The Common Vein copyright 2009
Niharika Dixit MD Ashley Davidoff MD
Definition
Cancer is an aggressive growth disorder initiated by a cell or a group of renegade cells with genetic aberrance, usually caused by either a carcinogen in the environment, or less commonly by an inherited genetic abnormality.
The structural changes are characterized by aberrant space occupation of tissue with a variety of macroscopic morphologies, but often characterized at a cellular level by large hyperchromatic nuclii with diminished cytoplasm.
Functionally the rebel cells and cell group parasitize nutrition and oxygen, but do not contribute to the overall function of the mother organ or to the community at large.
The disease is complicated by local spread within the organ and surrounding tissues, displacing well meaning and well functioning tissue. Continued uncontrolled growth results in the invasion of blood vessels and lymphatics and spread to distant organs where metastatic disease repeats the pattern of continued advance of rebellious and aggressive parasitization of normal tissue. Other local complications include bleeding, necrosis, and obstruction. Systemic and non specific complications include fatigue, weight loss, night sweats and pain
The diagnosis is suspected clinically when an older patient presents with unexplained weight loss, or a new mass is felt on clinical examination.
Imaging characteristics include finding a mass, characteristically with a spiculated appearance, that shows evidence of local invasion or a metastatic pattern. PET scan is able to characterize the metabolic pattern of disease, and cancer typically is hypermetabolic. When cancer is suspected, pathological confirmation is almost universally indicated to confirm the diagnosis, and to evaluate and classify the type and virulence of the cancer. Types of biopsy include aspiration technique where individual cells are sucked up into a needle, core biopsy where a cutting needle provides a small sample of tissue, and incisional biopsy where a part of a lump or a sample is removed using a scalpel.
Staging the disease is essential in the diagnostic workup since treatment plans depend on the extent and location of the disease.
Treatment options depend on staging of the cancer. In the early stages the goal of treatment is cure and may include surgical resection. In advanced stages the role of treatment is control of disease and prolongation of life. This may include surgery, chemotherapy and radiation. Recent advances include localized chemical ablation with alcohol for example, or thermal or electrical ablation.
|

The Malignant Process Left Unchecked
|
| The nature of malignancy is outlined in the evolution of a malignant cell in the gastrointestinal tract. The bowel consists of 4 basic layers with an inner epithelial layer (pink) a submucosal layer (yellow), a muscular layer (red) and an outer serosal or adventitial layer (blue). The bowel lumen lies between two layers of bowel wall (black and white). In image 1, a single cell of the mucosa seen in the background of white, becomes “aberrant” and plays no role in the function of the mucosa. It multiplies and its progeny occupies a larger space (image 2). As it continues to grow it breaks through the mucosa and into the submucosa (yellow) and muscularis (red) in 3. Its uninhibited growth into the veins (blue) and lymph nodes (orange) results in metastatic disease to secondary sites. In the meantime it continues to invade locally encircling the intestinal tract, narrowing the bowel lumen, and eventually causing obstruction of the tract. (image 5).
Courtesy Ashley Davidoff MD. 32336c |
Introduction
The normal process of cell growth and cell death is orderly. There is a time to live and a time to die. The process of timed cell death is called apoptosis literally meaning “dropping off” from the Greek apo = from and ptosis = falling, and is best equated to a similar event in botany of a petal falling off a flower. A series of biochemical events over time results in structural change in the nucleus, cytoplasm and cell membrane. with eventual “falling off” of the cell from the population at large. In health the cell is replaced. Between 50-70 billion cells die each day in the human adult.In cancer the orderly process of new cell growth and cell death is altered. There is uncontrolled cell division and growth and reduction in cell death. An imbalance occurs with a shift that favors the anti-apototic mechanisms over the pro-aptotic mechanisms and cells live past their age, and do not die.
A Cancer Cell – Aberrant Sense of Time
|
| The image represents the life of a single set of columnar cells showing a progression of generations as the cell lives dies and is regenerated. The orange secretions of the cell are seen in the background of the pink cytoplasm and the purple nucleus. The nucleus of the newest generation and cell is seen as a clock that has become distorted causing time to become disordered. This is the forerunner of a malignant process.
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198j03s.81s |
The abnormal cells also characteristically acquire the capability to invade surrounding structures as well as an ability to spread to distant organs through blood stream or lymphatics.
The malignant population of cells compete for nutritional resources and space.

Abnormal Programming Multiplication and Space Occupation
|
| The image represents the evolution of a single cancer cell (a) that fails to conform to the normal time cycle. In image a, the normal columnar mucosa is composed of rectangular cells supported by a thin purple basement membrane. One cell becomes aberrant, and is characterized by a large blue nucleus, scanty cytoplasm and a a change in it shape and overall appearance. The cell grows, multiplies, (b,c,d) and then invades the space of other parts of the tissue like the submucocsa (yellow) and muscular layer (maroon) in e and finally the serosal layer in f(outer white layer).
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198fc02.8s |
At a molecular level, the cancer cell acquires mutations which either results in down regulation of tumor suppressor genes or upregulation of cancer causing genes. Some of these mutations may code for a particular protein which may enhance cell growth and suppress the process of apoptosis (programmed cell death).
History of the Disease
Cancer has afflicted humans for centuries and knowledge gathered in earlier centuries laid a background for knowledge we have today. Cancer is derived from terms carcinos or carcinoma, which literally mean crab and was first used by Celsus. Galen used “oncos” to describe all tumors. (Karpozilos) Interestingly the earliest reports of cancer are found in Egypt in 1500 BC in on Papyrus documents describing eight patients with tumor of the breast. These documents describe tumors as incurable and local thermal cauterization as a palliative measures. There were multiple theories of what causes cancer, Ancient Egyptian believed it was caused by gods while Hippocrates blamed the imbalances in the balance of human body. It has taken many centuries to discern what causes cancer and even today the knowledge is far from complete. The modern oncology practice has made tremendous strides. Some cancers are now curable and a multitude of clinical trials are currently ongoing.
Principles
Cancer can affect any tissue of the body. Initial cancer is just a localized overgrowth of abnormal cells which is called carcinoma in situ. It is often difficult to diagnose at this stage. As these cells grow and acquire more invasiveness, tumor breaches the membranes and acquires the capacity to grow, invade other tissues and eventually develop the capacity to invade blood vessels and lymphatics. Once blood borne cancer cells can reach any organ of the body and develop secondary tumors called as metastasis. They are divided in to two major subtypes based on origin of the cells. Cancers arising from epithelial surfaces are known as carcinomas while tumors arising from connective tissue are known as sarcomas.
The cancer at its origin is called the primary cancer, and the distant cancer is called metastasis.
Carcinoma
Carcinoma is a malignant cancer that arises from epithelial cells. Epithelial cells form the inner lining of all the tubular systems of the body including the gastrointestinal tract, genitourinary tract and the airways. They also form the cellular matrix of all the glands including the liver, pancreas, and the breast. Carcinoma is classified into histological subtypes based on histopathological appearance. Adenocarcinoma arises from glandular epithelium. Adenocarcinoma may have its different subtypes based on appearance. Squamous cell carcinoma has appearance suggestive of squamous epithelium. Transitional cell carcinomas are seen arising from the urothelium. Anaplastic carcinomas are undifferentiated, and cellular makeup is varied, bizarre and cell type difficult to discern. As a rule carcinomas are referred to by specific organ of origin such as carcinoma of prostate or breast carcinoma. The cells of malignant tissue usually resemble each other as if they arise from a single cell line.
Normal Liver Cells
|
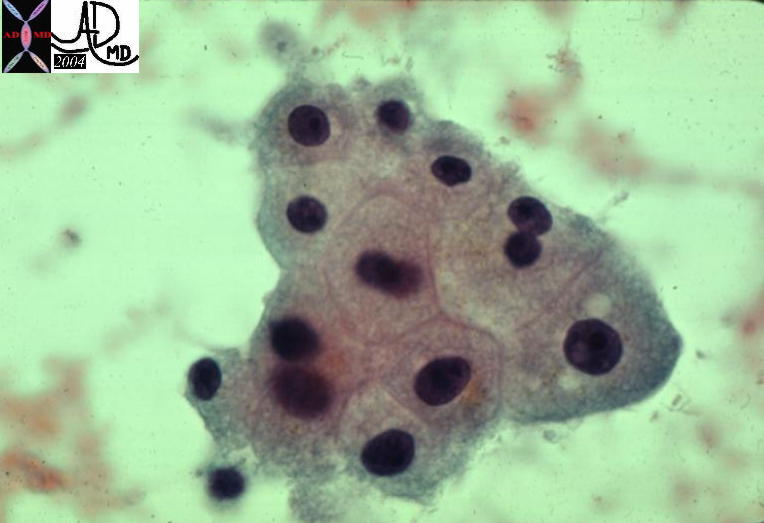
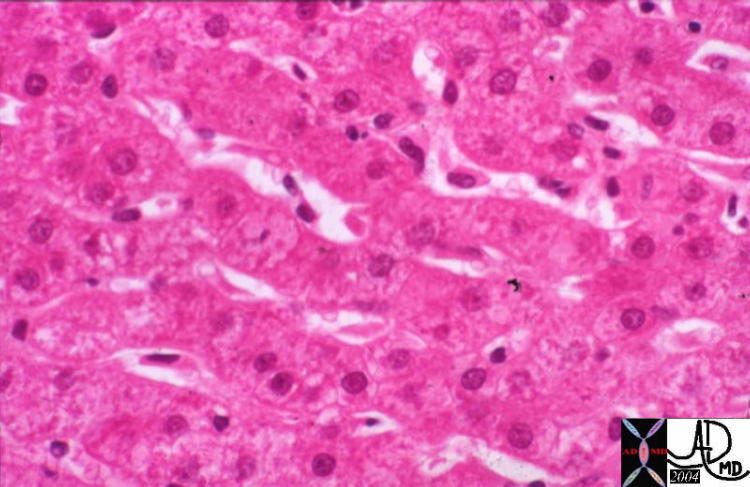
| The volume ratio of nucleus to cytoplasm is 1:4 or even 1:6 and the cytoplasm is a light pink (eosinophillic) The shape of the cell is polygonal.
