Causing Swelling |
| 71695c02 colon splenic flexure fx fat induration dirty fat Gerotas fascia lateral conal fascia thickened thickening of the interstitium acute inflammation inflammatory exudate diverticulitis large bowel CTscan Davidoff MD 71695c01 |
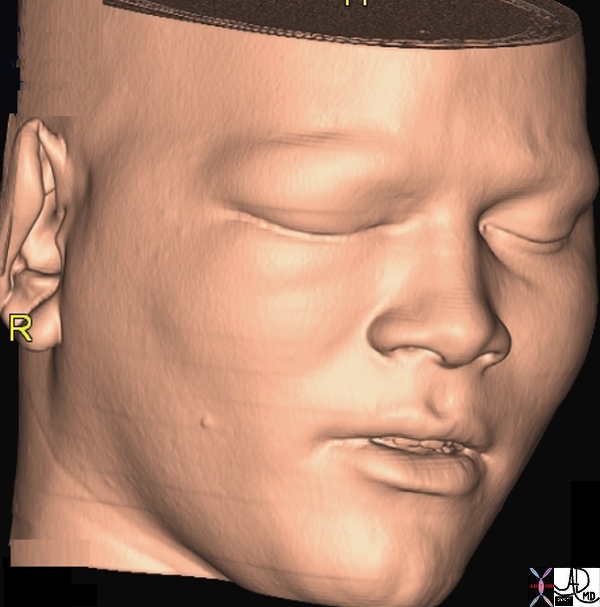
Swelling Supraorbital Region and Maxillary Sinus |
| 48717b01 skin bone swelling acute traumatic injury inflammation fracture inferior orbital wall roof of maxillary sinus trauma 3D volume rendering CTscan Davidoff MD |
Hyperemia
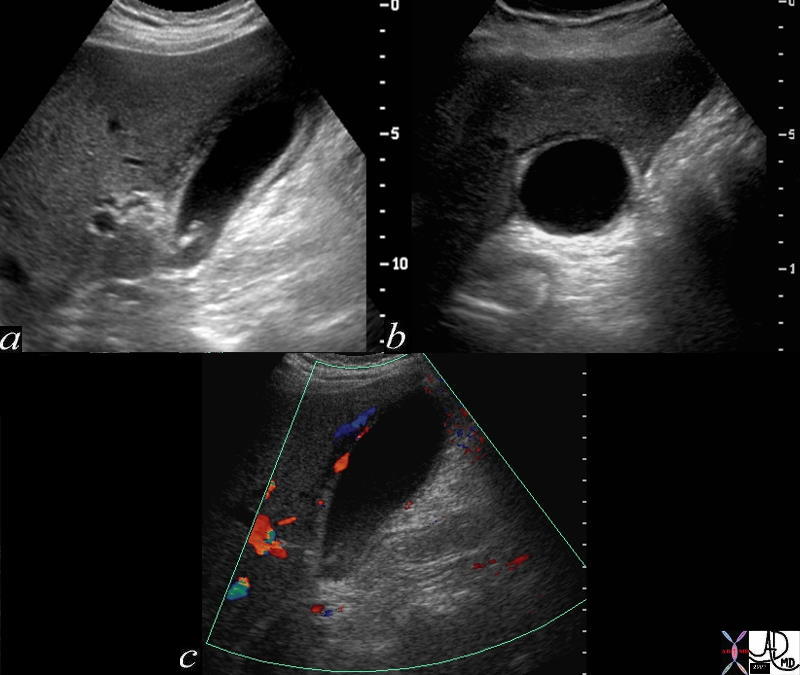 
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia |
| 72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy?s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD |
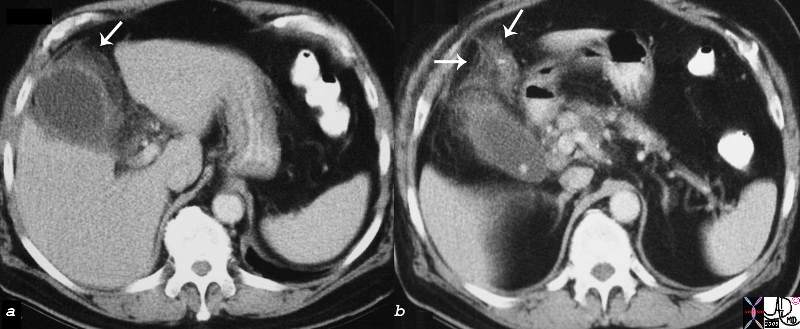
Acute Cholecystitis with Transmural Induration |
|
16203c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008
|
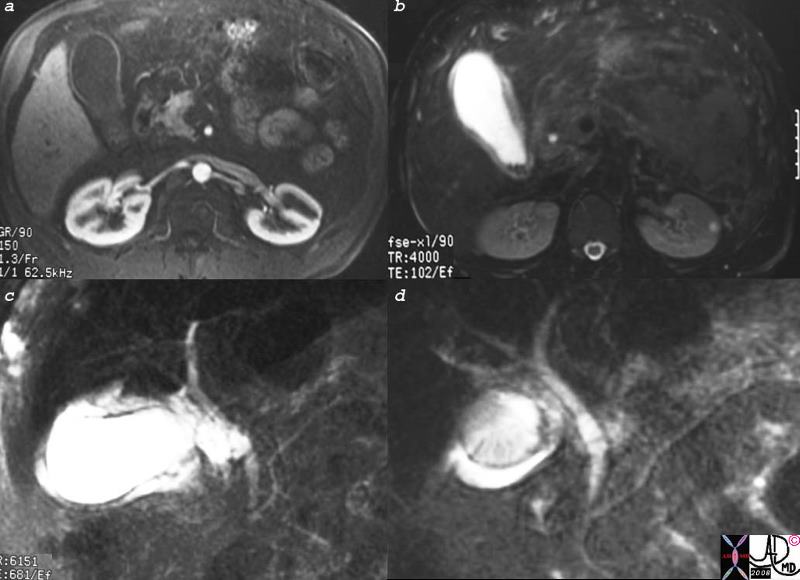
Acute Cholecystitis |
| 16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008 |
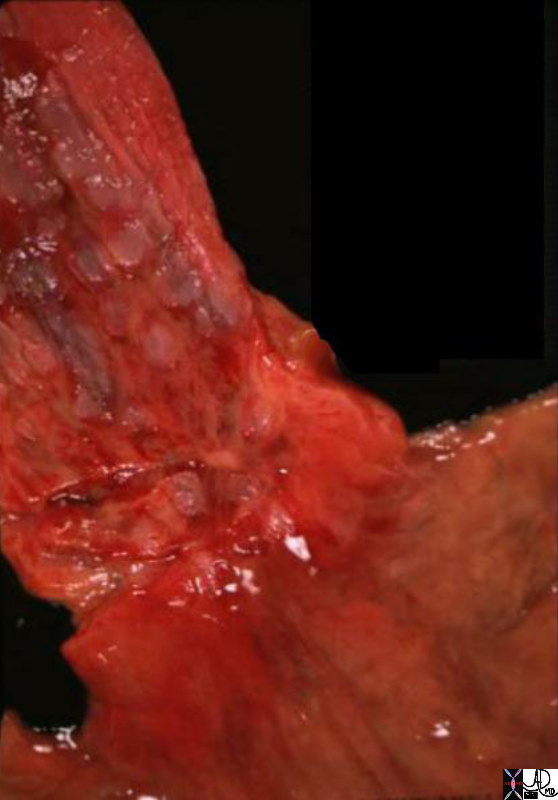
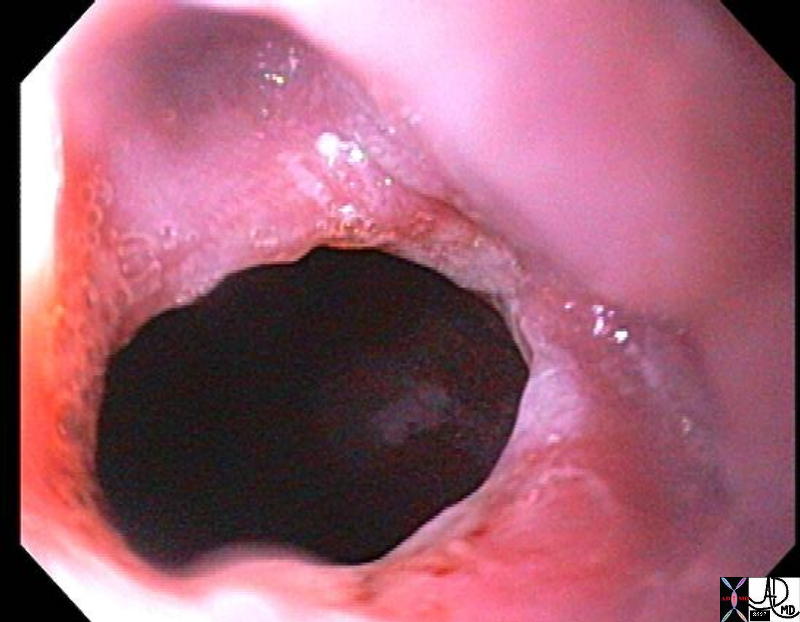
The Normal (left) and Abnormal (right) Red and Swollen GE junction ? Reflux Esophagitis |
| 01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD |

Chemical Peptic Esophagitis |
| 73405 esophagus redness patches inflammation chemical acute esophagitis endoscopy Courtesy Joshua Namias |
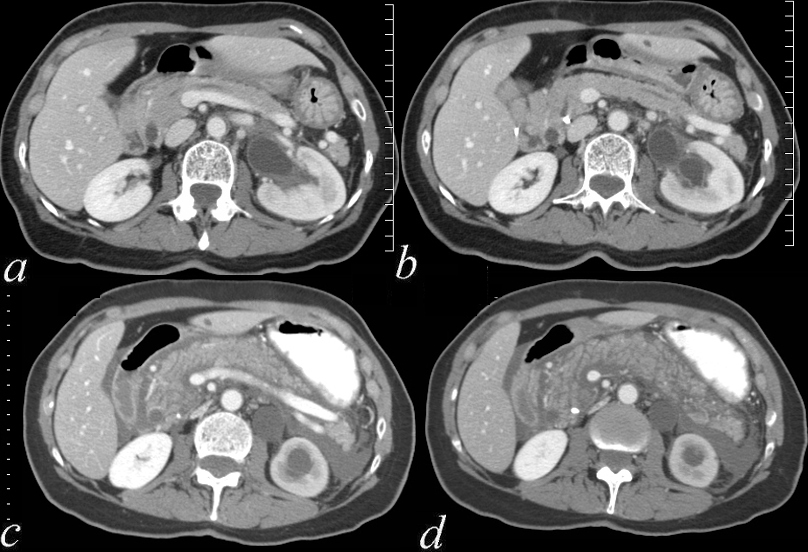  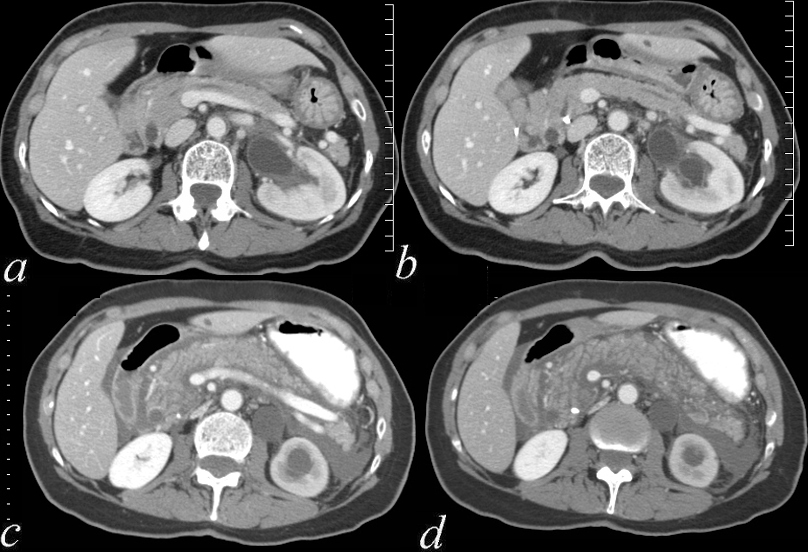
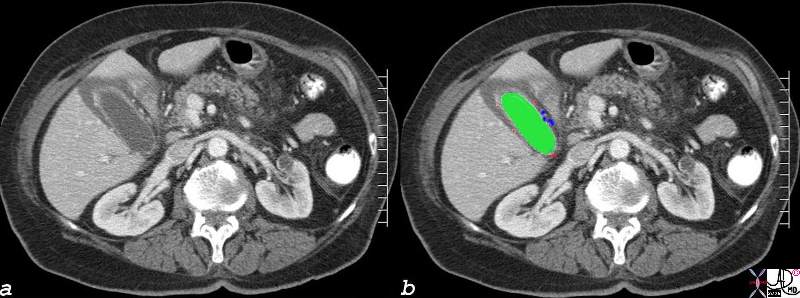
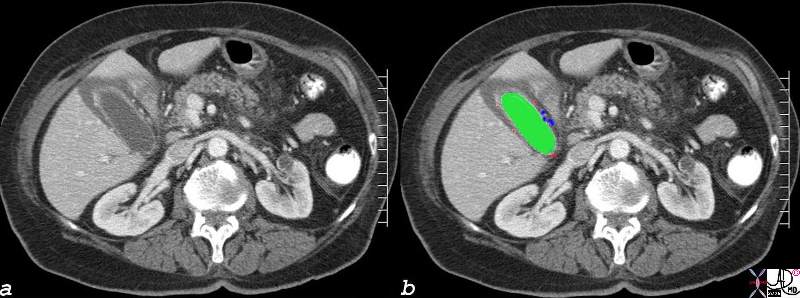
Before and After Acute Pncreatitis Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid |
| 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02 |
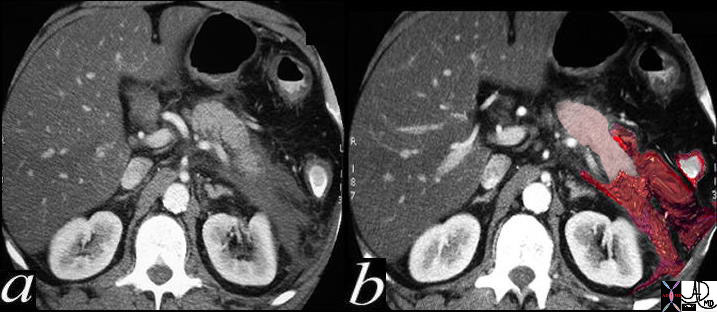
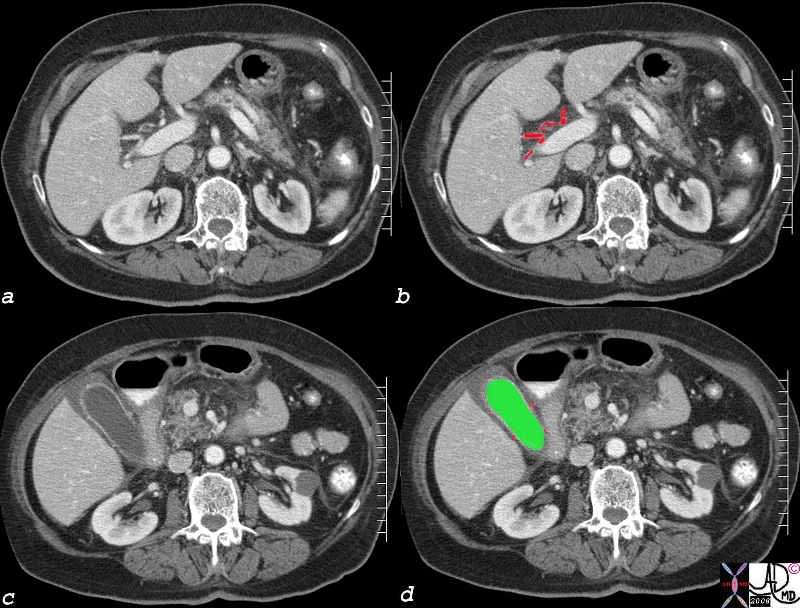
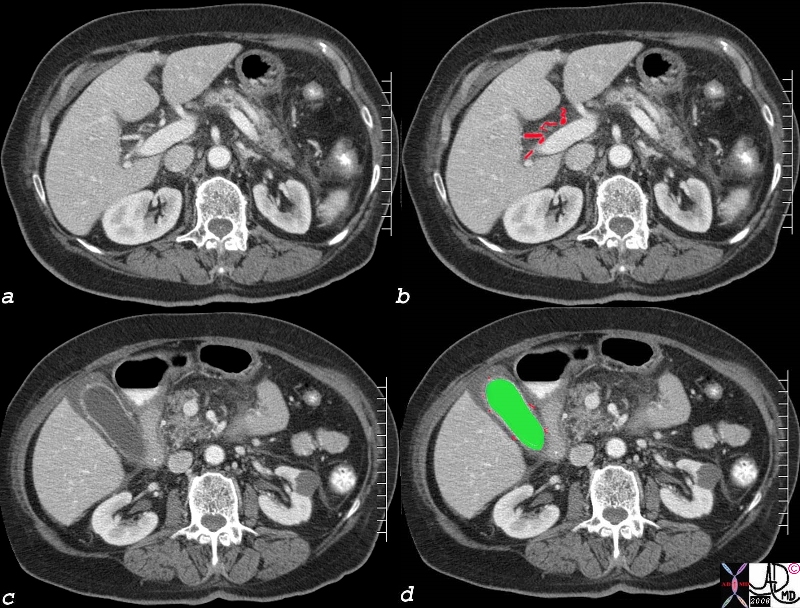
Acute Pancreatitis |
|
This patient presented with acute abdominal pain following an alcoholic binge. The pancreas shown in pink in image b, looks relatively normal, but is surrounded by a exudate (red ) which is characteristic of this entity. The exudate has extended around the colon (white surrounded by red ring on the left side) . 40396c02 Courtesy Ashley Davidoff MD code abdomen colon colon cutoff sign code pancreas pancreatic tail fx induration exudate code anterior pararenal space left colic gutter Gerota?s fascia lateral conal ligament fx thickened lcode liver hypodensity dx steatosis fatty liver code dx acute alcoholic pancreatitis with fatty change in the liver and colonic narrowing imaging radiology plain film CTscan acute inflammation mechanical |
Chemical Inflammation
|
Before and After Acute Pncreatitis Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid |
| 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02 |
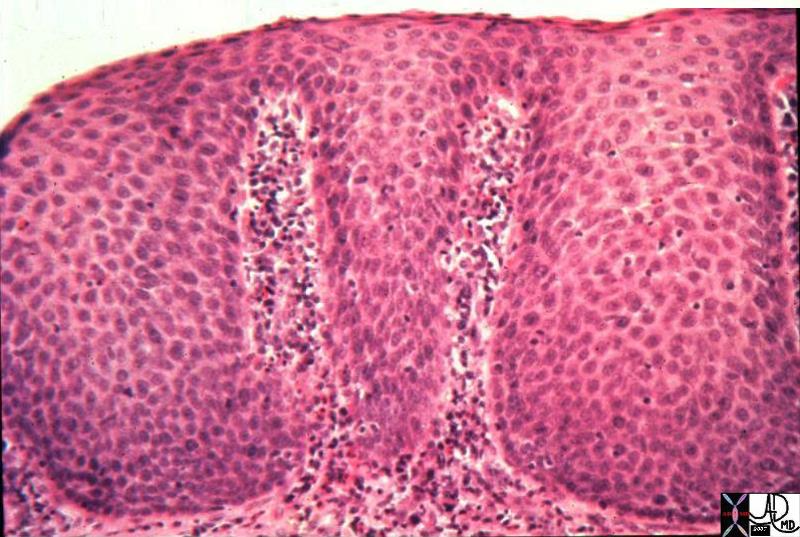
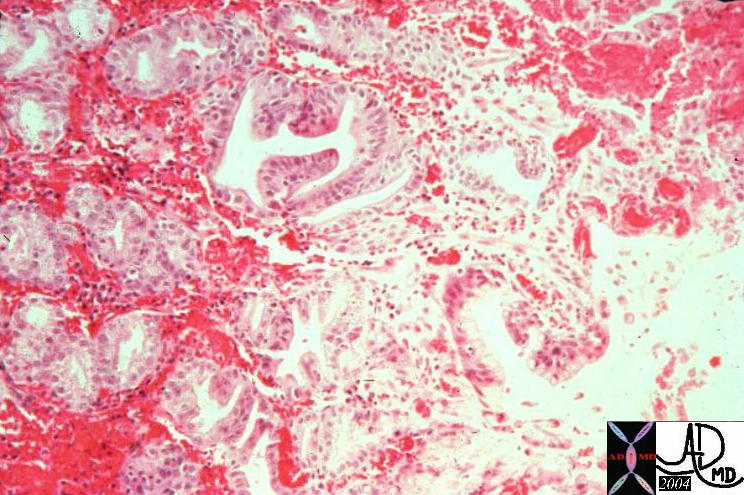
Reflux Esophagitis |
| 12253.800 esophagus cellular infiltrate inflammation stratified columnar epithelium reflux esophagitis histopathology Courtesy Barbara Banner MD |
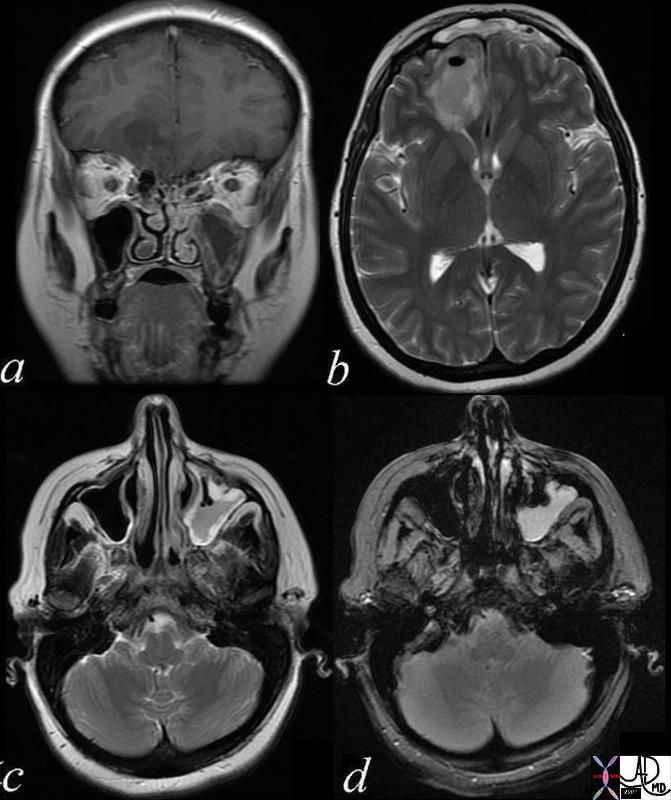
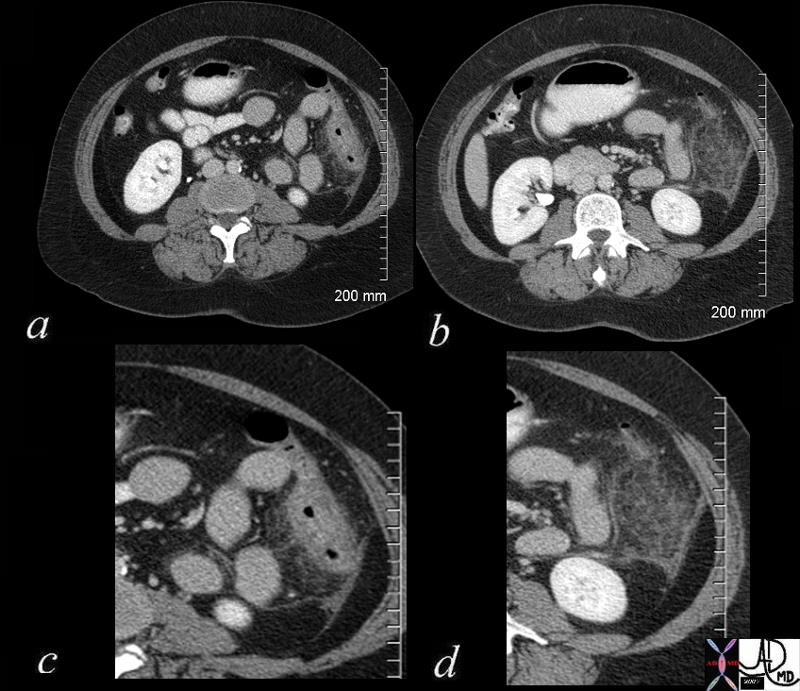
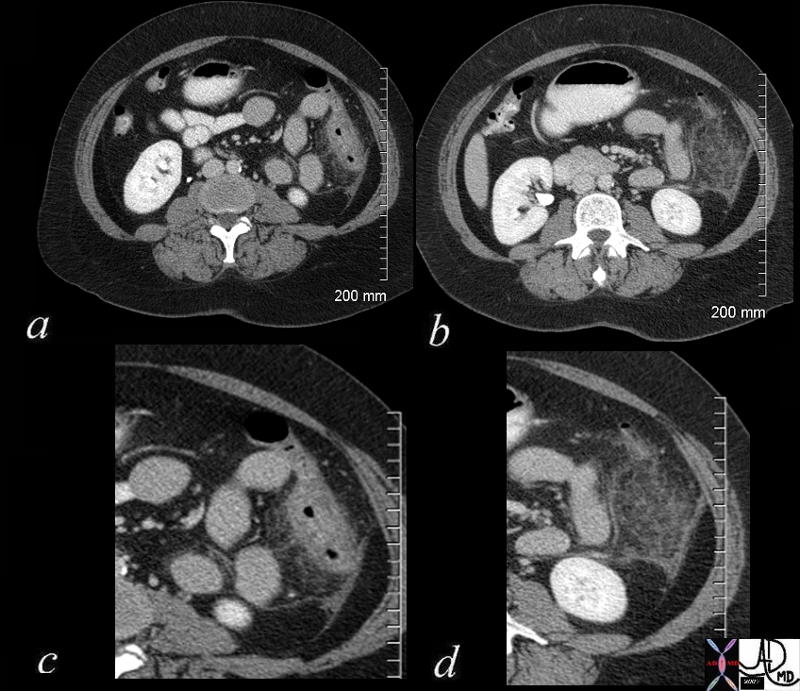
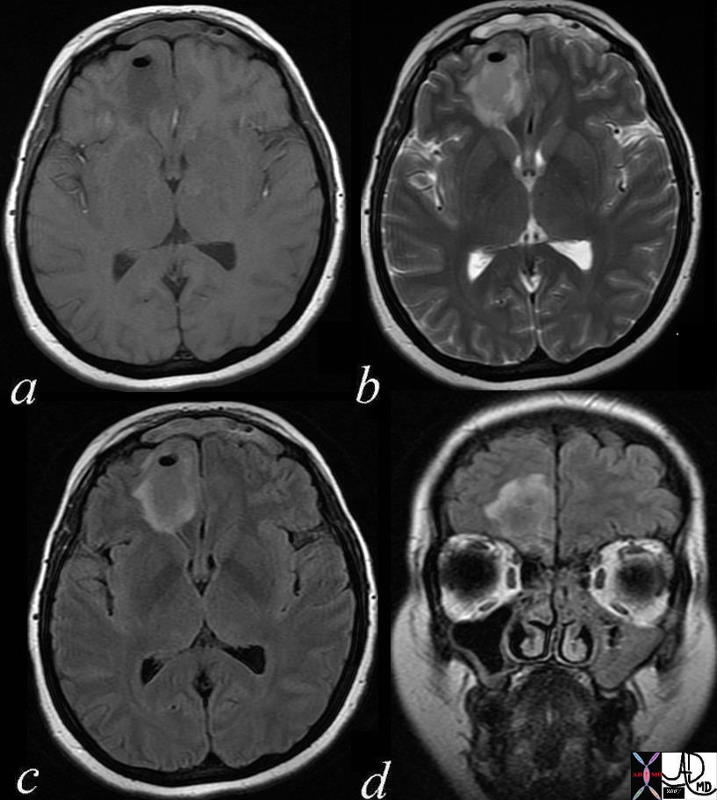
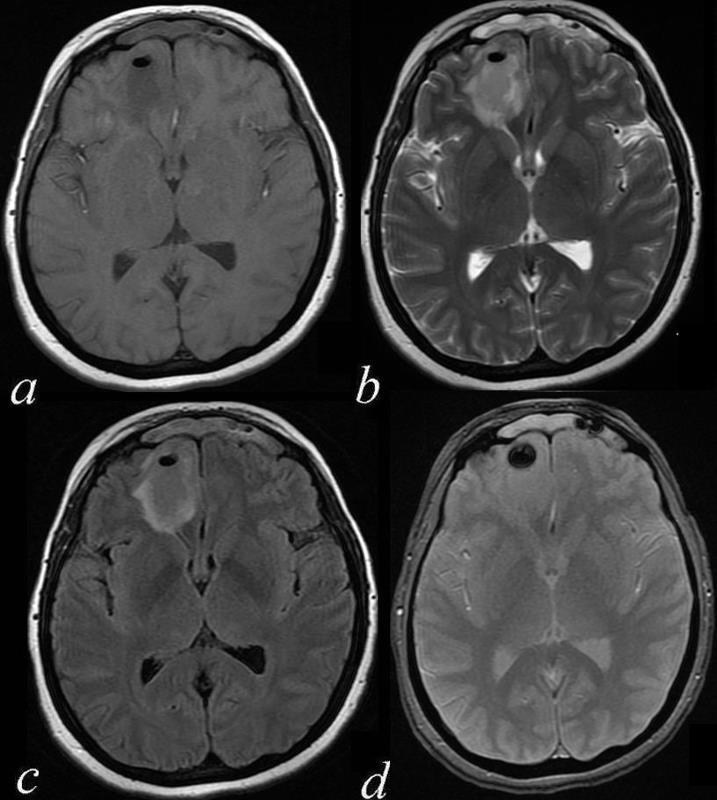
Left Maxillary Sinusitis Complicated by Brain Abscess ? MRI
71604.c03 40 year old female with headache brain maxillary sinus frontal lobe fx air fluid level parafalcine falx cerebri a= T1 weighted b= T2 weighted c = T2 weighted d= FLAIR dx acute on chronic left maxillary sinusitis with brain abscess air fluid level thickened mucosa of maxillary sinus MRI Davidoff MD 71604.c02 71604.c03 71604.c04 71604.c02b


CNS
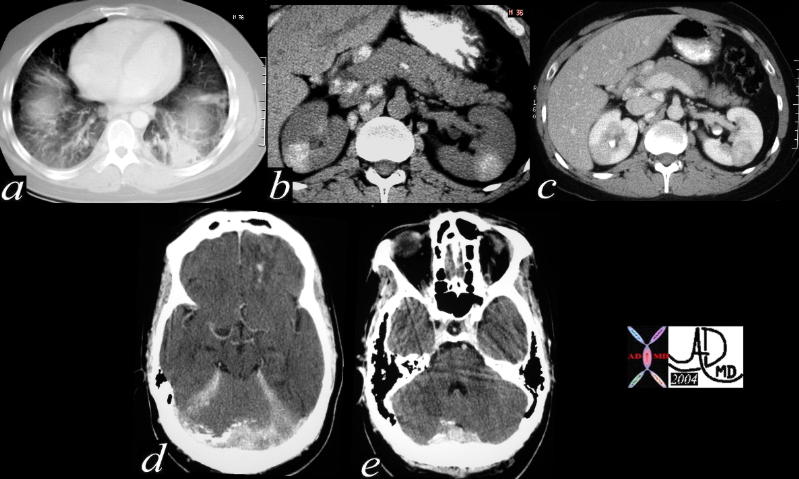
Sarcoidosis Involving the Basal Meninges |
| 40406c Courtesy Ashley Davidoff MD code lung fx interstium fx thickening dx interstitial lung disease ILD code pancreas abdomen lymph nodes fx calcified code brain meninges fx calcifications code dx sarcoidosis imaging radiology CT scan code inflammation immune |
CVS

Sarcoidosis of the Heart |
| 49740c01 34 male with sarcoidosis presents with dizzineess and complete heart block cardiac heart LV sarcoidosis complete heart blosk early gadolinium delayed gadolinium enhancement of the LV wall left ventricle inflammation MRI T1 Davidoff MD |
Calcific Myocarditis |
| This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 code heart septum dense calcific calcified calcification myocarditis inflammation cardiac imaging radiology CTscan |
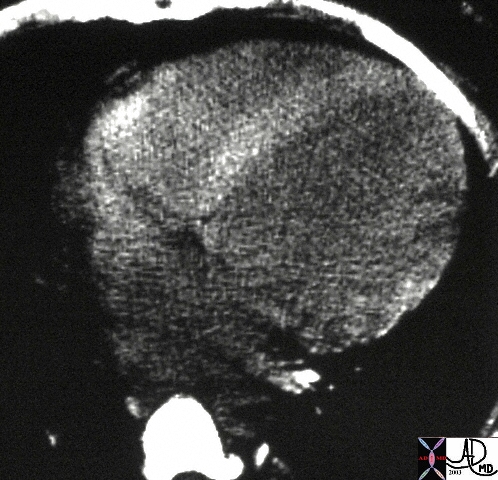
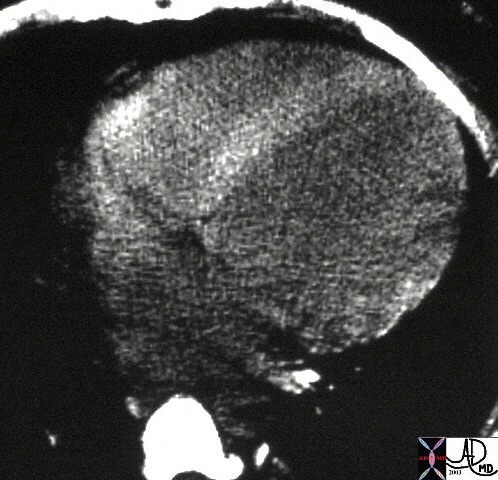
Takayasu?s Aortitis |
| 16917b aorta fx irregular fx narrow dx Takayasu arteritis imaging radiology MRI Courtesy Ashley Davidoff MD DB |
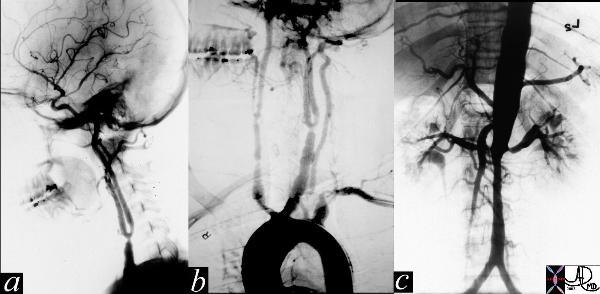
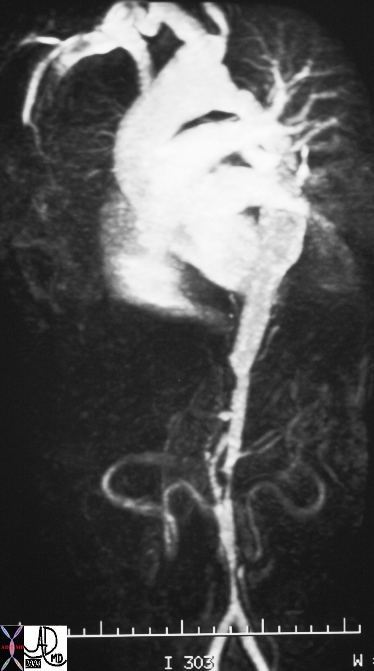
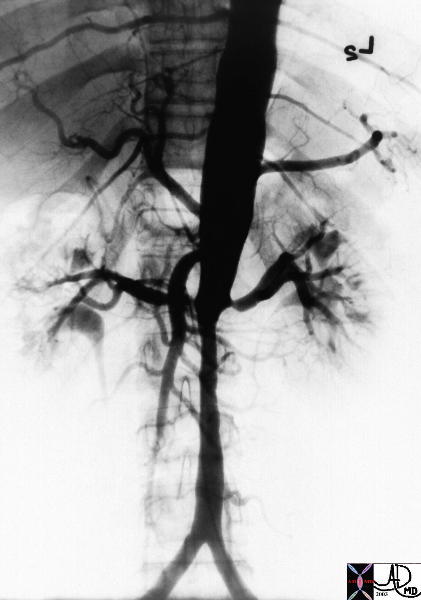
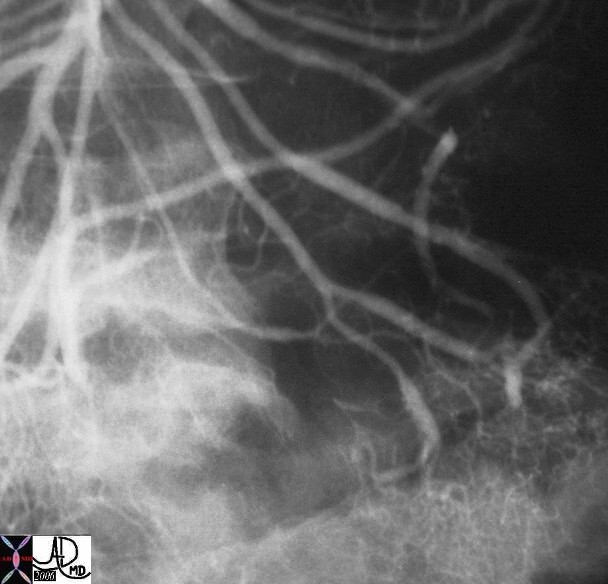
Takayasu?s Arterirtis |
| The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless |
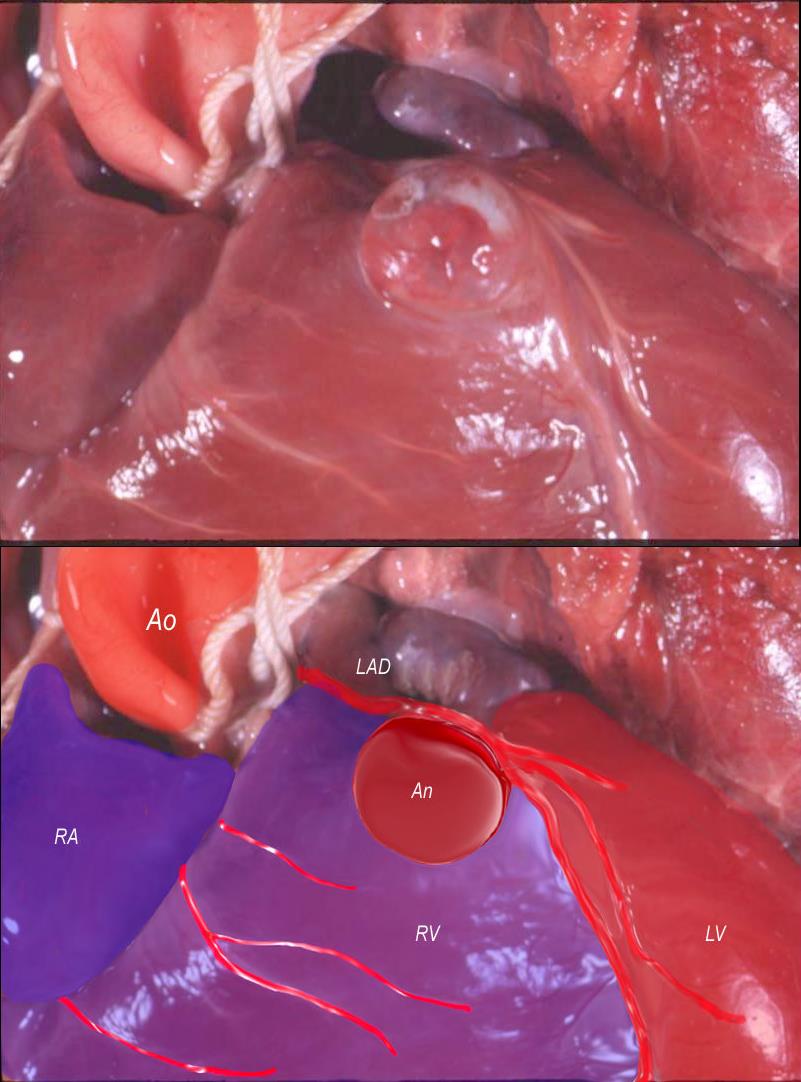 
Kawasaki Arteritis and Coronary Artery Aneurysm |
| 07587 heart cardiac aneursym coronary artery Kawasaki?s areteritis grosspathology Courtesy Ashley Davidoff MD |
|
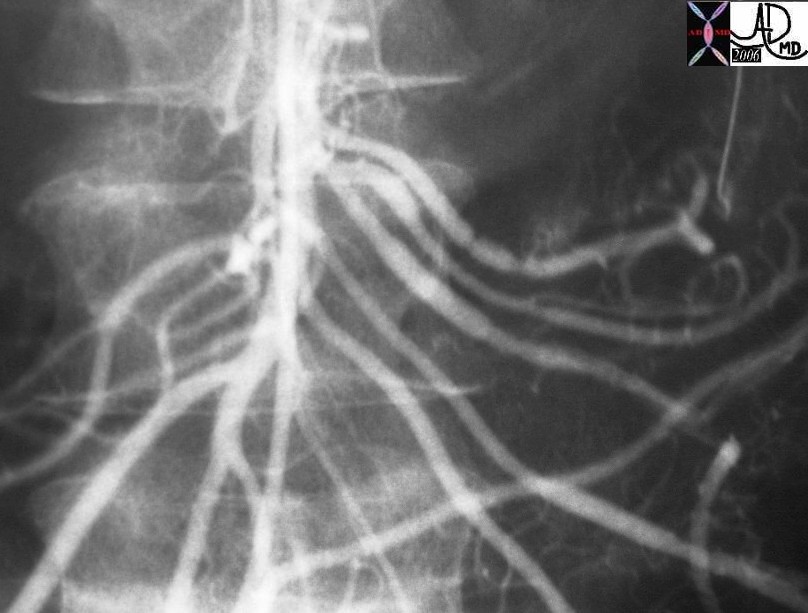
Takayasu?s Arterirtis |
| The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless |
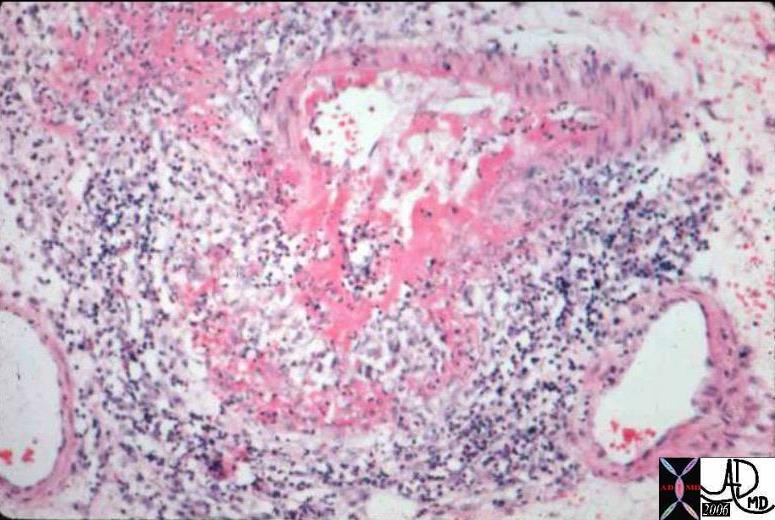
Polyarteritis Nodosa |
| Occlusive Vascular Disease: Causes of Vascular Occlusion ? Polyarteritis Nodosa. This is a medium power photomicrograph from a bowel in a patient with Polyarteritis Nodosa. Bowel is commonly affected in this disorder. The medium sized artery seen here has undergone a deeply eosinophilic (fibrinoid) change. Notice that there is a surrounding inflammatory infiltrate of WBCs and formation of aneurysmal dilatation. This can result in massive hemorrhage if the aneurysm ruptures. colon large bowel artery small bowel fx aneurysm inflammation dx polyarteritis nodosa histopathology Courtesy Barbara Banner MD 12889 |
 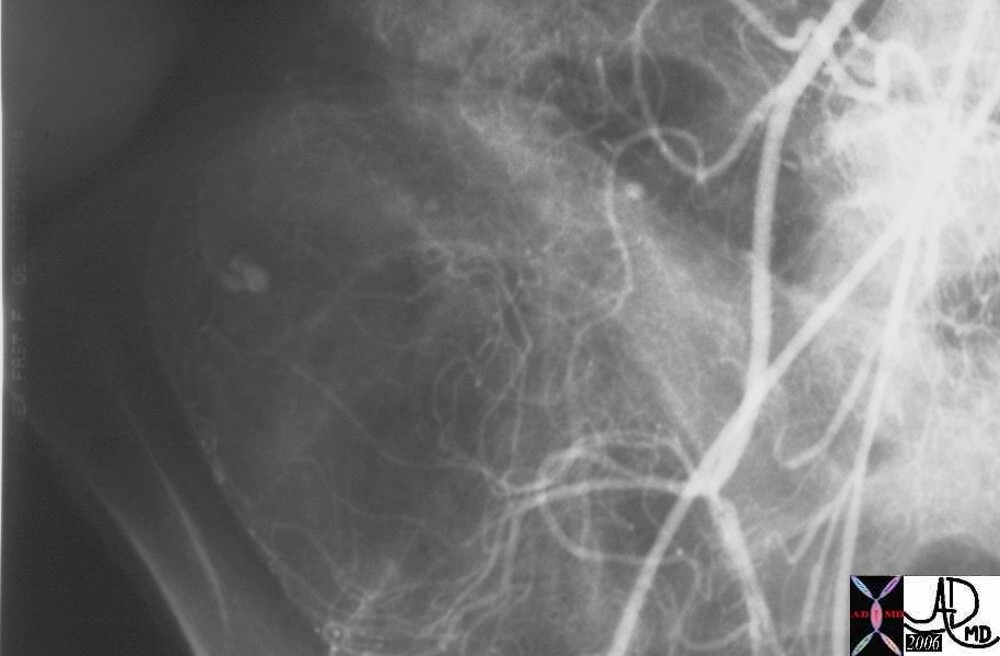  
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage |
| Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia |
RS
Acute

Acute Pneumonitis Secondary to Chemotherapy ? Drug Reaction |
| 47095 lung chest fx lobar infiltrates fx air bronchogram dx chemotherapy related pneumonitis acute inflammation CTscan Davidoff MD |
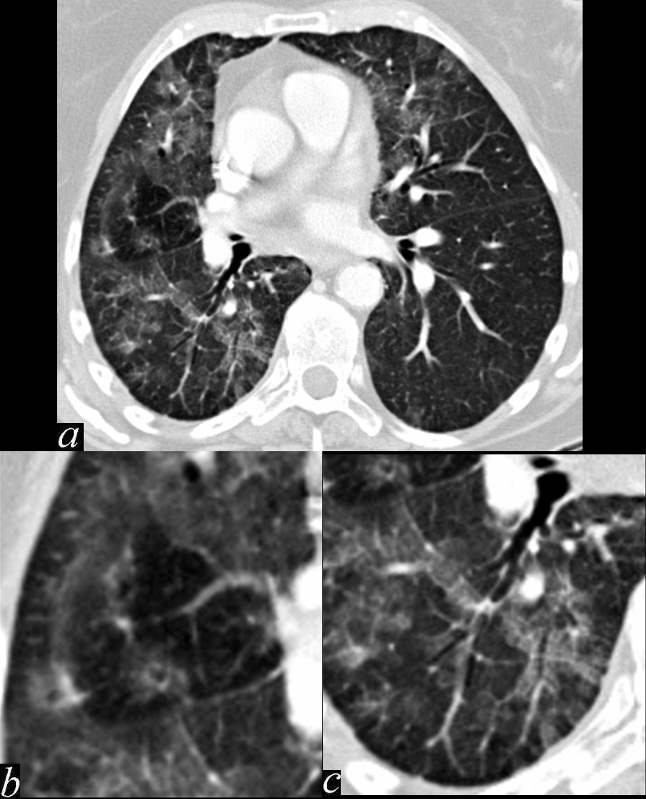 
Bronchovascular Inflammation |
| 47170c01.800 bronchocentric inflammation lung bronchovascular bundle chest inflammation peribronchial halo air trapping mosaic perfusion ground glass changes alveolar change air bronchogram acute bronchovascular inflammation ddx allergic collagen vascular disease infection CTscan |
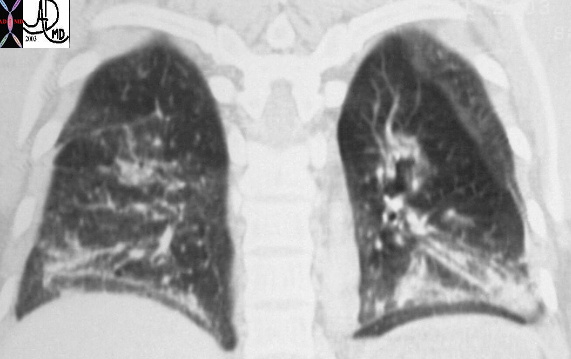
Scleroderma |
| This coronally reformatted CT of the posterior aspect of the chest shows interstitial lung disease within the lower lobes in this patient with scleroderma. The upper lobes were relatively spared. Courtesy Ashley Davidoff MD. 30476 code lung pulmonary interstitium interstial disease thickening lower lobes chronic inflammation fibrosis scleroderma collagen vascular disease imaging radiology CTscan |
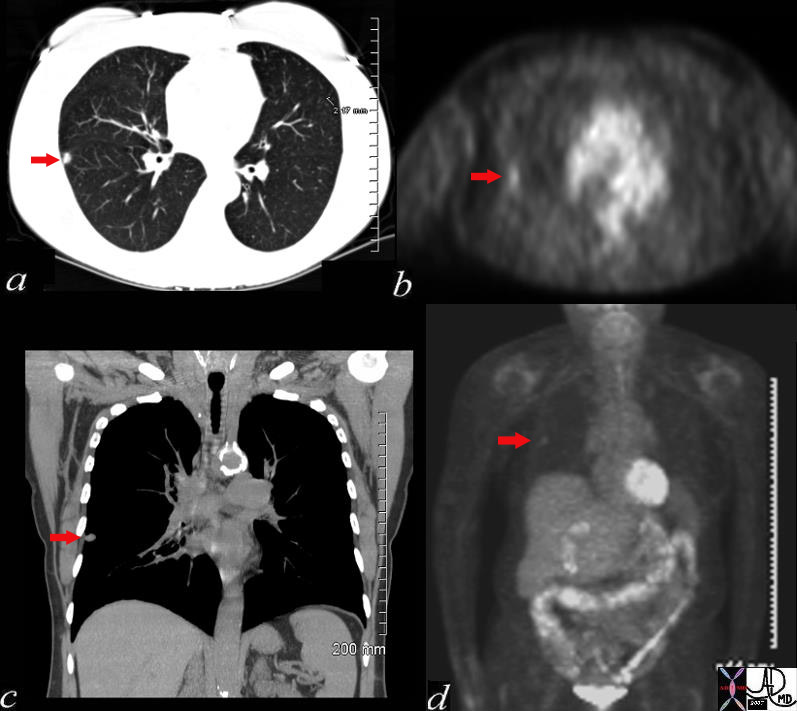 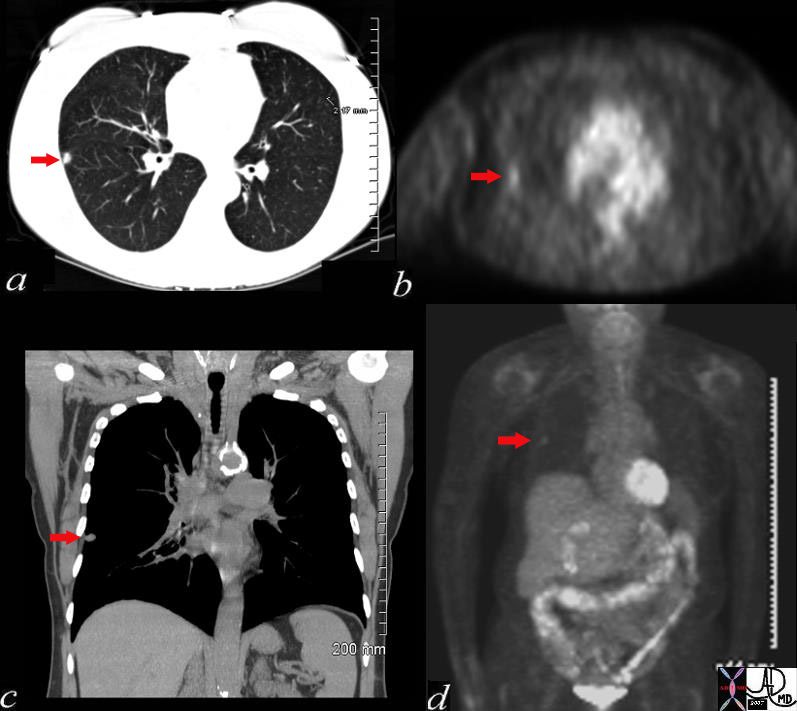
Necrotizing Granuloma |
| 72372c03 60 female with long history of smoking lung nodule slow growth SUV 1.3 right lower lobe dx necrotizing granuloma Most necrotizing granulomas are related to infection. Wegener?s granulomatosis Churg-Strauss syndrome ? vasculitis sarcoidosis usually non necrotizing CTscan PETscan Davidoff MD |
Subacute Inflammation
Chronic Inflammation
Environmental Causes of Chronic Inflammation
  Asbestosis Asbestosis |
| 47060c01 chest lung fx shaggy heart border reticular changes interstitial lung disease interstitium honeycombing pleural calcification fibrosis dx asbestosis CTscan Davidoff MD |
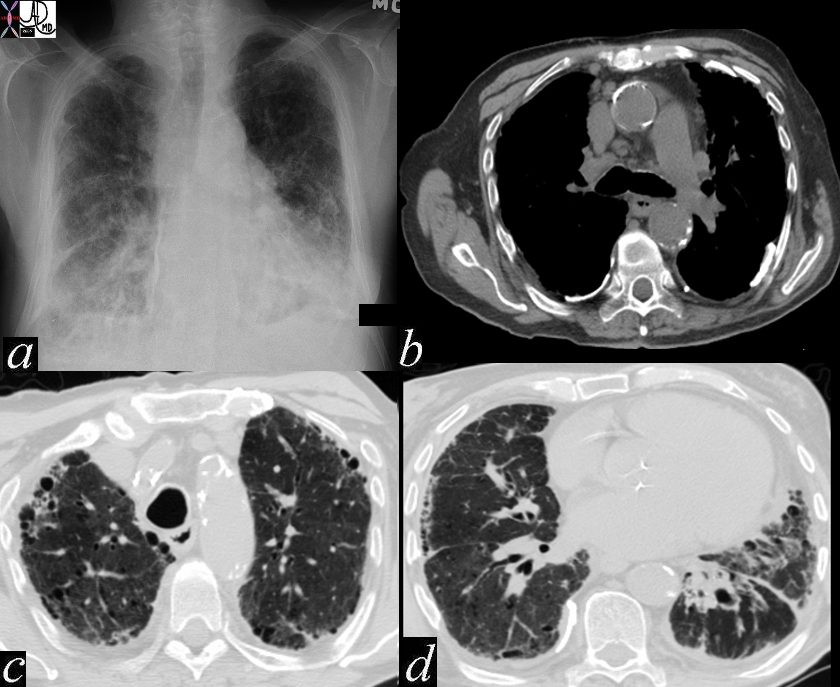
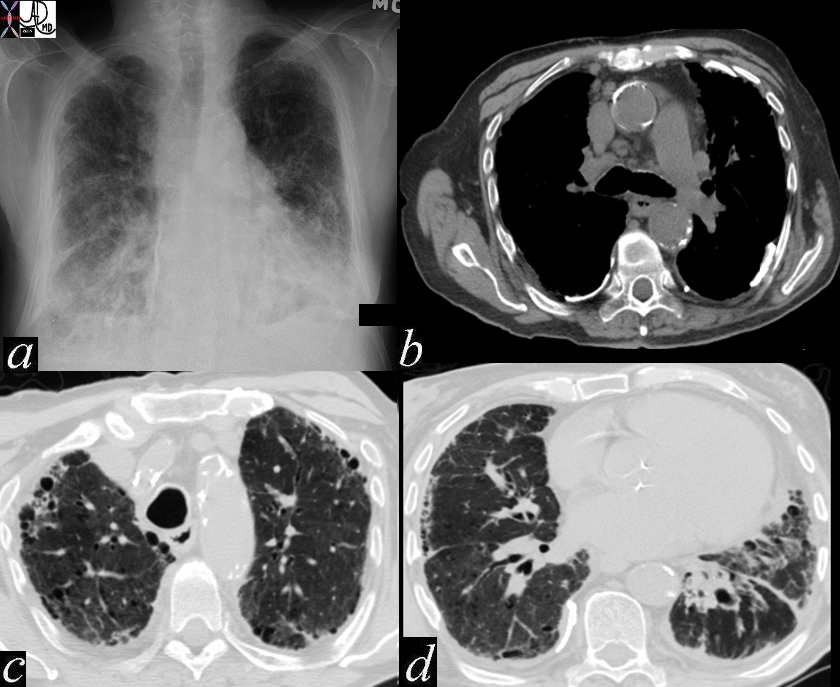
 End Stage Fibrosis ? IPF End Stage Fibrosis ? IPF |
| 47145c01 lung interstitium interstitial disease parenchymal destruction shaggy heart border fx honeycombing interstitial pulmonary fibrosis IPF CTscan Davidoff MD |
GIT
 
Normal GE Junction and Ulcerating Esophagitis |
| 02464b Normal Davidoff MD01239 Ashley Davidoff MD code esophagus ulcer ulcerating inflammed inflammation red congested esophagitis grosspathology |
 
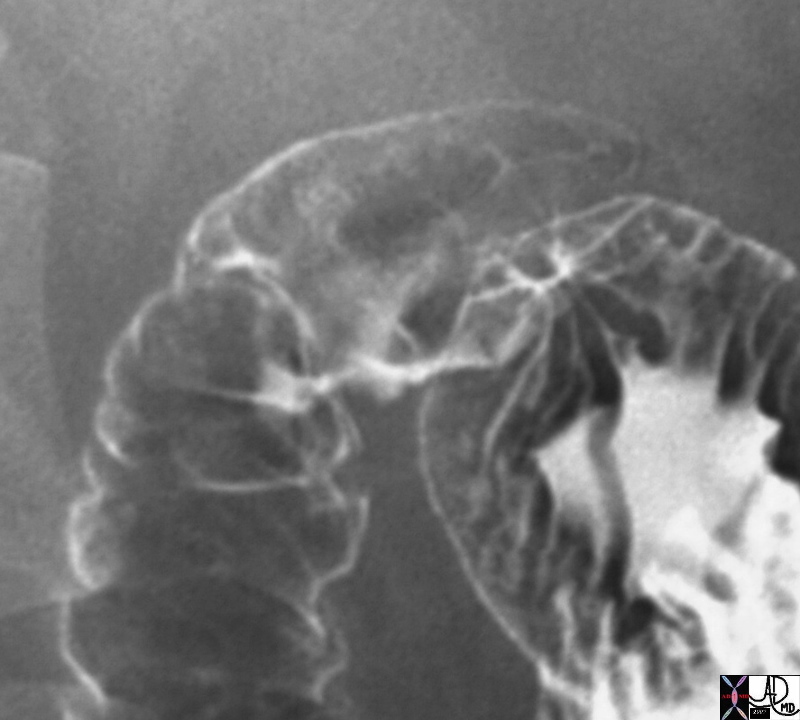
Normal and Quinidine Ulcer |
| 39562b01 esophagus single contrast barium wallow normal anatomy Davidoff MDCourtesy Ashley Davidoff MD 01258 esophagus + quinidine ulcer barium swallow inflammation upper GI UGI imaging radiology contrast X-Ray |
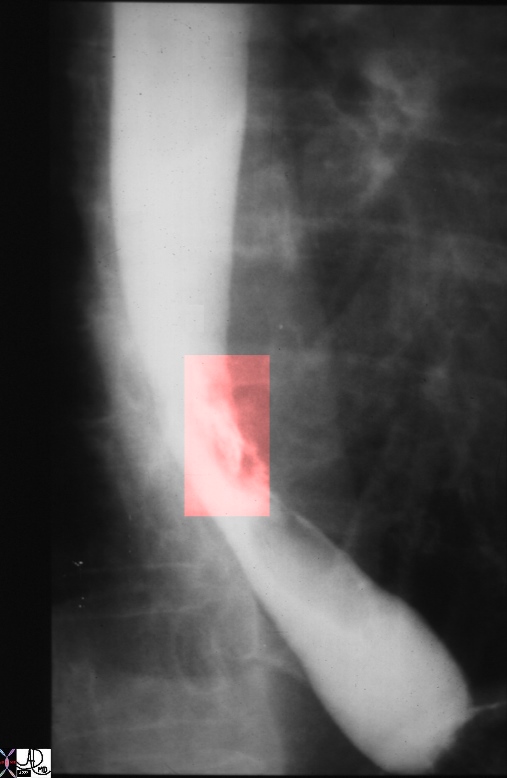
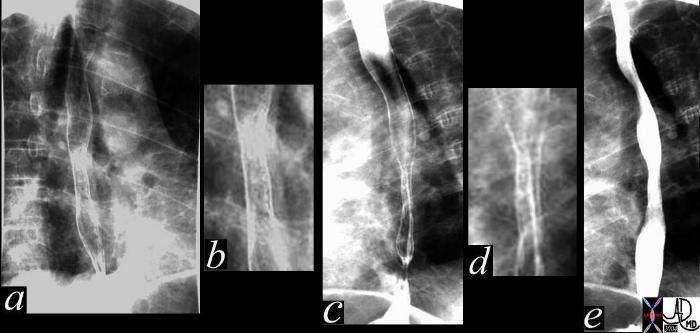
Radiation Induced Esophagitis ? Fixed Narrowing |
| This series of esphageal images from a double contrast barium swallow shows a long segment stenosis in mid esophagus assocated with punctate accumulations of contrast. The patient is known to have lung carcinoma and hasirradiation and the findings are consistent with radiation esophagitis. Courtesy Ashley Davidoff MD 38394c code GI esophagus radiation esophagitis ulceration |
