Imaging the Brain
Sumit Karia MD and Ashley Davidoff MD
The Common Vein Copyright 2010
Introduction
Several medical conditions often require, for their diagnosis, that certain findings are present in imagiological studies, many of which are discussed in the chapters for the diseases described. However, the science of Medicine is actually an art, and thus, the decision regarding which and if and imaging study is indicated is multifactorial, depending upon the specific clinical situation and the availability of the test. Generally, CT is the preferred study to identify acute hemorrhages, bony abnormalities and calcifications. MRI provides formidable imaging of the brain parenchyma.
Many categories of conditions can be made; the following represent circumstances in which such studies are deemed necessary for an accurate and final diagnosis:
Head trauma, there being:
Change in mental status
Signs of increased intracranial pressure.
Loss of consciousness
New neurological deficits.
Seizures
Worsening headaches
Skull fracture.
Suspected intracranial hemorrhage
CT or MRI are in these cases medically necessary. The former is preferred when there is suspicion for hemorrhage, acute subdural/epidural hematoma and fracture. MRI is preferred for suspected shearing lesions and diffuse axonal injury in closed head trauma, as well as for evaluation of subacute and chronic sequelae of head injuries.
Cerebrovascular accident, where there can be changes in motor, sensory, visual, behavioral and cognitive functions.
CT or MRI are necessary.
When symptoms develop in less than 90 minutes, there is a possibility to intervene with thrombolysis or IR guided thrombectomy. In this situation, there is necessity to exclude hemorrhage or mass, which is better evaluated with CT is indicated (hyperacute setting).
MRI is indicated to detect subtle mass effects that may be associated with acute hemorrhagic infarction. It can also give information about the timing of the hemorrhage, that is, if it is hyperacute, acute, or chronic. It is very useful in the evaluation of infarcts in the brain stem and deep white matter infarcts / lacunar infarcts, since CT cannot give as much detail in these regions, yielding many times false negatives.
Inflammation and infection, for instance, abscess formation, encephalitis.
CT or MRI are the modalities indicated, MRI being preferred for evaluating bacterial, fungal and parasitic abscesses (i.e., cysticercosis), ependymitis and subdural empyemas.
Headache
The differential diagnosis includes hemorrhage, mass lesions. These are of more suspicion when headaches are accompanied by symptoms of increased intracranial pressure or suggest intracranial bleeding.
Again, CT or MRI are indicated if this headache has given characteristics:
Sudden very severe headache
With suspicion of intracranial lesion
Exacerbation of chronic headache with neurologic signs, such as motor or mental status changes
Chronic headache with increase in frequency or severity
If associated with fever and meningeal symptoms
If there is history of cancer or AIDS
If they awake patients from sleep
If they are exertional
Malignant and benign lesions
Both CT and MRI are necessary for the evaluation before and after therapy of malignant lesions treated with surgery, chemotherapy, or radiation.
MRI is preferred for evaluating the posterior fossa and primary intraaxial or extraaxial tumors (gliobastoma, astrocytoma, lymphoma, acoustic neuromas, menigiomas, cholesteotomas, etc.) and pituitary adenomas.
Demyelinating diseases
When there is a suspicion for multiple sclerosis or acute disseminated encephalomyelitis MRI is considered necessary for its diagnosis. Central nervous system demyelination will be observed and this is seen on MRI. Leukodystrophies, central pontine myelinolysis, progressive multifocal leukoencephalopathy are examples of other demyelinating diseases, less frequent, that can be diagnosed by observation of CNS demyelination in MRI, in conjunction with clinical findings.
Structural abnormalities
Due to the incredible detail MRI provides, it is the exam of choice in these evaluations:
Chiari I & II malformations. This set of malformations are part of a group of congenital abnormalities that involve components of the cranio-cervical junction (hindbrain abnormalities).
Congenital lesions such as Dandy-Walker malformations, craniosynostosis, macrocephaly, microcephaly)
Hydrocephalus – for the initial evaluation hydrocephalus. CT is chosen when goal is to follow degree of hydrocephalus in shunted patient
Vascular abnormalities (e.g., aneurysm, arteriovenous malformations, venous capillary and cavernous angiomas, venous thrombosis) ? MRI, more specifically MRA
Non-Traumatic and Non-CVA related Hemorrhage
In suspicion of hypertensive hemorrhage.