13440 liver hepatocytes cells cytology histology normal 5star |
|
Malignant Liver Cells
|
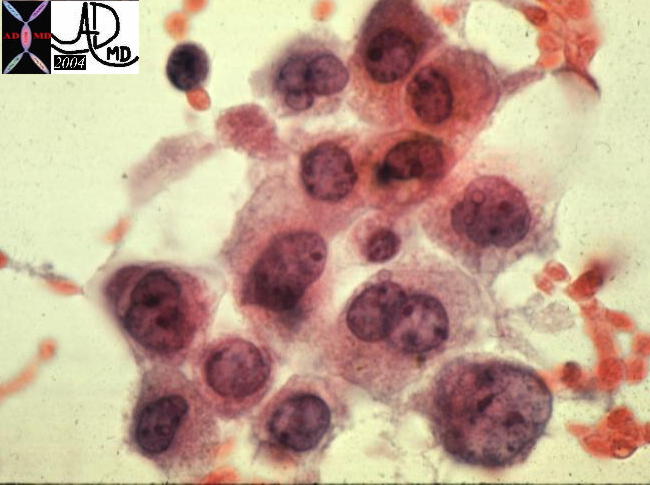
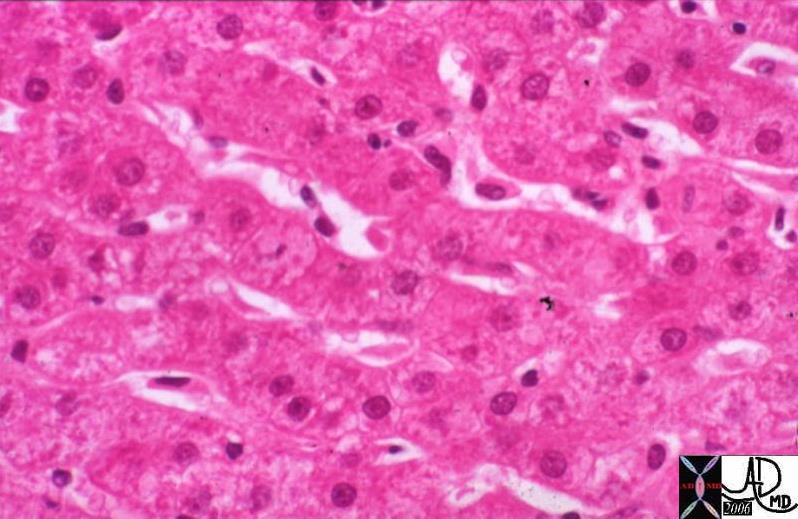
| In this cytopathology specimen the nuclear cytoplasmic ratio is closer to 1:1 and sometimes as in the cell in the lower right hand corner the nucleus is 4 or 5 times larger than the cytoplasm. This appearance is characteristic of malignant tissue. This is an example of a hepatocellular carcinoma.
13447 liver HCC hepatocellular carcinoma cytopathology |
|

Normal Colonic Mucosa
|
| This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, “test tube”-like arrangement of the straight tubular glands which comprise the colonic crypts. The nuclii are seen in orderly fashion at the base of the columnar cell as dark purple dots while the cytoplasm is seen with vacuoles of mucin reflecting a nuclear cytoplasmic ratio of 1:4 or even 1:6. The underlying submucosa is not seen in this image although submucosa between the crypts is noted.
12860 Normal Colon Mucosa. This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, ?test tube?-like arrangement of the straight tubular glands which comprise the colonic crypts. colon large bowel mucosa submucosa crypts histology Courtesy Barbara Banner MD 5star |
|

Colon Carcinoma
|
| The low power view of the malignant colonic mucosa shows somewhat normal mucosa to the left of the image, but ringed in purple in image b is a group of renegade cells that has broken away from the orderly “test tube” format and has advanced into the submucosa. Although it is difficult to evaluate accurately, very little cytoplasm can be appreciated and the overall “blueness” of the mass suggests hyperchromicity.
02746c02.8s The low power view of the malignant colonic mucosa shows basicar cells that have hyperchromicity, lack cytoplasm and have invaded into the submucosa code colon carcinoma malignant primary histopathology Courtesy Barbara Banner MD copyright 2009 allrights reserved GW question |
Sarcoma
Sarcoma is a less common form of cancer and represents an aggressive uncontrolled growth of connective tissue elements, bone, muscle, and fat . The word sar derives from the Greek word that means fleshy because this is the characteristic nature of the tissue. These arise from mesenchymal tissue which is the precursor of connective tissue, fat, bone and muscle.
Sarcomas are usually identified by the specific stromal tissue they arise from such as osteosarcoma (arising from bone) or leiomyosarcoma (arising from muscle), or liposarcomas (arising from fat). The grade is an important variable in sarcoma. The higher the grade of a sarcoma, the worse the prognosis.
The exact etiology of sarcoma is unknown but in some patients there is a genetic predisposition. An example of inherited soft tissue sarcomas is retinoblastoma. Other inherited connective tissue diseases that can predispose to malignancy include neurofibromatosis type 1, tuberous sclerosis, familial adenomatous polyposis, Li Fraumeni Syndrome and Werner’s syndrome.
Risk factors include radiation therapy during childhood, following carcinoma of the breast or cervix, and lymphoma.
Metastatic Leiomyosarcoma
|
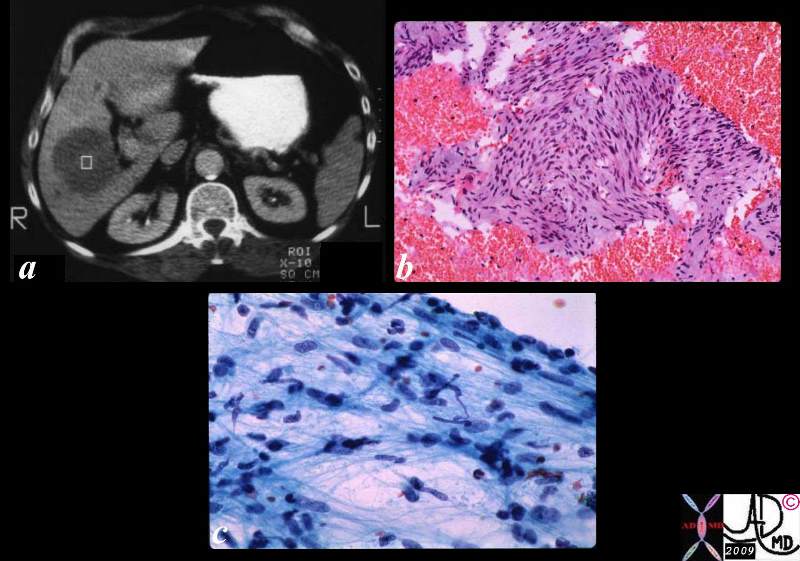
| The collage consists of a CT scan (a) showing a focal well circumscribed low density liver lesion. Biopsy of this lesion yielded the histopathological specimen (b) that shows hyperchromatic nuclii and spindle shaped cells, in a swirling pattern characteristic of leiomyosarcoma. The cytological aspirate (c) shows spindle shaped nuclii with pleomorphism and hyperchromicity.
code malignant cancer sarcoma histopathology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 03057c01.8s |
Metastasis
Metastatic disease is a malignant disorder in a secondary site remote from the primary cancer. It infers that the primary cancer has spread to another non-adjacent organ or part.
The spread of cancerous cells through the lymphatic system, the circulatory system, or both, enables the primary disease to spread to distant organs.
The origin of the word is Greek, and means displacement. The plural is metastases which is a word that is commonly abbreviated as “mets”.
The cause of the spread of cancer is due to an innate characteristic of malignant disease to detach from the primary site, advance into spaces and vessels, and grow in the secondary site. New populations of cells cloned from the original tumor grow and multiply in the secondary organ and present as a nodule or a mass in the new host organ.
Structurally the resulting cells at the secondary site are clones of the originating cell and have features that are identical to original tumor.
Certain cancers have the propensity to metastasize to certain organs. Colon cancer usually metastasizes to liver and prostate cancer usually metastasizes to bone.
Functional impairment depends on the site and extent of the metastatic disease. A small midbrain metastasis may impair vital function, while extensive metastases in the liver may be relatively asymptomatic. The predominant morbidity and mortality of cancer derives from metastatic disease.
Diagnosis is suspected clinically by symptoms specific to organ systems such new pain in a patient with know primary. This is commonly due to bone metastases. Advancing anorexia, malaise, or weight loss are systemic symptoms and signs that would raise the question of metastatic disease. Imaging studies such as CT scan, MRI or PET scans.