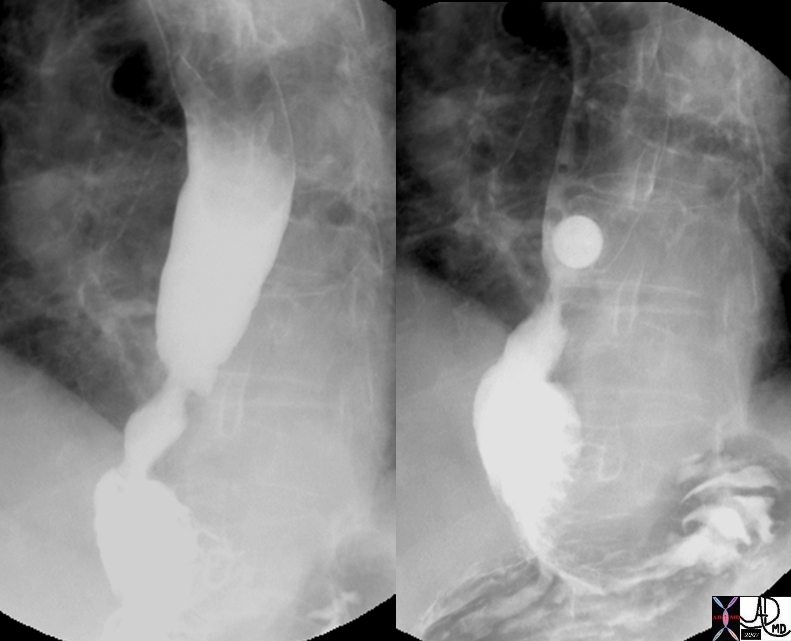 13 mm stricture in Esophagus 13 mm stricture in Esophagus |
| 49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD |
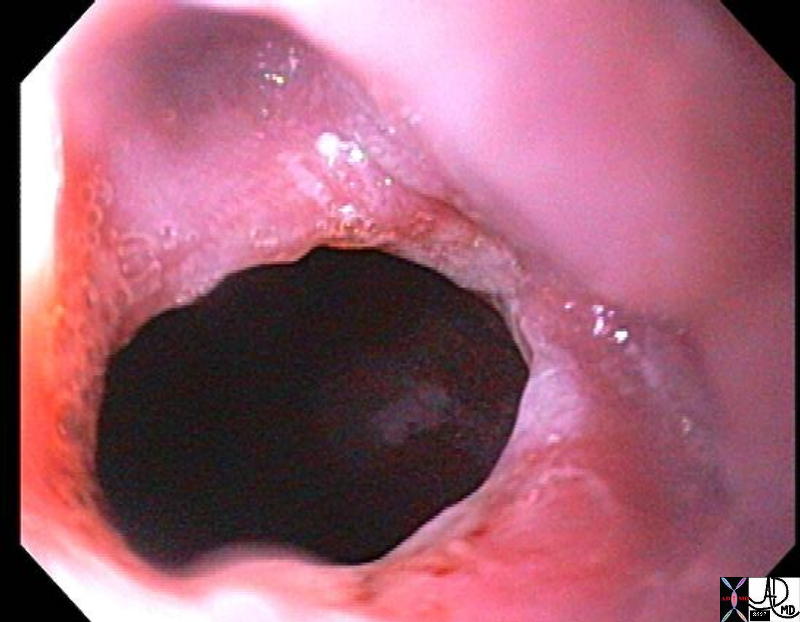 
Stricture of the Esophagus |
| 73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias |
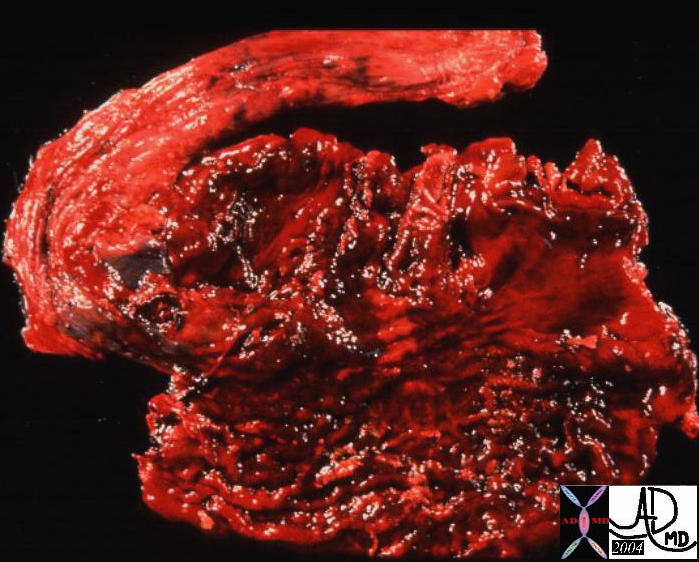 
Normal Antrum and Stomach with Hemorrhagic Gastritis |
| 01978b stomach gastric pylorus duodenum junction normal anatomy12263 code stomach gastric + hemorrhagic gastritis grosspathology |
Hemorrhagic Gastritis |
| 12264 code stomach gastric + hemorrhagic gastritis grosspathology |
  
Linear Erosions of Antral Gastritis |
| 49746b01 normal01323 01323b01 code stomach + linear erosions erosive gastritis + upper GI UGI imaging radiology contrast X-Ray inflammation |
|
Normal Antrum, Pylorus and Duodenum |
| 01978b stomach gastric pylorus duodenum junction normal anatomy |
Normal Bulb and Crohn?s Duodenitis |
|
33637b02 normal
01954 duodenum fx thickened folds dx duodenitis Crohn?s disease upper GI UGI imaging radiology contrast X-Ray Courtesy Ashley Davidoff MD DB |
 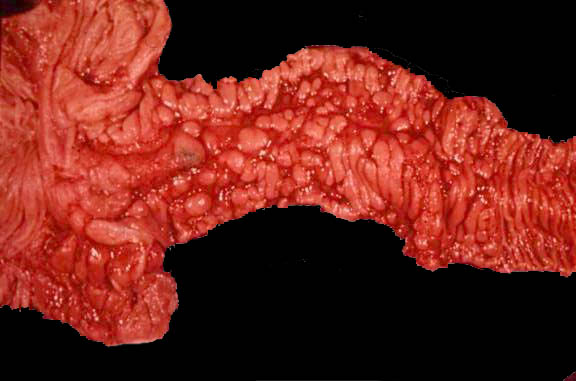
Normal and Denuded Ulcerating Mucosa with Cobblestone of the Terminal Ileum in Crohn?s Disease |
| 12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB |
  
Normal and Cobblestone |
| 32525b01 small bowel terminal ileum colon ileocecal valve large bowel normal anatomy UGI SBFT Courtesy Ashley Davidoff MD
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD |
|
Cobblestone of the Terminal Ileum |
|
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD 02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB |

Terminal Normal terminal Ileum and Ileum Chronic Inflammation with Secondary Narrowing |
| Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD 12287 l |
|
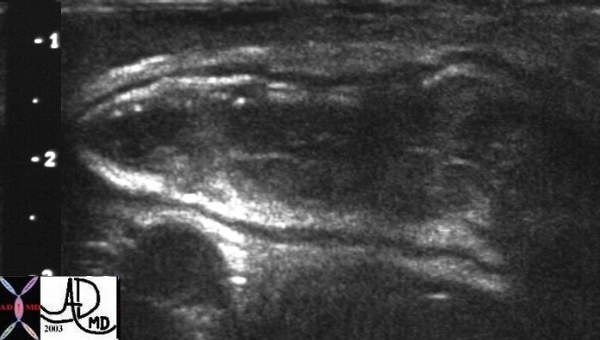
Ileum Chronic Inflammation with Secondary Narrowing and USscan of the Terminal ileum |
| Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD
12287 l |

Stenoses in Bile Ducts Caused by Sclerosing Cholangitis |
| 24209.800 76 male with jaundice liver bile duct fx narrowed fx multicentric narrowing Dx sclerosing cholangitis chronic inflammation pancreas pancreatic duct ampulla fx normal MRI T2 weighted Davidoff MD |

Cholecysto-duodenal Fistula |
| 26909c04.8s gallbladder air stomach duodenum thickened dx penetrating ulcer dx cholecystoduodenal fistula IVC inferior vena cava filteer small prominent folds valvulae conniventes ascites CTscan C+ Courtesy Ashley Davidoff MD copyright 2008 |
|
Before and After Acute Pncreatitis Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid |
| 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02 |
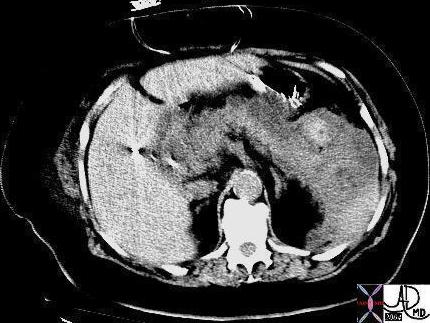
Hemorrhagic Pancreatitis |
| 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation |
Skin
  Laceration Laceration |
| 82875.800 trauma hand knuckle carpal bones skin abrasion blood coagulation redness inflammation vein Davidoff MD Davidoff photography |
Types
Hemorrhagic Inflammation
|
Hemorrhagic Pancreatitis |
| 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation |
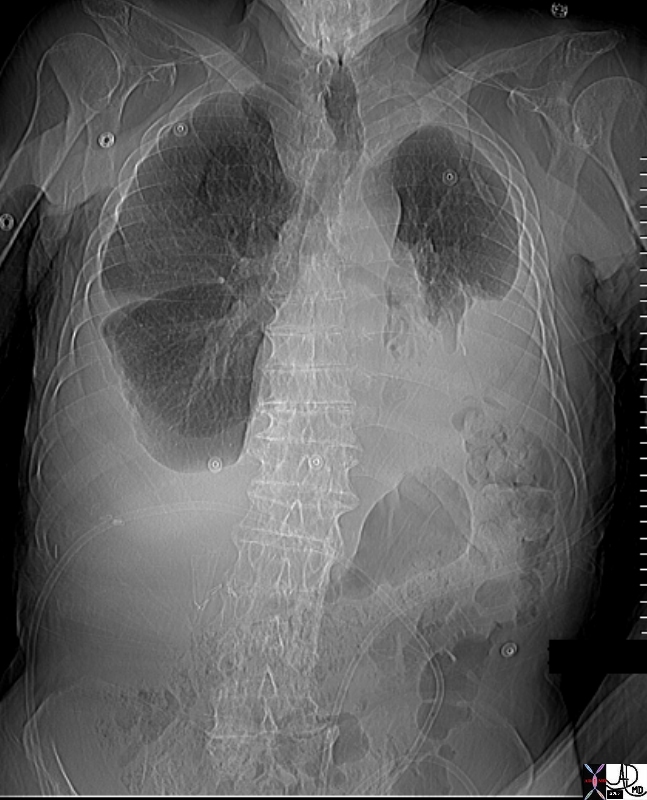    
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification |
| 74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD |
Metaplasia ? Sign of Chronic Inflammation |
| This medium power photomicrograph shows gallbladder mucosa with an inflammatory infiltrate of mononuclear cells. The lumen is the clear area, and a tiny part of muscular layer can be seen at the opposite side of the picture. Look carefully and you will find one area near the lumen with goblet cells, like intestinal epithelium. This is intestinal metaplasia. Deeper in the mucosa near the muscular layer is a cluster of a few glands which do not have a tall columnar epithelium. They resemble gastric glands, and in fact this is gastric metaplasia. Metaplastic epithelium occurs frequently throughout the biliary and gastrointestinal tracts in chronic inflammatory conditions. In the gallbladder it has no significance other than being part of the changes due to chronic inflammation.11932.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD |
Chronic
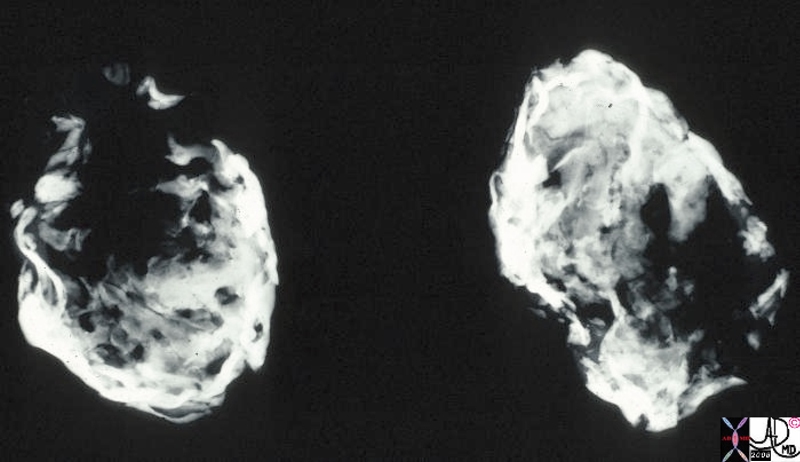
Porcelain Gallbladder ? Variant of Chronic Inflammation |
| This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma.11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD |
Porcelain Gallbladder ? Variant of Chronic Inflammation |
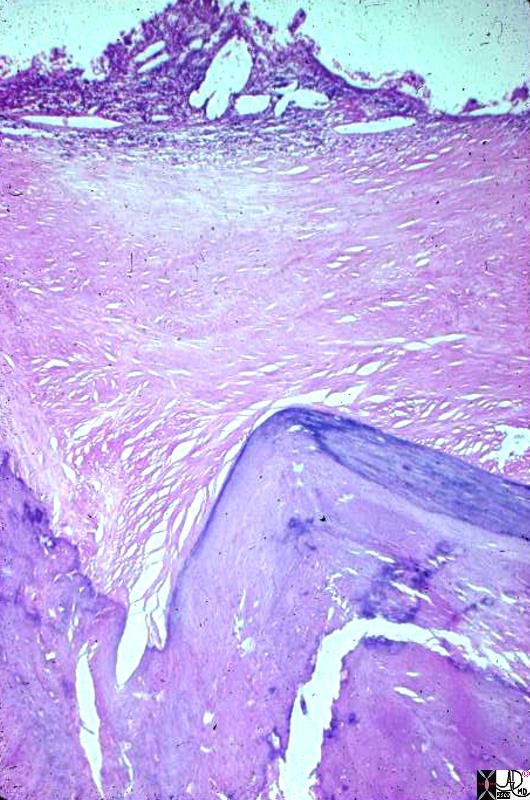
| This photomicrograph at low power shows most of the full thickness of the wall of a gallbladder. The lumen is the clear area at one side of the picture. The pale homogeneous area down the middle is fibrous replacement of the wall. The little nubbin of tissue and cholesterol clefts along the lumen represents what is left of the mucosa. The darker, zig-zag structure at the side opposite the lumen represents where the gallbladder wall is calcified. This calcification and fibrosis of the entire gallbladder wall is the diagnostic feature of porcelain gallbladder.11940.8s gallbladder porcelain gallbladder histopathology Courtesy Barbara Banner MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
This photomicrograph at low power shows most of the full thickness of the wall of a gallbladder. The lumen is the clear area at one side of the picture. The pale homogeneous area down the middle is fibrous replacement of the wall. The little nubbin of tissue and cholesterol clefts along the lumen represents what is left of the mucosa. The darker, zig-zag structure at the side opposite the lumen represents where the gallbladder wall is calcified. This calcification and fibrosis of the entire gallbladder wall is the diagnostic feature of porcelain gallbladder.11940.8s gallbladder porcelain gallbladder histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
This photomicrograph at low power shows most of the full thickness of the wall of a gallbladder. The lumen is the clear area at one side of the picture. The pale homogeneous area down the middle is fibrous replacement of the wall. The little nubbin of tissue and cholesterol clefts along the lumen represents what is left of the mucosa. The darker, zig-zag structure at the side opposite the lumen represents where the gallbladder wall is calcified. This calcification and fibrosis of the entire gallbladder wall is the diagnostic feature of porcelain gallbladder.11940.8s gallbladder porcelain gallbladder histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This photomicrograph at low power shows most of the full thickness of the wall of a gallbladder. The lumen is the clear area at one side of the picture. The pale homogeneous area down the middle is fibrous replacement of the wall. The little nubbin of tissue and cholesterol clefts along the lumen represents what is left of the mucosa. The darker, zig-zag structure at the side opposite the lumen represents where the gallbladder wall is calcified. This calcification and fibrosis of the entire gallbladder wall is the diagnostic feature of porcelain gallbladder.11940.8s gallbladder porcelain gallbladder histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This photomicrograph at low power shows most of the full thickness of the wall of a gallbladder. The lumen is the clear area at one side of the picture. The pale homogeneous area down the middle is fibrous replacement of the wall. The little nubbin of tissue and cholesterol clefts along the lumen represents what is left of the mucosa. The darker, zig-zag structure at the side opposite the lumen represents where the gallbladder wall is calcified. This calcification and fibrosis of the entire gallbladder wall is the diagnostic feature of porcelain gallbladder.11940.8s gallbladder porcelain gallbladder histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma.11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma.11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma.11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma.11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Porcelain Gallbladder ? Variant of Chronic Inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Metaplasia ? Sign of Chronic Inflammation
This medium power photomicrograph shows gallbladder mucosa with an inflammatory infiltrate of mononuclear cells. The lumen is the clear area, and a tiny part of muscular layer can be seen at the opposite side of the picture. Look carefully and you will find one area near the lumen with goblet cells, like intestinal epithelium. This is intestinal metaplasia. Deeper in the mucosa near the muscular layer is a cluster of a few glands which do not have a tall columnar epithelium. They resemble gastric glands, and in fact this is gastric metaplasia. Metaplastic epithelium occurs frequently throughout the biliary and gastrointestinal tracts in chronic inflammatory conditions. In the gallbladder it has no significance other than being part of the changes due to chronic inflammation.11932.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Metaplasia ? Sign of Chronic Inflammation