Spontaneous hemorrhage in patients at risk for bleeding, such as those receiving anticoagulation therapy.
Other CNS indications (not absolute):
Suspicion of TIA / stroke
New onset of seizure activity
Papilledema
Visual field loss, diplopia or other visual changes that remain unexplained after ophthalmologic evaluation
Dementia
Focal neurologic deficit unexplained by clinical history
Change in mental status
Suspicion of degenerative neurologic process (e.g. ataxia, dyskinesia)
Suspicion of hypothalamic / pituitary lesion.
Parkinson?s disease
Persistent tinnitus
Further evaluation of changes detected in other radiologic exams, if clinically warranted (e.g. for therapeutic decision)
Symptoms of increased intracranial pressure, for decision of safety of performance of lumbar puncture (risk of herniation).
For the following, MRI is the recommended study and is considered necessary, in the presence of progressive asymmetrical hearing loss associated with:
Abnormal neurological evaluation
Vertigo, syncope and dizziness
Abnormal electronystagmography, audiometry or auditory brainstem response
When symptoms persist and evaluation other etiologies have been ruled out
Neurosurgical procedures:
Pre-operative evaluation prior to neurosurgery involving craniotomy, craniofacial surgery, cranial nerve procedures or a biopsy of the central nervous system.
Evaluation of hydrocephalus.
Evaluation of shunt for hydrocephalus or its revision.
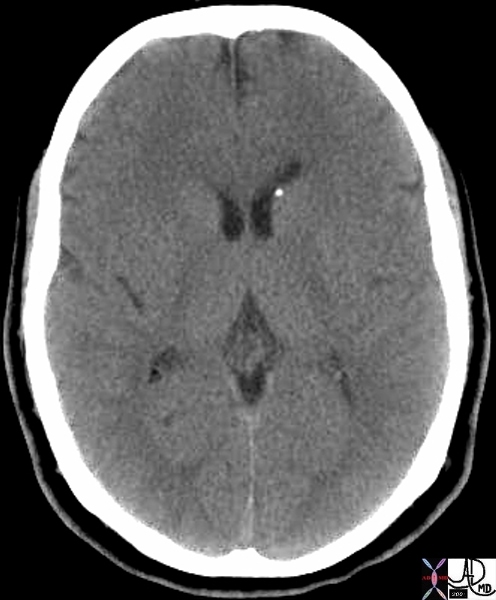
Subependymal Calcification DDX CMV Toxoplasmosis, Rubella |
| 49498 brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirius toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD |

Acute and Chronic Infarction with CT and DWI MRI |
| 49679c01 brain DWI occipital lobe fx vague hypodensity right occipital lobe with encephalomalacia and ex vacuo changes in the left occipital and posterior parietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe CTscan high intesity in right occipital lobe and low intensity in left occipitoparietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe MRI diffusion weighted imaging Courtesy Ashley Davidoff MD |
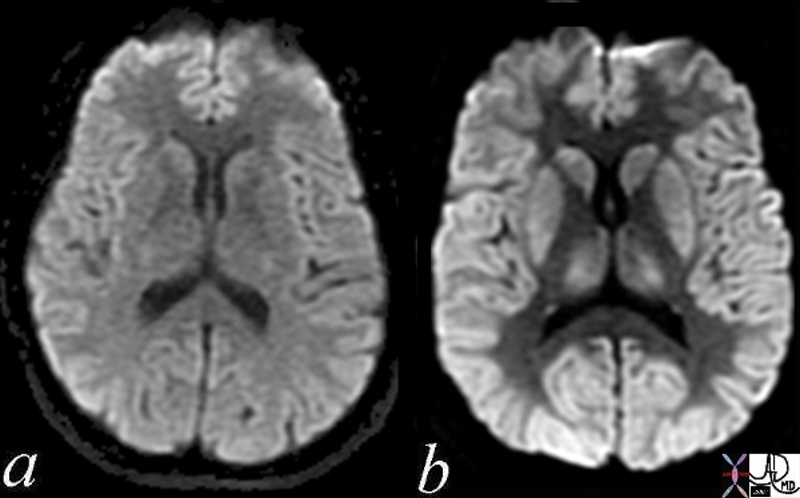
Normal and Global Ischemia after Cardiac Arrest |
| The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD |

Cisternogram |
| 49689.800 CSF flow brain cisternogram radioisotope injected into subarachnoid space via lumbar puncture and over 6.5 hours progresses to base of brain. This patient had a CSF leak in the cribiform plate. Hernose was plugged with cotton gauze and the gauze was scanned after 6 hours – The left and right were both positive for leak greater on the right nuclear medicine Courtesy Alan Ashare MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Cisternogram
49689.800 CSF flow brain cisternogram radioisotope injected into subarachnoid space via lumbar puncture and over 6.5 hours progresses to base of brain. This patient had a CSF leak in the cribiform plate. Hernose was plugged with cotton gauze and the gauze was scanned after 6 hours – The left and right were both positive for leak greater on the right nuclear medicine Courtesy Alan Ashare MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cisternogram
49689.800 CSF flow brain cisternogram radioisotope injected into subarachnoid space via lumbar puncture and over 6.5 hours progresses to base of brain. This patient had a CSF leak in the cribiform plate. Hernose was plugged with cotton gauze and the gauze was scanned after 6 hours – The left and right were both positive for leak greater on the right nuclear medicine Courtesy Alan Ashare MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49689.800 CSF flow brain cisternogram radioisotope injected into subarachnoid space via lumbar puncture and over 6.5 hours progresses to base of brain. This patient had a CSF leak in the cribiform plate. Hernose was plugged with cotton gauze and the gauze was scanned after 6 hours – The