Metastatic disease is largely denoted as an incurable disease, though there are exceptions in certain circumstances.
Treatment options depend on the number and location of the metastasis, the size of the primary tumor and patient’s performance status.
For example a single small metastasis in lung or liver may be resected along with the primary tumor resulting in potential cure.
|

Primary Duodenal Cancer- Metastases to the Liver
|
| The post mortem specimen (a) shows a 2cms primary duodenal carcinoma (white arrow) with extensive nodular hepatic metastases occupying 80% of the liver. (b) In image c, the metastasis reflects an overall a blue hue caused by the increased nuclear presence. The image reveals an irregular and advancing threat on the normal liver. The higher power view in d, shows a rind of compressed liver that is in the process of destruction and hemorrhage (red patches) in the tumor, in the border, as well as in the normal liver. This image is reminiscent of an advancing enemy in a battlefield with victory apparent for the aggressor.
02643c03.8s code liver duodenum adenocarcinoma metastases metastasis cancer malignant space occupation pressure atrophy death grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved |
|
Infiltrative and Nodular Form
|
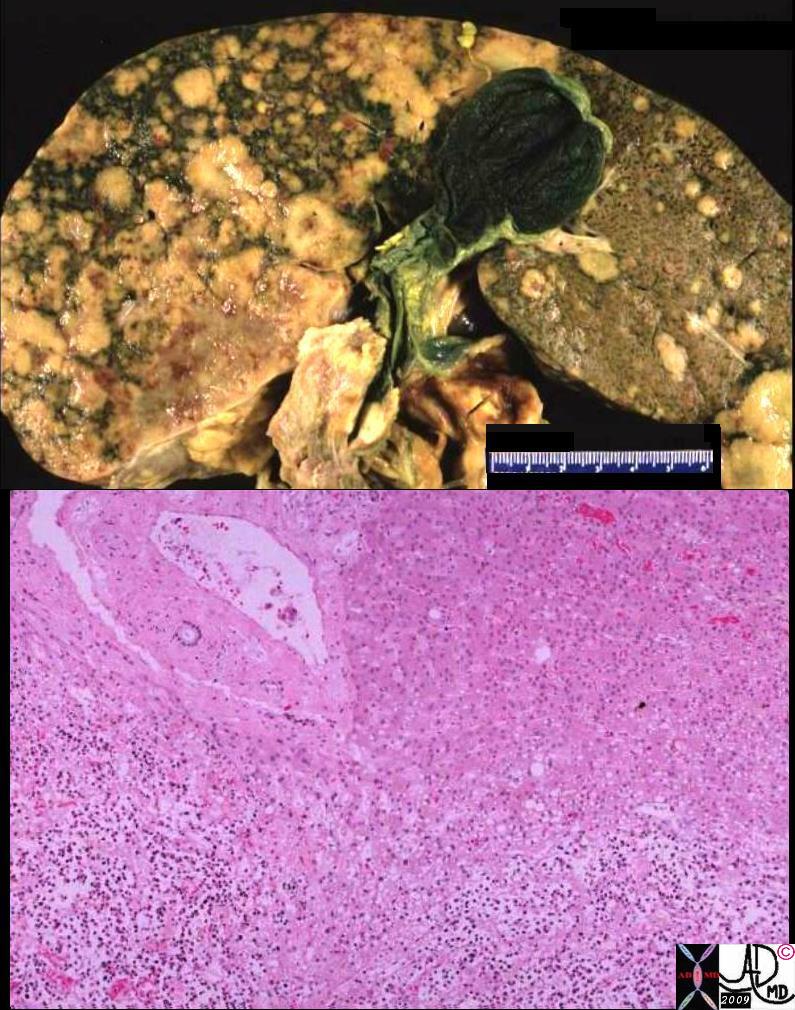
| The gross and histopathological specimens are from the autopsy of a patient who died of breast carcinoma that was metastatic to the liver. The right lobe of the liver shows two patterns of metastases. In the posterior aspect of the right lobe of the liver, there is diffuse disease, and in the anterior aspect there are innumerable nodules of varying sizes. The left lobe is relatively spared, and the pattern is of a nodular nature. The low power histopathological section shows a diffuse infiltrate of hyperchromatic malignant nuclii in the bottom of the image and relatively normal liver in the upper portion.
03034c.8s code liver metastases metastasis breast primary cancer malignant space occupation infiltration infiltrative pattern right lobe left lobe grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved GW question |
Cause of Cancer
What causes cancer?
In a human body, large a number of cells divide and form new cells to replace the cells that die by a process called apoptosis. Thus a balance of apoptosis and regeneration of new cells is crucial to human life. In a tumor, this balance is altered and either the cells are dividing too much or the cells lose their ability to undergo apoptosis. When a tumor acquires the ability to invade the surrounding tissue and also to spread to other organs it becomes a malignant tumor. The commonly associated agents that cause cancer include viruses, smoking, industrial exposure such as asbestos, hormonal factors and familial predisposition.
The exact etiology of cancer is not known. There are about 200 different types of cancer affecting all the different body tissues. What affects one body tissue may not affect another. A basic alteration and disorder in the genetic coding in general, is the underlying etiology
Genetic make up
Cancer is caused by alterations in oncogenes, tumor-suppressor genes, and microRNA genes. These alterations or mutations are usually acquired as a lifetime event (somatic events), although germ-line mutations can predispose a person to heritable or familial cancer. A single genetic change is rarely sufficient for the development of a malignant tumor. Most evidence points to a multistep process of sequential alterations in several, often many, oncogenes, tumor-suppressor genes, or microRNA genes in cancer cells (Croce). Rarely, some people are born with these mutations and there may be multiple family members with cancer. This is known as genetic predispositions. Some of these syndromes are well defined, such as BRCA1 and BRCA2 which are breast cancer genes that have a genetic predisposition. Women who carry one of these genetic mutations have a higher chance of developing breast cancer than women who do not. However, only 5% of breast cancers are associated with these mutations, and the majority are sporadic. However a history of breast cancer in a family member increases the risk of developing cancer multifold.
Carcinogens
Carcinogens are substances in the environment that can produce cancer. Smoking is a carcinogen and can cause many cancers but most commonly is associated with lung cancer. Excessive sun exposure is a carcinogen and may cause skin cancer. Asbestos exposure is associated with mesothelioma which is a specific type of lung cancer.
|
Nicotene
|
| These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d code RS pulmonary lung alveolus smake amoking cigarettes nicotene accessory pathology histopathology drawing |
Age:
Cancer occurs predominantly in older people, with nearly three quarters (74%) of cases diagnosed in people aged 60 and over, and more than a third of cases in people aged 75 and over ( Cancer Research UK). As human beings get older the elegant process of cell division is not be perfect, as cells acquire mutations and therefore cancers are more common.
Immune system:
Patients with immune disorders whether acquired or congenital are at a higher risk of cancer. For example there is a high risk of cancer in patient on immune suppression following organ transplant and in HIV positive individuals.
Diet:
Certain diets are associated with increased risk of cancer. Diet rich in animal fats and low in fresh fruits and vegetables are often blamed for causing cancer. In addition alcohol intake has been associated with breast cancer in women. Aflatoxin B1 is a carcinogen produced by the fungus Aspergillus flavus and is found on stored grains, nuts, and peanut butter.
Viruses:
Certain viruses such as Ebstein Barr virus, (EBV), human papilloma virus (HPV ) and hepatitis C are associated with cancer.(Joseph)
Structural Changes
Malignant disease is about aggressive space occupation by a group of cells that have no intent on contributing in a positive way to the society at large. Cells organs, people, families and nations have to have their own space in order to function and contribute to the society at large.
Aggressive Space Occupation
Aggressive space occupation is the structural nature of malignancy. Eventually space occupation either impedes the function of the mother organ, or it sends seedlings directly into the surrounding tissues, into the lymph nodes, and or via the circulation to distant organs where it takes up more space and further impedes function. Eventually the well meaning society succumbs, together with the parasite and all is lost to everybody.
The Battleground – Tumor vs Healthy Tissue
|
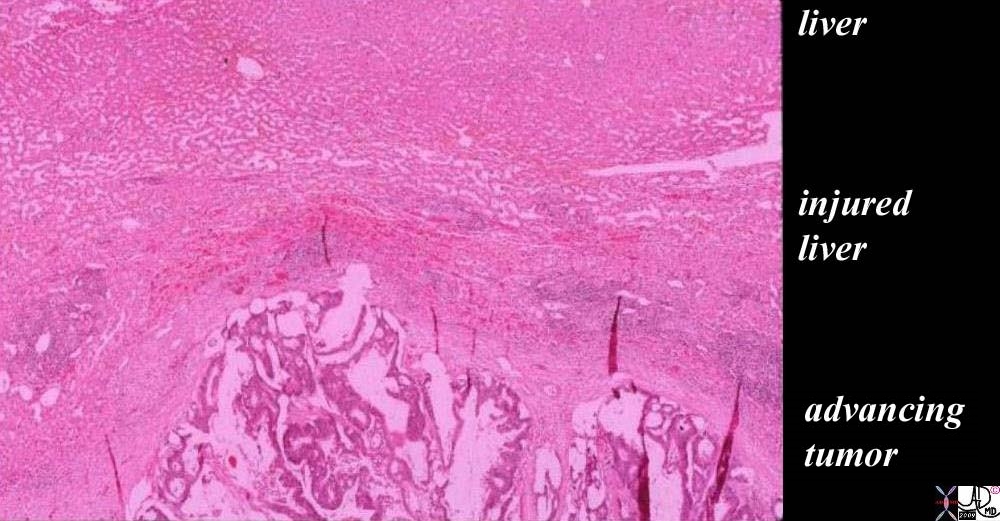
| The histopathology of a surgically resected hepatic metastasis from a primary colon carcinoma shows a mucinous secreting tumor at the bottom of the image labeled “advancing tumor”. The cellular detail is not well seen in the low power view but the columnar epithelial nature, hyperchromicity, and bizarre appearance of squatter tissue in the liver are recognized as malignant characteristics. The white spaces in between the cellular structure, represents mucin in the tumor. The edge of the tumor shows a rounded and aggressive push into the liver where the injured liver in the battlefield is recognized as compressed normal liver with linear areas of hemorrhage evidenced by a curvilinear line at 11 and 12 oclock of increased area of redness representing extravascular red cells (“layer of “injured liver”). The uppermost layer represents the normal liver which at this time looks healthy but is in jeopardy.