This medium power photomicrograph shows gallbladder mucosa with an inflammatory infiltrate of mononuclear cells. The lumen is the clear area, and a tiny part of muscular layer can be seen at the opposite side of the picture. Look carefully and you will find one area near the lumen with goblet cells, like intestinal epithelium. This is intestinal metaplasia. Deeper in the mucosa near the muscular layer is a cluster of a few glands which do not have a tall columnar epithelium. They resemble gastric glands, and in fact this is gastric metaplasia. Metaplastic epithelium occurs frequently throughout the biliary and gastrointestinal tracts in chronic inflammatory conditions. In the gallbladder it has no significance other than being part of the changes due to chronic inflammation.11932.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This medium power photomicrograph shows gallbladder mucosa with an inflammatory infiltrate of mononuclear cells. The lumen is the clear area, and a tiny part of muscular layer can be seen at the opposite side of the picture. Look carefully and you will find one area near the lumen with goblet cells, like intestinal epithelium. This is intestinal metaplasia. Deeper in the mucosa near the muscular layer is a cluster of a few glands which do not have a tall columnar epithelium. They resemble gastric glands, and in fact this is gastric metaplasia. Metaplastic epithelium occurs frequently throughout the biliary and gastrointestinal tracts in chronic inflammatory conditions. In the gallbladder it has no significance other than being part of the changes due to chronic inflammation.11932.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This medium power photomicrograph shows gallbladder mucosa with an inflammatory infiltrate of mononuclear cells. The lumen is the clear area, and a tiny part of muscular layer can be seen at the opposite side of the picture. Look carefully and you will find one area near the lumen with goblet cells, like intestinal epithelium. This is intestinal metaplasia. Deeper in the mucosa near the muscular layer is a cluster of a few glands which do not have a tall columnar epithelium. They resemble gastric glands, and in fact this is gastric metaplasia. Metaplastic epithelium occurs frequently throughout the biliary and gastrointestinal tracts in chronic inflammatory conditions. In the gallbladder it has no significance other than being part of the changes due to chronic inflammation.11932.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Metaplasia ? Sign of Chronic Inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Metaplasia ? Sign of Chronic Inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification
74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification
74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hemorrhagic Pancreatitis
16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hemorrhagic Pancreatitis
16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hemorrhagic Pancreatitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hemorrhagic Pancreatitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Laceration
82875.800 trauma hand knuckle carpal bones skin abrasion blood coagulation redness inflammation vein Davidoff MD Davidoff photography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Laceration
82875.800 trauma hand knuckle carpal bones skin abrasion blood coagulation redness inflammation vein Davidoff MD Davidoff photography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 82875.800 trauma hand knuckle carpal bones skin abrasion blood coagulation redness inflammation vein Davidoff MD Davidoff photography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82875.800 trauma hand knuckle carpal bones skin abrasion blood coagulation redness inflammation vein Davidoff MD Davidoff photography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Laceration
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Laceration
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hemorrhagic Pancreatitis
16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hemorrhagic Pancreatitis
16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 16851b04 Courtesy Ashley Davidoff MD code pancreas + fx mass hemorrhage acute pancreatitis acute hemorrhagic pancreatitis imaging radiology CTscan inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hemorrhagic Pancreatitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hemorrhagic Pancreatitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cholecysto-duodenal Fistula
26909c04.8s gallbladder air stomach duodenum thickened dx penetrating ulcer dx cholecystoduodenal fistula IVC inferior vena cava filteer small prominent folds valvulae conniventes ascites CTscan C+ Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cholecysto-duodenal Fistula
26909c04.8s gallbladder air stomach duodenum thickened dx penetrating ulcer dx cholecystoduodenal fistula IVC inferior vena cava filteer small prominent folds valvulae conniventes ascites CTscan C+ Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 26909c04.8s gallbladder air stomach duodenum thickened dx penetrating ulcer dx cholecystoduodenal fistula IVC inferior vena cava filteer small prominent folds valvulae conniventes ascites CTscan C+ Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 26909c04.8s gallbladder air stomach duodenum thickened dx penetrating ulcer dx cholecystoduodenal fistula IVC inferior vena cava filteer small prominent folds valvulae conniventes ascites CTscan C+ Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cholecysto-duodenal Fistula
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cholecysto-duodenal Fistula
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Stenoses in Bile Ducts Caused by Sclerosing Cholangitis
24209.800 76 male with jaundice liver bile duct fx narrowed fx multicentric narrowing Dx sclerosing cholangitis chronic inflammation pancreas pancreatic duct ampulla fx normal MRI T2 weighted Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Stenoses in Bile Ducts Caused by Sclerosing Cholangitis
24209.800 76 male with jaundice liver bile duct fx narrowed fx multicentric narrowing Dx sclerosing cholangitis chronic inflammation pancreas pancreatic duct ampulla fx normal MRI T2 weighted Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 24209.800 76 male with jaundice liver bile duct fx narrowed fx multicentric narrowing Dx sclerosing cholangitis chronic inflammation pancreas pancreatic duct ampulla fx normal MRI T2 weighted Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 24209.800 76 male with jaundice liver bile duct fx narrowed fx multicentric narrowing Dx sclerosing cholangitis chronic inflammation pancreas pancreatic duct ampulla fx normal MRI T2 weighted Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Stenoses in Bile Ducts Caused by Sclerosing Cholangitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Stenoses in Bile Ducts Caused by Sclerosing Cholangitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ileum Chronic Inflammation with Secondary Narrowing and USscan of the Terminal ileum
Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD
12287 l
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ileum Chronic Inflammation with Secondary Narrowing and USscan of the Terminal ileum
Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD
12287 l
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD
12287 l
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD
12287 l
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Ileum Chronic Inflammation with Secondary Narrowing and USscan of the Terminal ileum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Ileum Chronic Inflammation with Secondary Narrowing and USscan of the Terminal ileum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Terminal Normal terminal Ileum and Ileum Chronic Inflammation with Secondary Narrowing
Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD 12287 l
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Terminal Normal terminal Ileum and Ileum Chronic Inflammation with Secondary Narrowing
Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD 12287 l
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD 12287 l
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Gross photomicrograph of a terminal ileum from a patient with Crohn?s disease. Notice the stricture which tapers to a maximum at the ileocecal valve. Notice also the irregular linear longitudinal ulcers with tufts of remaining mucosa between them. Notice the sharp segmental cutoff to more normal-appearing ileum as you move away from the ileocecal valve. Notice that the bowel wall in the involved area is thickened. code small bowel ileum fx thickening fx linear ulcers dx Crohns disease Crohn?s disease grosspathology Courtesy Barbara Banner MD12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD 12287 l