left and right were both positive for leak greater on the right nuclear medicine Courtesy Alan Ashare MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49689.800 CSF flow brain cisternogram radioisotope injected into subarachnoid space via lumbar puncture and over 6.5 hours progresses to base of brain. This patient had a CSF leak in the cribiform plate. Hernose was plugged with cotton gauze and the gauze was scanned after 6 hours – The left and right were both positive for leak greater on the right nuclear medicine Courtesy Alan Ashare MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cisternogram
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cisternogram
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal and Global Ischemia after Cardiac Arrest
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Global Ischemia after Cardiac Arrest
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Global Ischemia after Cardiac Arrest
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Global Ischemia after Cardiac Arrest
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute and Chronic Infarction with CT and DWI MRI
49679c01 brain DWI occipital lobe fx vague hypodensity right occipital lobe with encephalomalacia and ex vacuo changes in the left occipital and posterior parietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe CTscan high intesity in right occipital lobe and low intensity in left occipitoparietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe MRI diffusion weighted imaging Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute and Chronic Infarction with CT and DWI MRI
49679c01 brain DWI occipital lobe fx vague hypodensity right occipital lobe with encephalomalacia and ex vacuo changes in the left occipital and posterior parietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe CTscan high intesity in right occipital lobe and low intensity in left occipitoparietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe MRI diffusion weighted imaging Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49679c01 brain DWI occipital lobe fx vague hypodensity right occipital lobe with encephalomalacia and ex vacuo changes in the left occipital and posterior parietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe CTscan high intesity in right occipital lobe and low intensity in left occipitoparietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe MRI diffusion weighted imaging Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49679c01 brain DWI occipital lobe fx vague hypodensity right occipital lobe with encephalomalacia and ex vacuo changes in the left occipital and posterior parietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe CTscan high intesity in right occipital lobe and low intensity in left occipitoparietal region dx acute infarction right occipital lobe chronic infarction left occipital lobe MRI diffusion weighted imaging Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute and Chronic Infarction with CT and DWI MRI
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute and Chronic Infarction with CT and DWI MRI
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Subependymal Calcification DDX CMV Toxoplasmosis, Rubella
49498 brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirius toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Subependymal Calcification DDX CMV Toxoplasmosis, Rubella
49498 brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirius toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49498 brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirius toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49498 brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirius toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Subependymal Calcification DDX CMV Toxoplasmosis, Rubella
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Subependymal Calcification DDX CMV Toxoplasmosis, Rubella
)