The The radial red spokes seen at the edge of the tumor are artifacts of preparation but are indicators of the direction of the battle.
03028b01.81s Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 5star |
|

The Battleground
|
| The reenactment of the war that was fought between the American revolutionaries seen here, and the loyalists to the English king depicts the battlefield in the fields of Lincoln Massachusetts in 1775. The concept of cancerous tissue vs normal in a battlefield has parallels . Left untreated the cancer is victorious. The normal well meaning tissues need assistance of clever therapies to attain victory. Left unchecked the cancer is inevitably victorious.
84022p.800 baby Lincoln Massachusetts Minuteman State PArk Reenactment of the days of the Revolution America circa 1775 men army gun horses Boston Davidoff photography |
|
Normal Liver – (left) and Cancer in the Liver (right)
|
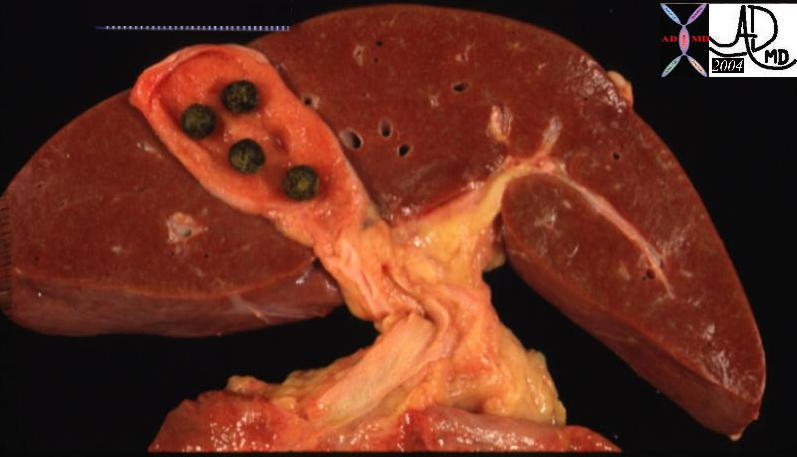
| The liver on the left is normal except for gallstones in the gallbladder. Gallstones are squatters but they usually do not have aggressive tendencies unless they block the outflow of bile. The liver shown in the right image is from a patient who succumbed to metastatic pancreatic carcinoma. The normal liver cells have been displaced and have been overridden by metastatic squatters. The metastases have contributed to the demise of the patient by their relentless displacement of normal tissue, causing progressive impairment of function.
13456 13448b01 liver normal anatomy gallbladder stones cholelithiasis grosspathology |
Normal Liver and Single Group of Cancer Cells
|
| These two cases represent the microscopic events described in the macroscopic examples above. The left image shows normal liver cords at high power, while the image on the right shows slightly lower power of the liver cords in pink, and a blue, rounded, space occupying metastasis.
13445 11440 liver cords sinusoids hepatocytes Kuppfer cells TCV concepts histology Courtesy Barbara Banner MD |
Space occupying disease is especially poignant in the brain within the unforgiving non pliable nature of the skull. Thus any new growth in the brain, benign or malignant encroaches on the space of normal structures and inhibits their function. In addition, many structures are closely positioned and concentrated in a small space. Thus impingement on functions in the body can occur if the new growth is in a critical location.
In the following example, a metastasis from a renal cell carcinoma occupies space, but it also causes space occupying edema which causes the shift of other structures.
|
Renal Cell Carcinoma Metastasis with Edema
|
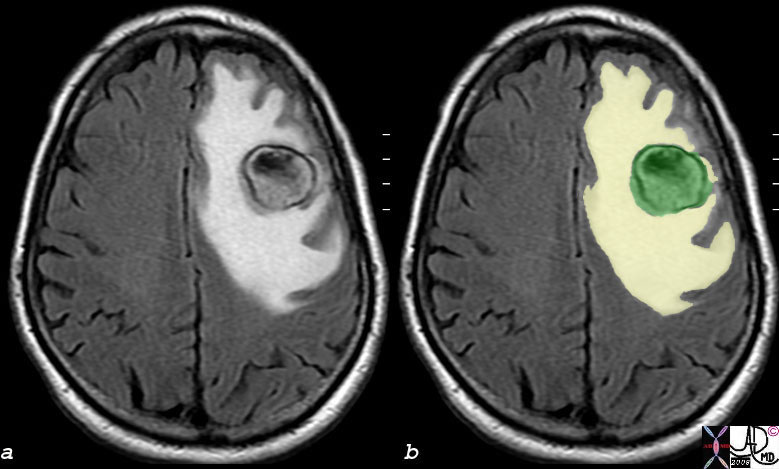
| In this MRI image of the brain there is a metastatic nodule (green) that measures just over 2cms, but it has created a ring of edema which is causing mass effect by space occupation by a volume that is at least 3 times its size. (yellow). This has resulted in subtle midline shift.
77300c bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008 |
|
Renal Cell Carcinoma Metastasis with Edema
|
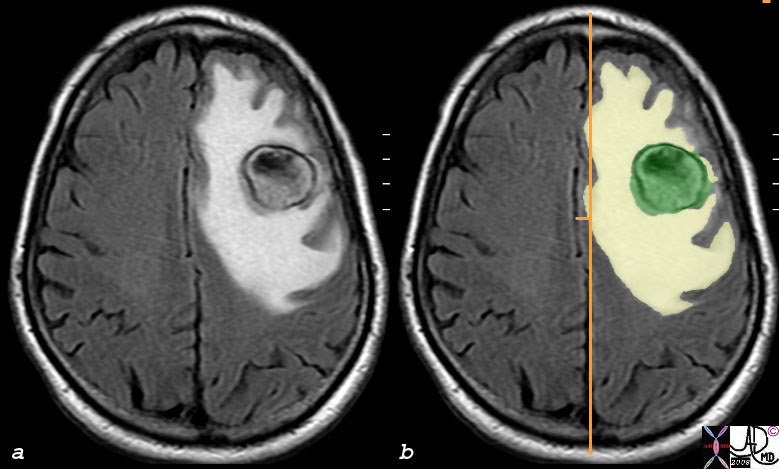
| The long orange line from front to back of the brain represents the middle and the small horizontal orange line shows midline shift of about 4mm. In this instance steroids would help reduce the edema and would help limit the pressure caused by the edema.
77300c01 bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008 |
|
Breast Cancer Invading the Skin Chest Wall and Heart
|
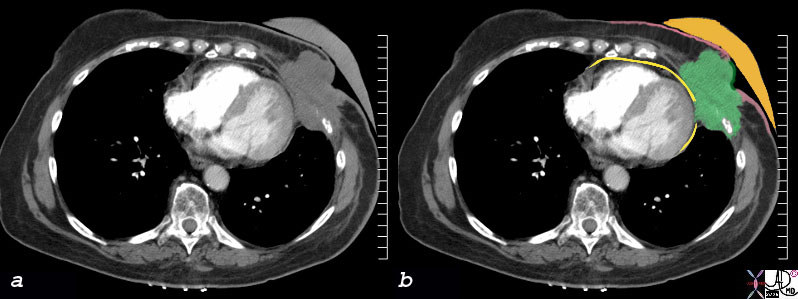
| In this CT scan a patient with breast carcinoma is exemplified in image (a) with color overlays of the CT scan in b. The patient already has had a mastectomy for cancer and the prosthesis (orange) overlies the mastectomy site. A recurrence of the cancer has occurred (green) and it has invaded the skin and is exposed on the outside between the involved skin (pink )which is thickened either due to radiation and or the recurrent cancer. The break in the skin (green exposed through the pink) represents an ulcerating mass. The tumor also invades through the chest wall and has started to erode the pericardium (yellow).
78387c breast skin heart pericardium invasion space occupation prosthesis CTscan Courtesy Ashley Davidoff MD |

Two Ulcerating Malignant Nodules in a Surgical Breast Specimen
|
| In this surgical specimen of a mastectomy, two malignant ulcerating nodules have grown through the skin of the breast. The skin is the flesh colored bruised area and the two fungating nodules have grown through onto the surface.
13526b04 skin + fx ulcer ulceration dx carcinoma complicated by skin invasion grosspathology Courtesy Frank Reale MD |
Cellular Changes
At a cellular level there are a number of characteristic features that define malignant cells;
The structural changes predominantly affect the nucleus. In cancer, the nucleus contains an excess of DNA and this results in a variety of morphological changes.