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Terminal Normal terminal Ileum and Ileum Chronic Inflammation with Secondary Narrowing
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Terminal Normal terminal Ileum and Ileum Chronic Inflammation with Secondary Narrowing
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cobblestone of the Terminal Ileum
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cobblestone of the Terminal Ileum
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cobblestone of the Terminal Ileum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cobblestone of the Terminal Ileum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal and Cobblestone
32525b01 small bowel terminal ileum colon ileocecal valve large bowel normal anatomy UGI SBFT Courtesy Ashley Davidoff MD
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Cobblestone
32525b01 small bowel terminal ileum colon ileocecal valve large bowel normal anatomy UGI SBFT Courtesy Ashley Davidoff MD
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32525b01 small bowel terminal ileum colon ileocecal valve large bowel normal anatomy UGI SBFT Courtesy Ashley Davidoff MD
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32525b01 small bowel terminal ileum colon ileocecal valve large bowel normal anatomy UGI SBFT Courtesy Ashley Davidoff MD
43159 small bowel fx ileum fx nodular mucosa fx cobblestone fx thickened folds fx narrowed lumen dx Crohns UGI SBFT Courtesy Ashley Davidoff MD AFD AFD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Cobblestone
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Cobblestone
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal and Denuded Ulcerating Mucosa with Cobblestone of the Terminal Ileum in Crohn?s Disease
12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Denuded Ulcerating Mucosa with Cobblestone of the Terminal Ileum in Crohn?s Disease
12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 12231 colon large bowel cecum ileocecal valve appendix fx normal anatomy Courtesy Barbara Banner MD02477b02 small bowel terminal ileum mucosa fx inflammation ulceration fx nodules fx cobble stone thick walled dx Crohn?s disease ileocecal valve grosspathology Courtesy Dr Gutkin MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Denuded Ulcerating Mucosa with Cobblestone of the Terminal Ileum in Crohn?s Disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Denuded Ulcerating Mucosa with Cobblestone of the Terminal Ileum in Crohn?s Disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Bulb and Crohn?s Duodenitis
33637b02 normal
01954 duodenum fx thickened folds dx duodenitis Crohn?s disease upper GI UGI imaging radiology contrast X-Ray Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Bulb and Crohn?s Duodenitis
33637b02 normal
01954 duodenum fx thickened folds dx duodenitis Crohn?s disease upper GI UGI imaging radiology contrast X-Ray Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
33637b02 normal
01954 duodenum fx thickened folds dx duodenitis Crohn?s disease upper GI UGI imaging radiology contrast X-Ray Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
33637b02 normal
01954 duodenum fx thickened folds dx duodenitis Crohn?s disease upper GI UGI imaging radiology contrast X-Ray Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Bulb and Crohn?s Duodenitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Bulb and Crohn?s Duodenitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Antrum, Pylorus and Duodenum
01978b stomach gastric pylorus duodenum junction normal anatomy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Antrum, Pylorus and Duodenum
01978b stomach gastric pylorus duodenum junction normal anatomy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 01978b stomach gastric pylorus duodenum junction normal anatomy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 01978b stomach gastric pylorus duodenum junction normal anatomy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Antrum, Pylorus and Duodenum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Antrum, Pylorus and Duodenum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Linear Erosions of Antral Gastritis
49746b01 normal01323 01323b01 code stomach + linear erosions erosive gastritis + upper GI UGI imaging radiology contrast X-Ray inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Linear Erosions of Antral Gastritis
49746b01 normal01323 01323b01 code stomach + linear erosions erosive gastritis + upper GI UGI imaging radiology contrast X-Ray inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49746b01 normal01323 01323b01 code stomach + linear erosions erosive gastritis + upper GI UGI imaging radiology contrast X-Ray inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49746b01 normal01323 01323b01 code stomach + linear erosions erosive gastritis + upper GI UGI imaging radiology contrast X-Ray inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Linear Erosions of Antral Gastritis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Linear Erosions of Antral Gastritis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hemorrhagic Gastritis
12264 code stomach gastric + hemorrhagic gastritis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hemorrhagic Gastritis
12264 code stomach gastric + hemorrhagic gastritis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 12264 code stomach gastric + hemorrhagic gastritis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 12264 code stomach gastric + hemorrhagic gastritis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hemorrhagic Gastritis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hemorrhagic Gastritis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Antrum and Stomach with Hemorrhagic Gastritis
01978b stomach gastric pylorus duodenum junction normal anatomy12263 code stomach gastric + hemorrhagic gastritis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Antrum and Stomach with Hemorrhagic Gastritis
01978b stomach gastric pylorus duodenum junction normal anatomy12263 code stomach gastric + hemorrhagic gastritis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 01978b stomach gastric pylorus duodenum junction normal anatomy12263 code stomach gastric + hemorrhagic gastritis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 01978b stomach gastric pylorus duodenum junction normal anatomy12263 code stomach gastric + hemorrhagic gastritis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Antrum and Stomach with Hemorrhagic Gastritis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Antrum and Stomach with Hemorrhagic Gastritis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Stricture of the Esophagus
73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Stricture of the Esophagus
73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Stricture of the Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Stricture of the Esophagus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
13 mm stricture in Esophagus
49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
13 mm stricture in Esophagus
49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 13 mm stricture in Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 13 mm stricture in Esophagus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Radiation Induced Esophagitis ? Fixed Narrowing
This series of esphageal images from a double contrast barium swallow shows a long segment stenosis in mid esophagus assocated with punctate accumulations of contrast. The patient is known to have lung carcinoma and hasirradiation and the findings are consistent with radiation esophagitis. Courtesy Ashley Davidoff MD 38394c code GI esophagus radiation esophagitis ulceration
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Radiation Induced Esophagitis ? Fixed Narrowing
This series of esphageal images from a double contrast barium swallow shows a long segment stenosis in mid esophagus assocated with punctate accumulations of contrast. The patient is known to have lung carcinoma and hasirradiation and the findings are consistent with radiation esophagitis. Courtesy Ashley Davidoff MD 38394c code GI esophagus radiation esophagitis ulceration
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This series of esphageal images from a double contrast barium swallow shows a long segment stenosis in mid esophagus assocated with punctate accumulations of contrast. The patient is known to have lung carcinoma and hasirradiation and the findings are consistent with radiation esophagitis. Courtesy Ashley Davidoff MD 38394c code GI esophagus radiation esophagitis ulceration
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This series of esphageal images from a double contrast barium swallow shows a long segment stenosis in mid esophagus assocated with punctate accumulations of contrast. The patient is known to have lung carcinoma and hasirradiation and the findings are consistent with radiation esophagitis. Courtesy Ashley Davidoff MD 38394c code GI esophagus radiation esophagitis ulceration
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Radiation Induced Esophagitis ? Fixed Narrowing
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Radiation Induced Esophagitis ? Fixed Narrowing
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal and Quinidine Ulcer
39562b01 esophagus single contrast barium wallow normal anatomy Davidoff MDCourtesy Ashley Davidoff MD 01258 esophagus + quinidine ulcer barium swallow inflammation upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Quinidine Ulcer
39562b01 esophagus single contrast barium wallow normal anatomy Davidoff MDCourtesy Ashley Davidoff MD 01258 esophagus + quinidine ulcer barium swallow inflammation upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 39562b01 esophagus single contrast barium wallow normal anatomy Davidoff MDCourtesy Ashley Davidoff MD 01258 esophagus + quinidine ulcer barium swallow inflammation upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 39562b01 esophagus single contrast barium wallow normal anatomy Davidoff MDCourtesy Ashley Davidoff MD 01258 esophagus + quinidine ulcer barium swallow inflammation upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Quinidine Ulcer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Quinidine Ulcer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal GE Junction and Ulcerating Esophagitis
02464b Normal Davidoff MD01239 Ashley Davidoff MD code esophagus ulcer ulcerating inflammed inflammation red congested esophagitis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal GE Junction and Ulcerating Esophagitis
02464b Normal Davidoff MD01239 Ashley Davidoff MD code esophagus ulcer ulcerating inflammed inflammation red congested esophagitis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 02464b Normal Davidoff MD01239 Ashley Davidoff MD code esophagus ulcer ulcerating inflammed inflammation red congested esophagitis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 02464b Normal Davidoff MD01239 Ashley Davidoff MD code esophagus ulcer ulcerating inflammed inflammation red congested esophagitis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal GE Junction and Ulcerating Esophagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal GE Junction and Ulcerating Esophagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
End Stage Fibrosis ? IPF
47145c01 lung interstitium interstitial disease parenchymal destruction shaggy heart border fx honeycombing interstitial pulmonary fibrosis IPF CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
End Stage Fibrosis ? IPF
47145c01 lung interstitium interstitial disease parenchymal destruction shaggy heart border fx honeycombing interstitial pulmonary fibrosis IPF CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47145c01 lung interstitium interstitial disease parenchymal destruction shaggy heart border fx honeycombing interstitial pulmonary fibrosis IPF CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47145c01 lung interstitium interstitial disease parenchymal destruction shaggy heart border fx honeycombing interstitial pulmonary fibrosis IPF CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => End Stage Fibrosis ? IPF
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => End Stage Fibrosis ? IPF
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Asbestosis
47060c01 chest lung fx shaggy heart border reticular changes interstitial lung disease interstitium honeycombing pleural calcification fibrosis dx asbestosis CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Asbestosis
47060c01 chest lung fx shaggy heart border reticular changes interstitial lung disease interstitium honeycombing pleural calcification fibrosis dx asbestosis CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47060c01 chest lung fx shaggy heart border reticular changes interstitial lung disease interstitium honeycombing pleural calcification fibrosis dx asbestosis CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47060c01 chest lung fx shaggy heart border reticular changes interstitial lung disease interstitium honeycombing pleural calcification fibrosis dx asbestosis CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Asbestosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Asbestosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Necrotizing Granuloma
72372c03 60 female with long history of smoking lung nodule slow growth SUV 1.3 right lower lobe dx necrotizing granuloma Most necrotizing granulomas are related to infection. Wegener?s granulomatosis Churg-Strauss syndrome ? vasculitis sarcoidosis usually non necrotizing CTscan PETscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Necrotizing Granuloma
72372c03 60 female with long history of smoking lung nodule slow growth SUV 1.3 right lower lobe dx necrotizing granuloma Most necrotizing granulomas are related to infection. Wegener?s granulomatosis Churg-Strauss syndrome ? vasculitis sarcoidosis usually non necrotizing CTscan PETscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 72372c03 60 female with long history of smoking lung nodule slow growth SUV 1.3 right lower lobe dx necrotizing granuloma Most necrotizing granulomas are related to infection. Wegener?s granulomatosis Churg-Strauss syndrome ? vasculitis sarcoidosis usually non necrotizing CTscan PETscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72372c03 60 female with long history of smoking lung nodule slow growth SUV 1.3 right lower lobe dx necrotizing granuloma Most necrotizing granulomas are related to infection. Wegener?s granulomatosis Churg-Strauss syndrome ? vasculitis sarcoidosis usually non necrotizing CTscan PETscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Necrotizing Granuloma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Necrotizing Granuloma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Scleroderma
This coronally reformatted CT of the posterior aspect of the chest shows interstitial lung disease within the lower lobes in this patient with scleroderma. The upper lobes were relatively spared. Courtesy Ashley Davidoff MD. 30476 code lung pulmonary interstitium interstial disease thickening lower lobes chronic inflammation fibrosis scleroderma collagen vascular disease imaging radiology CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma
This coronally reformatted CT of the posterior aspect of the chest shows interstitial lung disease within the lower lobes in this patient with scleroderma. The upper lobes were relatively spared. Courtesy Ashley Davidoff MD. 30476 code lung pulmonary interstitium interstial disease thickening lower lobes chronic inflammation fibrosis scleroderma collagen vascular disease imaging radiology CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This coronally reformatted CT of the posterior aspect of the chest shows interstitial lung disease within the lower lobes in this patient with scleroderma. The upper lobes were relatively spared. Courtesy Ashley Davidoff MD. 30476 code lung pulmonary interstitium interstial disease thickening lower lobes chronic inflammation fibrosis scleroderma collagen vascular disease imaging radiology CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This coronally reformatted CT of the posterior aspect of the chest shows interstitial lung disease within the lower lobes in this patient with scleroderma. The upper lobes were relatively spared. Courtesy Ashley Davidoff MD. 30476 code lung pulmonary interstitium interstial disease thickening lower lobes chronic inflammation fibrosis scleroderma collagen vascular disease imaging radiology CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Bronchovascular Inflammation
47170c01.800 bronchocentric inflammation lung bronchovascular bundle chest inflammation peribronchial halo air trapping mosaic perfusion ground glass changes alveolar change air bronchogram acute bronchovascular inflammation ddx allergic collagen vascular disease infection CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Bronchovascular Inflammation
47170c01.800 bronchocentric inflammation lung bronchovascular bundle chest inflammation peribronchial halo air trapping mosaic perfusion ground glass changes alveolar change air bronchogram acute bronchovascular inflammation ddx allergic collagen vascular disease infection CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47170c01.800 bronchocentric inflammation lung bronchovascular bundle chest inflammation peribronchial halo air trapping mosaic perfusion ground glass changes alveolar change air bronchogram acute bronchovascular inflammation ddx allergic collagen vascular disease infection CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47170c01.800 bronchocentric inflammation lung bronchovascular bundle chest inflammation peribronchial halo air trapping mosaic perfusion ground glass changes alveolar change air bronchogram acute bronchovascular inflammation ddx allergic collagen vascular disease infection CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Bronchovascular Inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Bronchovascular Inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Pneumonitis Secondary to Chemotherapy ? Drug Reaction