The nuclii display a variation in size and shape and this is called pleomorphism. The pleomorphism also affects the cells as a whole. Sometimes this implies that the cells are larger than normal and sometimes the cells are smaller.
Although the cell or nucleus may become larger or smaller the ratio of the nucleus to the cytoplasm usually increases as a characteristic feature. The normal size ratio of nucleus to cytoplasm is 1:4 or even 1:6. In cancer the ratio increases to close to 1:1. The nucleus also displays variations in shape as well as hyperchromicity meaning that is darker than normal. Coarse clumping of the chromatin also occurs and the nucleoli become prominent and enlarged.
Atypical and bizarre mitotic figures may be present and the cells lose their polarity meaning that the orientation is heterogeneous.
Functional Changes
The function of any organ or cell is to receive process and export a product that assists the organism as a whole. Cancer will affect local function as well as systemic function.
The local dysfunction will depend on the organ involved. Thus in the brain, depending on location, primary or metastatic cancer may affect the sensory, cognitive, or motor function. Cancer in a tubular system such as a bronchogenic carcinoma may cause lung collapse leading inability of the affected segment or lobe to exchange gas. A primary carcinoma of the head of the pancreas will obstruct the bile duct causing obstructive jaundice. Colon carcinoma often grows as an apple core lesion as described above, and will eventually cause obstruction of the colon.
The systemic changes are often more profound. Fatigue for example is a common symptom, defined as “persistent, subjective sense of tiredness related to cancer”. Often it signifies a recurrence of disease. Fatigue may seriously impair a patient’s ability to perform day to day activities.
There are associated metabolic changes the most common being hypercalcemia and hyponatremia.
Hypercalcemia occurs in 10-20% of patients with cancer, and is caused by absorption of calcium from the bones, as well as a decreased ability of the kidneys to excrete the calcium.
The cause may be due to hormones secreted by the primary tumor or due to metastases to bone. The most common malignancies associated with hypercalcemia are breast and lung, but it also occurs in patients with head and neck cancer, renal cell carcinoma and multiple myeloma. Patients confined to bed also can present hypercalcemia due to bone resorbtion.
The symptoms vary in each patient and the level of calcium does not correlate with the severity of symptoms. Tiredness, malaise, anorexia, increased urination, thirst, nausea, and vomiting are some of the representative symptoms.
Hyponatremia in cancer patients is usually hypovolemic, and hypotonic, most commonly caused by SIADH (syndrome of inappropriate secretion of antidiuretic hormone), chemotherapeutic agents such as vincristine, cisplatin, narcotic analgesics, diarrhea vomiting or bleeding. Symptoms are diverse and include difficulty with concentration, headache confusion, lethargy, personality changes, anorexia, nausea and vomiting. (Harrison’s Manual of Oncology)
Cachexia : The progressive deterioration in nutritional status frequently seen in cancer patients is often referred to as cancer cachexia. Unlike starvation, in which fat stores from adipose are depleted and protein is spared from skeletal muscle, neither fat nor protein is spared in cachexia. Cachexia affects nearly half of cancer patients, causing the clinical manifestations of anorexia, muscle wasting, weight loss, early satiety, fatigue, and impaired immune response. According to clinical studies, increasing caloric intake does not necessarily reverse cachexia. The processappears to be mediated by circulating catabolic factors, either secreted by the tumor alone or in concert with host-derived factors, such as tumor necrosis factor- (TNF- ), interleukins (IL-1 and IL-6), interferon (IFN-y), and leukemia inhibitory factor (LIF).14
Complications
Metastatic disease remains the most common complication in patients with malignancy, and deposits can be found in any part of the body but most frequently are found in the bone, liver, lungs and brain.
Metastases to cortical bone:
The bones most frequently involved by metastasis are femur; spine, ribs and pelvis. Tumors destroy the bone by primarily two processes, direct destruction of bone by tumor cells or stimulating osteoclastic activity of the bone. Bone health is determined by a balance of bone forming osteoblastic cells and bone destroying osteoclastic cells. The cancers secrete cytokines that increase the osteoclastic activity and inhibit the osteoblastic activity. Bone metastasis may present with severe pain and may also cause pathological fracture.


Pathological fracture – Lung Cancer with Metastasis to the Femur
|
| cThis combination represents a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) in this patient with COPD. A metastatic lesion to the right femur is complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD. 32202c code lung cancer carrcinoma squamous cell carcinoma malignant metastases metastasis bone pathological fracture CXR CTscan grosspathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved |
Liver Metastasis:
Liver is a common site for metastasis. Liver metastases are usually two types : Nodular : most common , Diffuse: less common and cause by cancer such as lymphoma, small cell lung cancer and breast cancer.
Liver metastasis may present with right upper quadrant pain , jaundice, nausea, anorexia, weight loss and hepatomegaly.
|
Diffuse Metastatic Infiltration in the Right Lobe
|
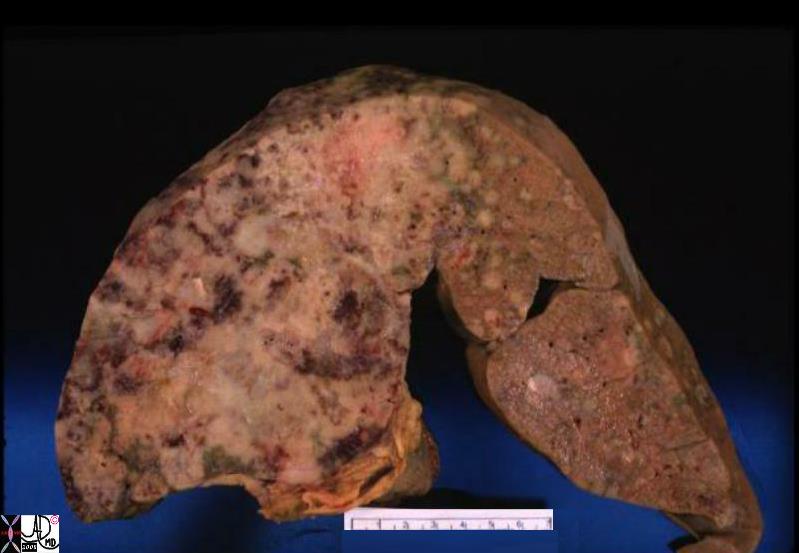
| This gross specimen of the liver obtained from a post mortem was from a patient who had metastatic liver disease from adenocarcinoma of the pancreas. There are both nodular components and diffuse infiltrative components of metastatic disease. The right lobe is almost completely replaced by infiltrative disease while the left lobe is only mildly affected with discrete nodules.
code liver grosspathology mets metatstatic disease metastases metastasis space occupation Courtesy Ashley Davidoff MD copyright 2009 allrights reserved 02692b.8s |
|
Diffuse Infiltration
|
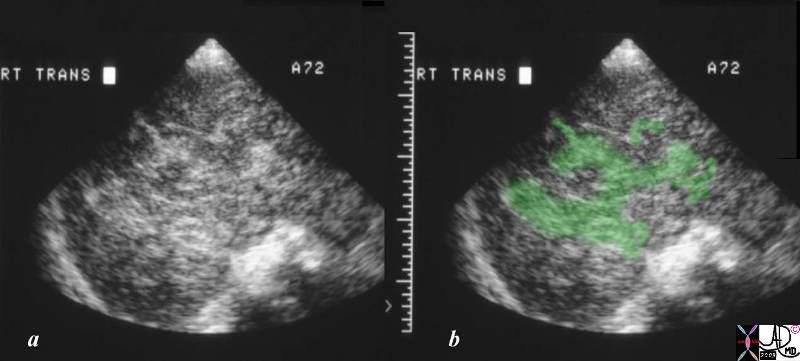
| The ultrasound of the liver is from a 72 year old patient with metastatic breast carcinoma. There is a region (overlaid in green ) that is hyperechoic and diffusely infiltrating without clear nor rounded borders. No obvious mass or nodule can be defined. This finding represents the less common infiltrating metastatic pattern, characteristically, but not exclusively, observed in patients with breast carcinoma.
code liver cancer malignancy malignant carcinoma metastasis infiltrating infiltrative US USscan ultrasound Courtsy Ashley DAvidoff MD copyright 2009 all rights reserved 24012c01.8s |
Lung Metastasis:
Lung metastasis may be nodular, or pleural based. Nodular metastasis may be solitary or multiple. Pleural metastasis may often present either as pleural effusion which may be recurrent and require obliteration of pleural space with sclerosing agents called as pleurodesis.
Lung metastasis may present with dyspnea, cough, wheezing hemoptysis and superior vena cava syndrome.
Skin Metastasis:
Skin may be common a site for solid tumor metastasis. Common malignancies that metastasize to skin are lung cancer, colon cancer, melanoma , and renal cell carcinoma. Metastases to skin may sometimes be delayed by many years following surgery for the primary tumor.
Neurological metastasis;
Many cancers may metastasize to brain, spinal cord and peripheral nervous system. Autopsy series have shown that 25 % who die of cancer have metastasis to brain. Lung cancer is the most common cancer to metastasize to brain. Metastases may present with global signs such as headache, mental status changes in 50 % of the patients. Focal signs include hemi paresis, visual field defects and aphasia. Seizure can occur in up to 20 % of the patients. A CT scan with contrast or a MRI are the best imaging modalities.