47095 lung chest fx lobar infiltrates fx air bronchogram dx chemotherapy related pneumonitis acute inflammation CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Pneumonitis Secondary to Chemotherapy ? Drug Reaction
47095 lung chest fx lobar infiltrates fx air bronchogram dx chemotherapy related pneumonitis acute inflammation CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47095 lung chest fx lobar infiltrates fx air bronchogram dx chemotherapy related pneumonitis acute inflammation CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47095 lung chest fx lobar infiltrates fx air bronchogram dx chemotherapy related pneumonitis acute inflammation CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Pneumonitis Secondary to Chemotherapy ? Drug Reaction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Pneumonitis Secondary to Chemotherapy ? Drug Reaction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Polyarteritis Nodosa
Occlusive Vascular Disease: Causes of Vascular Occlusion ? Polyarteritis Nodosa. This is a medium power photomicrograph from a bowel in a patient with Polyarteritis Nodosa. Bowel is commonly affected in this disorder. The medium sized artery seen here has undergone a deeply eosinophilic (fibrinoid) change. Notice that there is a surrounding inflammatory infiltrate of WBCs and formation of aneurysmal dilatation. This can result in massive hemorrhage if the aneurysm ruptures. colon large bowel artery small bowel fx aneurysm inflammation dx polyarteritis nodosa histopathology Courtesy Barbara Banner MD 12889
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Polyarteritis Nodosa
Occlusive Vascular Disease: Causes of Vascular Occlusion ? Polyarteritis Nodosa. This is a medium power photomicrograph from a bowel in a patient with Polyarteritis Nodosa. Bowel is commonly affected in this disorder. The medium sized artery seen here has undergone a deeply eosinophilic (fibrinoid) change. Notice that there is a surrounding inflammatory infiltrate of WBCs and formation of aneurysmal dilatation. This can result in massive hemorrhage if the aneurysm ruptures. colon large bowel artery small bowel fx aneurysm inflammation dx polyarteritis nodosa histopathology Courtesy Barbara Banner MD 12889
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Occlusive Vascular Disease: Causes of Vascular Occlusion ? Polyarteritis Nodosa. This is a medium power photomicrograph from a bowel in a patient with Polyarteritis Nodosa. Bowel is commonly affected in this disorder. The medium sized artery seen here has undergone a deeply eosinophilic (fibrinoid) change. Notice that there is a surrounding inflammatory infiltrate of WBCs and formation of aneurysmal dilatation. This can result in massive hemorrhage if the aneurysm ruptures. colon large bowel artery small bowel fx aneurysm inflammation dx polyarteritis nodosa histopathology Courtesy Barbara Banner MD 12889
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Occlusive Vascular Disease: Causes of Vascular Occlusion ? Polyarteritis Nodosa. This is a medium power photomicrograph from a bowel in a patient with Polyarteritis Nodosa. Bowel is commonly affected in this disorder. The medium sized artery seen here has undergone a deeply eosinophilic (fibrinoid) change. Notice that there is a surrounding inflammatory infiltrate of WBCs and formation of aneurysmal dilatation. This can result in massive hemorrhage if the aneurysm ruptures. colon large bowel artery small bowel fx aneurysm inflammation dx polyarteritis nodosa histopathology Courtesy Barbara Banner MD 12889
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Polyarteritis Nodosa
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Polyarteritis Nodosa
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Takayasu?s Arterirtis
The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Takayasu?s Arterirtis
The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Takayasu?s Arterirtis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Takayasu?s Arterirtis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Kawasaki Arteritis and Coronary Artery Aneurysm
07587 heart cardiac aneursym coronary artery Kawasaki?s areteritis grosspathology Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Kawasaki Arteritis and Coronary Artery Aneurysm
07587 heart cardiac aneursym coronary artery Kawasaki?s areteritis grosspathology Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 07587 heart cardiac aneursym coronary artery Kawasaki?s areteritis grosspathology Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 07587 heart cardiac aneursym coronary artery Kawasaki?s areteritis grosspathology Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Kawasaki Arteritis and Coronary Artery Aneurysm
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Kawasaki Arteritis and Coronary Artery Aneurysm
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Takayasu?s Arterirtis
The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Takayasu?s Arterirtis
The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The series of images are from the angiogram of a 14 year old female who presented with seizures and an elevated blood pressure. Images a and b show multiple stenoses within the carotids best seen at the level of the bifurcation into external and internal arteries. In addition in b, the aortic arch shows non critical narrowing just after the origin of the left common carotid vessel. Note that the right subclavian artery is not seen and presumably is accluded at its origin. The abdominal angiogram shows a significant narrowing of the left renal artery with post stenotic dilitation, and stenotic disease in the infrarenal abdominal aorta. The multicentric nature of the disease in a young female is athognomonic of Takayasu?s arteritis. 35155c Courtesy of Laura Feldman MD. code CVS artery aorta arteritis inflammation Takayasu?s carotid thorax arch renal abdomen pulseless
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Takayasu?s Arterirtis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Takayasu?s Arterirtis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Takayasu?s Aortitis
16917b aorta fx irregular fx narrow dx Takayasu arteritis imaging radiology MRI Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Takayasu?s Aortitis
16917b aorta fx irregular fx narrow dx Takayasu arteritis imaging radiology MRI Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 16917b aorta fx irregular fx narrow dx Takayasu arteritis imaging radiology MRI Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 16917b aorta fx irregular fx narrow dx Takayasu arteritis imaging radiology MRI Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Takayasu?s Aortitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Takayasu?s Aortitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Calcific Myocarditis
This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 code heart septum dense calcific calcified calcification myocarditis inflammation cardiac imaging radiology CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Calcific Myocarditis
This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 code heart septum dense calcific calcified calcification myocarditis inflammation cardiac imaging radiology CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 code heart septum dense calcific calcified calcification myocarditis inflammation cardiac imaging radiology CTscan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 code heart septum dense calcific calcified calcification myocarditis inflammation cardiac imaging radiology CTscan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Calcific Myocarditis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Calcific Myocarditis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Sarcoidosis of the Heart
49740c01 34 male with sarcoidosis presents with dizzineess and complete heart block cardiac heart LV sarcoidosis complete heart blosk early gadolinium delayed gadolinium enhancement of the LV wall left ventricle inflammation MRI T1 Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Sarcoidosis of the Heart
49740c01 34 male with sarcoidosis presents with dizzineess and complete heart block cardiac heart LV sarcoidosis complete heart blosk early gadolinium delayed gadolinium enhancement of the LV wall left ventricle inflammation MRI T1 Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49740c01 34 male with sarcoidosis presents with dizzineess and complete heart block cardiac heart LV sarcoidosis complete heart blosk early gadolinium delayed gadolinium enhancement of the LV wall left ventricle inflammation MRI T1 Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49740c01 34 male with sarcoidosis presents with dizzineess and complete heart block cardiac heart LV sarcoidosis complete heart blosk early gadolinium delayed gadolinium enhancement of the LV wall left ventricle inflammation MRI T1 Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Sarcoidosis of the Heart
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Sarcoidosis of the Heart
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Sarcoidosis Involving the Basal Meninges
40406c Courtesy Ashley Davidoff MD code lung fx interstium fx thickening dx interstitial lung disease ILD code pancreas abdomen lymph nodes fx calcified code brain meninges fx calcifications code dx sarcoidosis imaging radiology CT scan code inflammation immune
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Sarcoidosis Involving the Basal Meninges
40406c Courtesy Ashley Davidoff MD code lung fx interstium fx thickening dx interstitial lung disease ILD code pancreas abdomen lymph nodes fx calcified code brain meninges fx calcifications code dx sarcoidosis imaging radiology CT scan code inflammation immune
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 40406c Courtesy Ashley Davidoff MD code lung fx interstium fx thickening dx interstitial lung disease ILD code pancreas abdomen lymph nodes fx calcified code brain meninges fx calcifications code dx sarcoidosis imaging radiology CT scan code inflammation immune
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 40406c Courtesy Ashley Davidoff MD code lung fx interstium fx thickening dx interstitial lung disease ILD code pancreas abdomen lymph nodes fx calcified code brain meninges fx calcifications code dx sarcoidosis imaging radiology CT scan code inflammation immune
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Sarcoidosis Involving the Basal Meninges
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Sarcoidosis Involving the Basal Meninges
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Left Maxillary Sinusitis Complicated by Brain Abscess ? MRI
71604.c03 40 year old female with headache brain maxillary sinus frontal lobe fx air fluid level parafalcine falx cerebri a= T1 weighted b= T2 weighted c = T2 weighted d= FLAIR dx acute on chronic left maxillary sinusitis with brain abscess air fluid level thickened mucosa of maxillary sinus MRI Davidoff MD 71604.c02 71604.c03 71604.c04 71604.c02b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Left Maxillary Sinusitis Complicated by Brain Abscess ? MRI
71604.c03 40 year old female with headache brain maxillary sinus frontal lobe fx air fluid level parafalcine falx cerebri a= T1 weighted b= T2 weighted c = T2 weighted d= FLAIR dx acute on chronic left maxillary sinusitis with brain abscess air fluid level thickened mucosa of maxillary sinus MRI Davidoff MD 71604.c02 71604.c03 71604.c04 71604.c02b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71604.c03 40 year old female with headache brain maxillary sinus frontal lobe fx air fluid level parafalcine falx cerebri a= T1 weighted b= T2 weighted c = T2 weighted d= FLAIR dx acute on chronic left maxillary sinusitis with brain abscess air fluid level thickened mucosa of maxillary sinus MRI Davidoff MD 71604.c02 71604.c03 71604.c04 71604.c02b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71604.c03 40 year old female with headache brain maxillary sinus frontal lobe fx air fluid level parafalcine falx cerebri a= T1 weighted b= T2 weighted c = T2 weighted d= FLAIR dx acute on chronic left maxillary sinusitis with brain abscess air fluid level thickened mucosa of maxillary sinus MRI Davidoff MD 71604.c02 71604.c03 71604.c04 71604.c02b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Left Maxillary Sinusitis Complicated by Brain Abscess ? MRI
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Left Maxillary Sinusitis Complicated by Brain Abscess ? MRI
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Reflux Esophagitis
12253.800 esophagus cellular infiltrate inflammation stratified columnar epithelium reflux esophagitis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Reflux Esophagitis
12253.800 esophagus cellular infiltrate inflammation stratified columnar epithelium reflux esophagitis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 12253.800 esophagus cellular infiltrate inflammation stratified columnar epithelium reflux esophagitis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 12253.800 esophagus cellular infiltrate inflammation stratified columnar epithelium reflux esophagitis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Reflux Esophagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Reflux Esophagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Pancreatitis
This patient presented with acute abdominal pain following an alcoholic binge. The pancreas shown in pink in image b, looks relatively normal, but is surrounded by a exudate (red ) which is characteristic of this entity. The exudate has extended around the colon (white surrounded by red ring on the left side)
. 40396c02 Courtesy Ashley Davidoff MD code abdomen colon colon cutoff sign code pancreas pancreatic tail fx induration exudate code anterior pararenal space left colic gutter Gerota?s fascia lateral conal ligament fx thickened lcode liver hypodensity dx steatosis fatty liver code dx acute alcoholic pancreatitis with fatty change in the liver and colonic narrowing imaging radiology plain film CTscan acute inflammation mechanical
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Pancreatitis
This patient presented with acute abdominal pain following an alcoholic binge. The pancreas shown in pink in image b, looks relatively normal, but is surrounded by a exudate (red ) which is characteristic of this entity. The exudate has extended around the colon (white surrounded by red ring on the left side)
. 40396c02 Courtesy Ashley Davidoff MD code abdomen colon colon cutoff sign code pancreas pancreatic tail fx induration exudate code anterior pararenal space left colic gutter Gerota?s fascia lateral conal ligament fx thickened lcode liver hypodensity dx steatosis fatty liver code dx acute alcoholic pancreatitis with fatty change in the liver and colonic narrowing imaging radiology plain film CTscan acute inflammation mechanical
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This patient presented with acute abdominal pain following an alcoholic binge. The pancreas shown in pink in image b, looks relatively normal, but is surrounded by a exudate (red ) which is characteristic of this entity. The exudate has extended around the colon (white surrounded by red ring on the left side)
. 40396c02 Courtesy Ashley Davidoff MD code abdomen colon colon cutoff sign code pancreas pancreatic tail fx induration exudate code anterior pararenal space left colic gutter Gerota?s fascia lateral conal ligament fx thickened lcode liver hypodensity dx steatosis fatty liver code dx acute alcoholic pancreatitis with fatty change in the liver and colonic narrowing imaging radiology plain film CTscan acute inflammation mechanical
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This patient presented with acute abdominal pain following an alcoholic binge. The pancreas shown in pink in image b, looks relatively normal, but is surrounded by a exudate (red ) which is characteristic of this entity. The exudate has extended around the colon (white surrounded by red ring on the left side)
. 40396c02 Courtesy Ashley Davidoff MD code abdomen colon colon cutoff sign code pancreas pancreatic tail fx induration exudate code anterior pararenal space left colic gutter Gerota?s fascia lateral conal ligament fx thickened lcode liver hypodensity dx steatosis fatty liver code dx acute alcoholic pancreatitis with fatty change in the liver and colonic narrowing imaging radiology plain film CTscan acute inflammation mechanical
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Pancreatitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Pancreatitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 70369c01 pancreas time acute pancreatitis before after enlarged fluid interstitial fluid inflammation kidney obstruction CTscan Davidoff MD 70369c02
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Before and After Acute Pncreatitis
Swelling of the Pancreas from Edema and Leakage of Pancreatic Fluid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chemical Peptic Esophagitis
73405 esophagus redness patches inflammation chemical acute esophagitis endoscopy Courtesy Joshua Namias
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chemical Peptic Esophagitis
73405 esophagus redness patches inflammation chemical acute esophagitis endoscopy Courtesy Joshua Namias
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 73405 esophagus redness patches inflammation chemical acute esophagitis endoscopy Courtesy Joshua Namias
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 73405 esophagus redness patches inflammation chemical acute esophagitis endoscopy Courtesy Joshua Namias
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chemical Peptic Esophagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chemical Peptic Esophagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Normal (left) and Abnormal (right) Red and Swollen GE junction ? Reflux Esophagitis
01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Normal (left) and Abnormal (right) Red and Swollen GE junction ? Reflux Esophagitis