Meningeal metastasis: About 8 % of the patients may present with metastasis to leptominges. The spread to meninges is usually hematogenous. The presentation usually depends on the site of involvement.
Cerebral: Symptoms such as headache, ataxia, mental status changes and seizures.
Spinal: Usually presents with back pain, radicular pain, weakness and numbness of arms or legs.
Cranial nerve involvement: May present with facial weakness, numbness, diplopia and visual loss.
Hydrocephalus: May present with signs of increased intracranial pressure such as headache, ataxia, decreased level of consciousness and urinary incontinence.
Intestinal: Though uncommon may present with obstruction, perforation or bleeding.
Adrenal: Adrenal metastases are not uncommon. The most common tumor to metastasize to adrenal is lung carcinoma. The patient may present with catastrophic hemorrhage or adrenal insufficiency.
|
Bilateral Adrenal Metastases
|
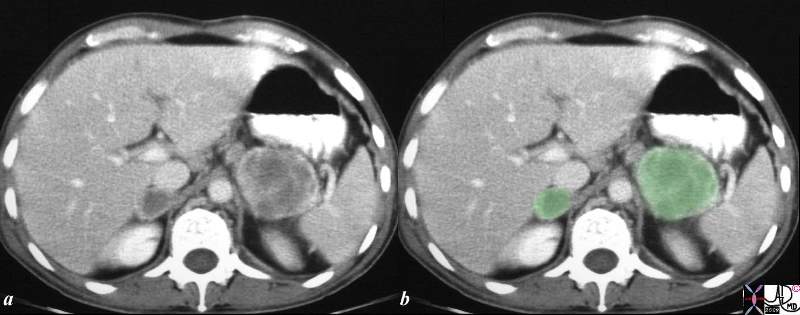
| The CTscan of the upper abdomen is from a patient with known lung carcinoma. The size, bilaterality and the heterogeneous appearance, particularly on the right are reminiscent of metastatic disease. In image b the adrenal tumors have been overlaid in green.
25767c01.8s Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasn malignant metastasis metastases primary lung imaging radiology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved |
Electrolyte abnormalities: Hypercalcemia: hypercalcemia is common complication of malignancy. Mechanisms of hypercalcemia are different in different cancers.
Hyponatremia : Hyponatremia is a common problem usually associated with lung carcinoma.
Endocrine abnormality : Tumors may produce hormones which can cause or exacerbate endocrine disorder such as hypercortisolism.
Tumor lysis syndrome:
Tumor lysis syndrome can occur in a rapidly growing tumor. Rapidly dividing cells undergo lysis releasing large amount of electrolytes such as high potassium , high phosphate that can cause cardiac rhythm abnormality. The high amount of uric acid that is released can precipitate in the kidneys causing acute renal failure. It is a life threatening emergency requiring immediate management.
Hematological :
Thrombosis : Cancer is a risk factor for unproved venous thrombosis
DIC : Many cancer can present with low grade or overt DIC and may even cause bleeding.
Bleeding disorders: Less common than thrombosis are hemorrhagic complications due to abnormalities such as factor VIII inhibitors.
Natural History
Most cancers develop stepwise over a long period of time with nonmalignant precursor lesions that only slowly evolve toward cancer. With many chemicals and some radiations, as well as some viruses (DNA and some retroviruses), cancer development can be divided into 3 major stages or periods; initiation, promotion and progression. Initiation is frequently associated with a more or less permanent change in the phenotype of a rare target cell, presumably due to a change in base composition in DNA or to gene rearrangements. During promotion, these rare cells expand by proliferation to generate focal proliferations that resemble benign neoplasm. These in turn may undergo either regression to normal appearing tissue or slow evolution to cancer. The prolonged nature of the promotion-progression stages in most tissues and its different outcome indicate that these stages are vulnerable sites for the development of ways to prevent the progression to cancer.
The histopathological appearance can help in differentiate fast growing tumors from slow growing. Well differentiated tumors are usually slow growing and anaplastic tumors are aggressive.
Clinical Approach
Assessment of cancer patient has to be comprehensive and detailed. It is not only an opportunity to gather details about the disease but also about the patient themselves. It is also important to address concerns of the patient’s family. This knowledge is very important as this will be crucial in decision making. The opportunity to delve in to patient’ support system is critical since a significant amount of support by the family is required in the treatment process. Nutritional assessment is vital component of initial assessment as starting potentially serious treatment in a patient with poor nutrition status can lead to significant morbidity as well as mortality.
History / Symptoms
Patient Background
A face-to-face caregiver to patient history is strongly encouraged and important in both general rapport as well as diagnosis. Never should one rely only on word of mouth, or medical records as sole tools for taking a history from any patient. Patience and genuine personal interaction is a defining characteristic of medicine in general. In oncology specifically, it is an opportunity to set forth a relationship between medical profession and the patient. And while patient autonomy is paramount, it may often be necessary to have a family member visit as often during the course of treatment. Discussion will be necessary between the patient and family to facilitate treatment decisions. Bringing a companion should always be the patient’s initiative but all patients should be given the opportunity to be interviewed and examined alone, even when accompanied to the office.6
The initial baseline history, if not immediately obvious, should include information on baseline functional status (ambulatory, wheelchair bound, bed-bound) in order to assess severity of disease and further management. Assessment of the exercise tolerance and basic ADLs (activities of daily living: feeding, hygiene, dressing, continence, transferring, bathing and mobility) and IADLs (independent activities of daily living: shopping, cooking, cleaning, managing money, telephoning, laundry, and travel) have been shown to be important tools in the prognosis of the disease.
There should always be enough time to allow for the patient to reflect and ask questions. The review of systems should be focused however the following issues should always be addressed.
Medications:
Due to risk of dangerous drug-drug interactions, potential overuse of over-the-counter drugs, misuse of herbal supplements, and simple accumulation of medication that may no longer be indicated, a careful drug history should be obtained. A comprehensive medication history can give clues in diagnoses of common problems, such as changes in mental status changes, acute kidney injury, and liver function abnormalities, among others. Assessment of the organization of a patient’s medications, often best obtained by asking the patient to bring all bottles and/or pillboxes, will provide a window into the understanding and compliance that a patient demonstrates.
Social History:
Social history should include detailed information on the patient’s living situation and, it is also important to determine if a patient is a caregiver him/herself, which can place the patient at higher risk. In that context, social supports and potentials for social interactions should be identified, as they are a major factor in both prevention of and recovery from disease. In addition, it should never be assumed that an older patient does not drink alcohol or use recreational drugs. These topics should not be avoided due to health provider discomfort.
Nutritional History:
The caregiver should emphasize good nutrition which is crucial to ensure a favorable patient outcome. Patients’ dietary patterns are a prime concern in patient with chronic disease of any type
Family History:
Family history is crucial in an oncology patient as it may signify a genetic predisposition. If it is suspected then family members need to undergo genetic testing to determine their individual risks.
Systemic Symptoms
One of the most common systemic manifestations of cancer is weight loss, and is considered the most common paraneoplastic manifestation of cancer.
Paraneoplastic syndromes are features in patients that cannot be explained on the basis of structural or functional characteristics directly related to the malignancy. Mediators produced by the tumor have effects often the body remote from the physical site of the tumor. The weight loss is thought to be caused by tumor necrosis factor. The underlying cause is anorexia which results in decrease intake of food. An unexplained weight loss of 10 pounds or more may be the first sign of cancer. This happens most often with cancers of the pancreas, stomach, esophagus, or lung. On the other hand the absence of weight loss does not imply the absence of cancer.
Fever is another common occurrence in cancer and is also a paraneoplastic phenomenon. It may or may not be associated with night sweats. It may be caused by the cytokines released by the tumor itself or secondary to immunosuppression associated fevers. Fever is very common with cancer, but it more often happens in patients with metastases. Cancer may cause fever by itself or it can be from suppression immune system by chemotherapy drugs. For cancer such as leukemia and lymphoma fever may the first sign of these entities.
Night sweats: Night sweats are common with many cancers however more commonly are associated with lymphoma.
Fatigue is extreme tiredness that does not get better with rest. It may be an important symptom as cancer grows. It may also be caused by anemia and chemotherapy.
Anemia is a common occurrence either due to myelosuppresion secondary to the cancer or resulting from hemorrhage. Anemia is also an important complication of chemotherapy.
Virtually every cancer patient has pain. It can affect quality of life and can be demoralizing to the patient. The etiology of pain may be visceral, somatic or neuropathic. Unfortunately pain in the cancer population still is difficult to control. It may be caused by bony metastases. Headache is a common symptom associated with CNS tumors and metastasis.
As stated above 10-20% of patients have hypercalcemia and hyponatremia is also a problem. These both have symptoms that include many of those mentioned above. Often they are correctable and so it is relevant to keep them in mind.
Cancer patients may have myriad neurological presentations ranging from peripheral neuropathy, paraplegia from a spinal lesion to focal deficit and seizures.
History Related to the Primary Site
Focused history related to the primary organ is an obvious component of the clinical concern. In the patient with suspected brain tumor, either primary or metastatic, questions about sensory cognitive or motor function are relevant. Dysphagia is a non specific sign, but may be associated with esophageal cancer. Early satiety is associated with gastric cancer. Change in bowel habits, such as new constipation, pencil thin stools or alternating constipation and diarrhea, although non specific sometimes reflects malignant disease in the colon.