01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Normal (left) and Abnormal (right) Red and Swollen GE junction ? Reflux Esophagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Normal (left) and Abnormal (right) Red and Swollen GE junction ? Reflux Esophagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Cholecystitis
16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Cholecystitis
16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Cholecystitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Cholecystitis with Transmural Induration
16203c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Cholecystitis with Transmural Induration
16203c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
16203c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
16203c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Cholecystitis with Transmural Induration
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Cholecystitis with Transmural Induration
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia
72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy?s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia
72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy?s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy?s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy?s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Swelling Supraorbital Region and Maxillary Sinus
48717b01 skin bone swelling acute traumatic injury inflammation fracture inferior orbital wall roof of maxillary sinus trauma 3D volume rendering CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Swelling Supraorbital Region and Maxillary Sinus
48717b01 skin bone swelling acute traumatic injury inflammation fracture inferior orbital wall roof of maxillary sinus trauma 3D volume rendering CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 48717b01 skin bone swelling acute traumatic injury inflammation fracture inferior orbital wall roof of maxillary sinus trauma 3D volume rendering CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 48717b01 skin bone swelling acute traumatic injury inflammation fracture inferior orbital wall roof of maxillary sinus trauma 3D volume rendering CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Swelling Supraorbital Region and Maxillary Sinus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Swelling Supraorbital Region and Maxillary Sinus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Transudation and Exudation Causing Swelling
71695c02 colon splenic flexure fx fat induration dirty fat Gerotas fascia lateral conal fascia thickened thickening of the interstitium acute inflammation inflammatory exudate diverticulitis large bowel CTscan Davidoff MD 71695c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Transudation and Exudation Causing Swelling
71695c02 colon splenic flexure fx fat induration dirty fat Gerotas fascia lateral conal fascia thickened thickening of the interstitium acute inflammation inflammatory exudate diverticulitis large bowel CTscan Davidoff MD 71695c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71695c02 colon splenic flexure fx fat induration dirty fat Gerotas fascia lateral conal fascia thickened thickening of the interstitium acute inflammation inflammatory exudate diverticulitis large bowel CTscan Davidoff MD 71695c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71695c02 colon splenic flexure fx fat induration dirty fat Gerotas fascia lateral conal fascia thickened thickening of the interstitium acute inflammation inflammatory exudate diverticulitis large bowel CTscan Davidoff MD 71695c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Transudation and Exudation Causing Swelling
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Transudation and Exudation Causing Swelling
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Arteries, Veins and Lymphatics in the Gallbladder Fossa
00140 gallbladder wall gallbladder fossa normal artery duct liver interface histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Arteries, Veins and Lymphatics in the Gallbladder Fossa
00140 gallbladder wall gallbladder fossa normal artery duct liver interface histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 00140 gallbladder wall gallbladder fossa normal artery duct liver interface histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 00140 gallbladder wall gallbladder fossa normal artery duct liver interface histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Arteries, Veins and Lymphatics in the Gallbladder Fossa
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Arteries, Veins and Lymphatics in the Gallbladder Fossa
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cystic Arterioles and Venules in the Submucosa
82006c05.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cystic Arterioles and Venules in the Submucosa
82006c05.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 82006c05.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82006c05.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cystic Arterioles and Venules in the Submucosa
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cystic Arterioles and Venules in the Submucosa
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cystic Arterioles in the Submucosa ? Hyperemia
82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cystic Arterioles in the Submucosa ? Hyperemia
82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles submucosa wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cystic Arterioles in the Submucosa ? Hyperemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cystic Arterioles in the Submucosa ? Hyperemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Calculous Cholecystitis
This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 ? 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction.11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Calculous Cholecystitis
This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 ? 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction.11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 ? 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction.11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 ? 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction.11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Calculous Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Calculous Cholecystitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Bile Inciting Inflammation
This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The ?granulomas? are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Bile Inciting Inflammation
This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The ?granulomas? are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The ?granulomas? are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The ?granulomas? are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Bile Inciting Inflammation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Bile Inciting Inflammation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hemorrhagic Congestion in the Gallbladder Wall
00151 gallbladder wall inflammation acute cholecystitis histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hemorrhagic Congestion in the Gallbladder Wall
00151 gallbladder wall inflammation acute cholecystitis histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 00151 gallbladder wall inflammation acute cholecystitis histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 00151 gallbladder wall inflammation acute cholecystitis histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hemorrhagic Congestion in the Gallbladder Wall
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hemorrhagic Congestion in the Gallbladder Wall
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Cholecystitis
This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall.11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Cholecystitis
This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall.11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall.11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall.11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Cholecystitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Radiation Hepatitis ? Hyperemia
The straight line and the hyperemia are characteristis features radiation induced change22975 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Radiation Hepatitis ? Hyperemia
The straight line and the hyperemia are characteristis features radiation induced change22975 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The straight line and the hyperemia are characteristis features radiation induced change22975 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The straight line and the hyperemia are characteristis features radiation induced change22975 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Radiation Hepatitis ? Hyperemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Radiation Hepatitis ? Hyperemia
)