Ulcers, white patches, and black patches
Non healing ulcer in any mucosal site may be cancerous. Skin cancers may bleed and look like sores that do not heal. Sores on the penis or vagina may either be signs of infection or an early cancer, and should not be ignored. Any change in appearance of a wart mole or freckle may signify a malignant transformation.
White patches inside the mouth and white spots on the tongue may be leukoplakia. Leukoplakia is a pre-cancerous area that is caused by ongoing irritation. It is often caused by smoking or any other tobacco habit.
Blood
Blood in the phlegm (hemoptysis) may be a sign of lung cancer. Blood in the stool (or a dark or black stool) could be a sign of colon or rectal cancer. Cancer of the cervix or the endometrium (lining of the uterus) can cause unusual vaginal bleeding. Blood in the urine may be a sign of bladder or kidney cancer. A bloody discharge from the nipple may be a sign of breast cancer.
Thickening or lump in the breast or other parts of the body
Many cancers can be felt through the skin. These cancers occur mostly in the breast, testicle, lymph nodes (glands), and the soft tissues of the body. A lump or thickening may be an early or late sign of cancer and should be reported to a doctor, especially if you’ve just found it or notice it has grown in size.
Persistent cough or hoarseness;
A cough that does not go away may be a sign of lung cancer. Hoarseness can be a sign of cancer of the larynx (or thyroid.
Signs
As the patient sits in the office, the general demeanor and psychological well being of the patient can be recognized. For example the hunched over, quiet patient who has lost the twinkle in the eyes may be features of depression. Depression accompanies malignancy in general but also accompanies pancreatic cancer specifically. Loss of skin turgor suggests dehydration and the lips should be glanced at to confirm this finding.
As the hands as are examined, the nail beds may reflect the presence of anemia. Clubbing is seen in small cell cancer of the lung among other suppurative and malignant conditions.
Skin changes may due to cancer itself such as with skin cancer or a result of cancers from other organ :
- darker looking skin (hyperpigmentation) is associated with pancreatic cancers
- yellowish skin and eyes (jaundice) associated with pancreatic cancer, Cancer of gall bladder or liver metastasis.
- reddened skin (erythema) may be caused by skin infiltration of cells such as in leukemia
- itching : may be associated with lymphoma or with gall bladder obstruction
- acanthosis nigricans is a darkening of the skin in the axilla or neck that is associated with gastric cancer
- icthyosis, is characterized by dry hyperkeratosis skin that resembles fish scales and is associated with lymphoma
- dermatomyositis is an autoimmune disease that is sometimes a paraneoplastic syndrome in patients with lung cancer. The entity is characterized by a skin rash and symmetric proximal muscle weakness sometimes accompanied by pain. Interestingly when the primary lesion is removed the dermatomyositis resolves.
As the axilla is examined enlarged lymph nodes should be sought both in the axilla as well as the supraclavicular, cervical and occipital regions. Examination of the cranial nerves is important in all cancers, particularly those with a propensity to brain metastases. This relates to the examination of the sensory and motor function as well. Abnormal cerebellar examination may relate to either metastatic disease or due to paraneoplastic syndrome in patients with lung cancer.
Examination of the lungs and heart is non specific in the cancer patient, but bone pain in the examination of the chest and back should be sought.
The liver is a common site for metastatic disease for gastrointestinal malignancies and enlargement and tenderness suggests metastatic disease. Ascites is a common finding in patients with ovarian malignancy. In the elderly patient with anemia the right colon often harbors an occult malignancy. The distinction between stool and a mass in the right lower quadrant at a single examination may be difficult, but a mass will not change on a subsequent examination whereas stool will probably change in configuration, size, or consistency.
Rectal examination should always be associated with examination of the prostate, and Guiac examination for blood should be routine. Vaginal examination with attention to the adnexa and cul de sac is imperative.
Diagnosis:
The diagnosis most commonly is suspected based on the clinical presentation or as an incidental finding on imaging.
The initial laboratory data should include a complete hematological as well as blood chemistry profile. Certain cancers are associated with cancer markers such as PSA for prostate cancer, CEA for colon cancer and CA125 for ovarian cancer.
Aim of management is to confirm diagnosis and ascertain the stage of disease.
Radiological studies such as ultrasound, CT scan and MRI help in diagnosis, staging and restaging after treatment.
Clinical Strategies
The clinical strategies in a patient with cancer are aimed at prompt diagnosis and staging, formulating a treatment plan and ensure an appropriate post follow up appointment.
Initial visits should be geared toward getting a good history and comprehensive exam. The diagnosis once suspected should be confirmed with prompt histopathological diagnosis with the biopsy. A prompt work up should be done to ascertain the staging of disease.
On completion of work up, it is important to sit down with patient as well as, any family member that patient wishes to be part of discussion. This opportunity should be utilized to explain the diagnosis, extent of the disease, prognosis and treatment options. As far as possible medical jargon is to be avoided and patients should be given every opportunity to ask questions. Diagnosis of cancer is a life altering event for patient and their families and the patient may not be able to handle all the information. Patients should be given the opportunity to participate in a clinical trial.
Treatment of the cancer patient is usually a multidisciplinary effort including surgeons, medical oncologist and radiation oncologist. Oftentimes multidisciplinary conferences may be required before a treatment plan is presented to the patient. During treatment it is important that other issues such as nutrition and psychosocial issues are also addressed.
After treatment every effort should be made to restage the disease. The findings should be then discussed with the patient. Based on restaging patient may be classified in to complete remission, partial remission, stable disease or chemo resistant disease. It is possible that some patients will require additional treatment.
Patients who are in remission will require frequent follow up with blood work and imaging.
Lab Tests
A variety of laboratory anomalies can be seen in the cancer patient, most of which are noted upon hospitalization, when
A value which might appear normal may not be and vice versa. A common example would be when an elderly patient would seem to have a normal or even low white blood cell count in response to pneumonia. A sample summary of lab changes in cancer appears in the following table.
|
Lab Value
|
|
|
hemoglobin
|
cancer patients are usually anemic but renal cancer may cause polycythemia
|
|
WBC and platelets
|
May be reduced by cancer
|
|
Insulin blood sugar
|
ACTH producing tumor may cause hyperglycemia
|
|
|
|
|
DHEA
|
May be increased with some adrenal tumors
|
|
Testosterone
|
May be increased with sex cord tumors
|
|
T3
|
May be increased due to thyroid
|
|
Estrogen & Progesterone
|
May be increased with ovarian cancer
|
|
Potassium
|
May be increased with tumor lysis syndrome
|
|
Calcium
|
Many cancers can cause hypercalcemia
|
|
PaO2
|
Hypoxia may be associated with lung cancers
|
|
GFR
|
Cancer can cause renal failure either by tumor lysis syndrome or abnormal protein
|
|
Calcium
|
Hypercalcemia is a common electrolyte abnormality in cancer patients.
|
|
CEA
|
Is high in colon cancer
|
|
Ca 125
|
Is associated with ovarian cancer
|
|
PSA
|
Increased with prostate cancer
|
|
Cell mediated immunity
|
May be reduced in patient with lymphoma
|
|
|
|
Other considerations:
Albumin correlates with mortality and reflects the patient’s nutritional status over the prior 3 months. (Swensen) Prealbumin reflects nutritional status over the past 20 days. A low pre-albumin as well as a lymphocyte count may reflect a poor nutritional status.
Venous access issues:
As a rule, central venous catheters may be a necessity in oncology patients as extravasation of certain drugs may threaten the loss of limb. In addition chemotherapy may make IV access difficult over a period of time. Therefore indwelling venous catheters are very important. A nurse should review the importance of the device, advantages, risks, and potential complications.
Imaging
Imaging is an important tool in oncology patients. It plays an important role in diagnosis, staging and restaging after treatment. It may play an important role in diagnosis of multiple complications that may occur during treatment.
Special concerns about the safety and needs of the oncology patient are outlined below, followed by a discussion on the modalities utilized.
Instruction before Coming to the Office or Hospital:
Patients should be instructed to wear loose comfortable clothing when coming for any exam or radiological test. In addition, a patient should be aware that it is important to have all hearing aid devices readily in place, if appropriate.
Registration process:
The patient should be made aware that certain tests use IV dyes that may cause an allergic reaction and the patient should make any allergies clear and known from the outset prior to or during registration. The intravenous contrast used for CT scan causes transient vasodilatation and a sensation of warmth may be felt in parts of the body. Each patient is different, but some experience an uncomfortable sensation of unreal urinary incontinence. Others may have transient nausea or vomiting. Allergic reactions have become less common with new agents and range from hives and swelling to anaphylaxis and life threatening disease. The incidence of life threatening reaction is not precise but older literature suggests between 1 per 50,000 patients.
The special approach to the patient in the imaging department:
Every effort should be made to keep the patient comfortable and calm while waiting for tests to be done in the radiology department. Whether ambulatory in the waiting room or on the stretcher, more often than not, there is associated anxiety with undergoing radiologic tests for any patients. Oncology patients may be more prone to anxiety surrounding potential results and long waiting times. In addition, all attempts at fall prevention are crucial, whether that means an obstacle free waiting room, raised guardrails on the hospital gurney or assistance from the technologist to transfer to the examination table.
Special equipment:
Depending on the needs of the patient, appropriate equipment should be available for transport and transfer of patients in the radiology department. Wheelchairs should be readily accessible for patients who may have difficulty walking distances from the facility’s entrance to the imaging department, along with staff to transport the patient. Comfortable gurneys and/or hospital beds suffice for inpatients, yet staff trained in proper transfer techniques is crucial to prevent both patient and staff injury. In that regard, exam tables need be made comfortable, with appropriate supervision and/or securing devices for maximal patient safety.
Bathroom Facilities:
Safety bars alongside commodes are essential. Ample space should for wheelchair entrance and storage, and low sinks for wheelchair bound patients to facilitate hand washing are necessary.
Contrast studies:
When a patient is required to receive IV contrast for any study, staff at every level of care should inquire about allergies to IV dye as well as pursue relevant past medical history regarding risk of contrast induced kidney injury (nephropathy), including but not limited to diabetes, hypertension, and chronic kidney disease.
MRI:
Inquiries need be made regarding pacemakers in patients, although many MRI’s and pacemakers are becoming compatible with advancing technology. Recent stents or other procedures requiring metal staples and the like need be addressed, as it is best to avoid MRI in a short time window after such procedures.
In any study requiring prolonged supine positioning, light sedation/anxiolytics may be considered, yet this should be administered, if at all, in the context of the patient’s overall medical condition. If a patient is ambulatory, any patient given the above medication classes should be asked to have an accompanying family member or friend to assist the patient in and out of a vehicle and home. Any sedation and/or anxiolytics used raises the fall risk of the elderly or weak patient and should be avoided if at all possible. In the hospitalized patient, slightly more liberality in this regard may be appropriate, yet utmost attention to changes in mental status need be made.
Modalities
It is important to remember that there are multiple modalities that may be utilized in a specific oncology patient which include X-rays, CT Scans, Ultrasounds, MRI and PET scans. To ascertain which modalities may be best may require discussions between a clinician and radiologists.
Radiology may also play in therapeutic procedures
Ultrasound
Ultrasound in radiology, or diagnostic sonography, is the imaging of parts of the body using sound energy. Ultrasound refers to sound waves above the human hearing range (>20kHz). It is commonly used in the patients with suspected breast cancer when a lesion identified on a mammogram requires further characterization. It is also used in the examination of the liver in patients with primary and metastatic liver disease, but because it is operator dependant, and follow up studies are often performed in a slightly different way, strict and accurate comparison is not usual. Ultrasound is one of the modalities of choice to distinguish between a cystic and solid lesion in the kidney, and is often the study that identifies unsuspected renal cell carcinoma. Evaluation of involvement of the renal vein, IVC, and right atrium by ultrasound is accurate. Ultrasound is also the study of choice when ovarian or testicular cancer is suspected.
|
Cyst – (right) and Solid Cancer in the Kidney (left)
|
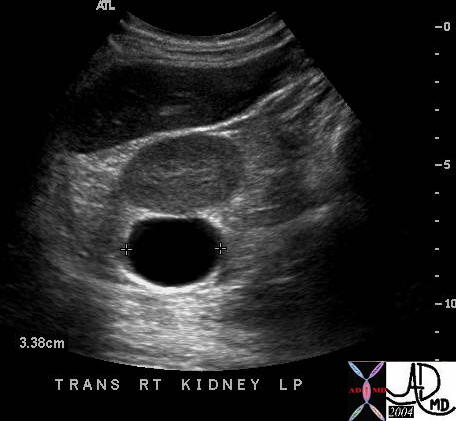
| This ultrasound scan demonstrates the classical features of a cyst with absence of internal echoes, back wall enhancement and through transmission of sound waves. This cyst was exophytic off the right kidney. The second image shows a solid mass off the inferior aspect of the right kidney with internal echoes. The cyst is simple and requires no further diagnostic attention, while the solid mass requires surgical intervention.
Courtesy Ashley DAvidoff MD 39051b 39052b |
It is a focused examination and does not have the same global perspective as CT scanning. Therefore once a diagnosis of cancer is suspected on ultrasound a CTscan, or CT PET scan is usual to assess the extent of the disease.
Ultrasound is often used for image guided procedures such as needle biopsy, thoracentesis, and paracentesis. The latter may be indicated for diagnostic or therapeutic needs.
There are neither real dangers nor disadvantages of ultrasound. For abdominal examinations the patient is asked to fast for 4 hours, because resulting increased peristalsis and gas prevents the sound waves from penetrating and hence limits visualization of deeper structures. The fasting state is necessary to enable the gallbladder to be distended and evaluable. Food causes cholecystokinin to be released and the gallbladder to be contracted.
Computed Tomography
CT is an imaging technique that utilizes the attenuation of an X-ray beam through the body to create tomographic images. Recent advances in CT technology allows for rapid, volumetric imaging and sophisticated data manipulation and image processing.
Computed tomography is the workhorse of oncologic imaging. One cannot imagine a oncological world without this modality, and advances in oncology have been spurred by advantages in imaging and specifically CT scanning because it has provided more accurate staging resulting in prudent therapy, and also objective evaluation of efficacy of therapy.
Advantages include the fact that it is less operator dependant, shows consistency from scan to scan, is rapid, non invasive, accurate, has wide availability, and provides a global perspective of the part of the body being imaged. Ionizing radiation, intravenous contrast, and the relative cost of the exam are the main disadvantages. It lacks the ability of ultrasound to accurately characterize simple cysts, and lacks the superior abilities of MRI to optimally characterize disease.
It is used in the oncological realm in the initial diagnostic workup in the patient suspected of having lung cancer, metastatic liver disease, renal cell carcinoma, pancreatic carcinoma, peritoneal carcinomatosis. It is routinely used in the staging of malignancies in the chest, abdomen, and pelvis, and in the follow up of these diseases following treatment.
CT guided biopsies of lung, liver, pancreatic, peritoneal, retroperitoneal lesions are readily accomplished and often is the only way in which a diagnosis can be made short of surgery.
|

Lung Biopsy
|
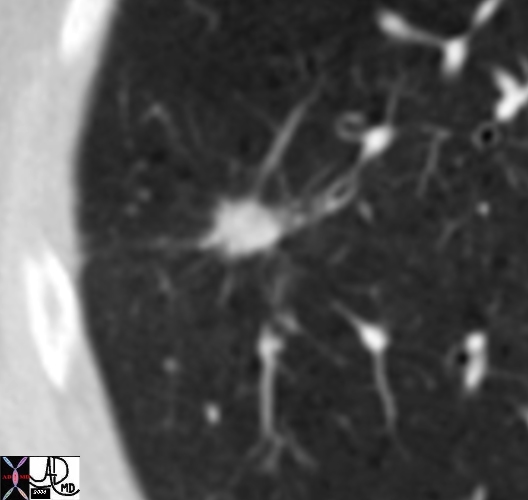
| The CT is from an 81 year old man with remote history of smoking who presents with an asymtomatic lung mass. The lesion was PET positive, without nodal activitiy suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
85221c01.8s Courtesy Ashley Davidoff MD all rights reserved |
Therapeutic procedures such as thoracentesis and paracentesis are best performed by ultrasound, but if difficult these can be performed under CT guidance. Radiofrequency ablation of liver, lung and kidney lesions are best performed under CT guidance since consistent accuracy, and uniform visualization of the tip of the transducers is essential prior to the treatment.
PET -CT is a new combination diagnostic modality that has revolutionized oncologic imaging in that it uses the power of PET scan to identify hypermetabolic regions in the body, but it lacks spatial resolution, so that it may be difficult to localize the exact tissue of origin. CT is combined with the PET scan, and performed at the same time, enabling the accurate localization of the diseased area.
MRI
MRI is an imaging technique that utilizes a strong magnetic field to align protons in the body. Specific pulse sequences produced by a radiofrequency electromagnetic pulse reorient the protons. When the RF pulse is turned off, the spinning protons relax back in a tissue specific manner (relaxation time) to their equilibrium state, which is characteristic and unique to the tissue. This data is detected, recorded, and converted into a format that is reflected as an image.
The advantages of MRI are that it does not involve ionizing radiation and it is a safe non invasive procedure.
It does require the patient to lie quite and still for prolonged periods (30-45 minutes), and is currently contraindicated in patients who have pacemakers, and other metal implants such as cochlear implants.
The contrast resolution of MRI is superior to CT and is made possible by a variety of pulse sequences (5-20 per study) that enable the contrast differences between two tissues to be enhanced. Contrast agents are usually used in oncological imaging, unless contraindicated by renal compromise) and further enable the distinction and characterization of malignant tissue.
Malignant tissue in general has higher water content and hence greater proton density than most tissues. The difference in proton density will allow tumor to be differentiated from normal tissues. It is particularly useful in imaging tumors of the brain and soft tissues. It is the study of choice when characterization of liver tumors is needed. Impingement on the spinal cord by metastases to the spine is best diagnosed by MRI. Of recent, contrast enhanced MRI has been used to detect small areas of cancer in the breast that would have previously eluded diagnosis.
|

Anterior and Posterior Commissures
|
| The T1 weighted sagittal image of the midbrain shows a hyperintense lesion in this patient with melanoma. Hyperintensity on T1 is most commonly associated with acute hemorrhage, but is also seen in melanoma.
21731 brain fx mass dx metastasis dx melanoma MRI T1 sagittal Courtesy James Donnelly MD Uploaded RP |
PET scan
Positron Emission Tomography is an imaging technique that utilizes nuclear emission to identify structure, function and disease. The most commonly used tracer is FDG (fluorodeoxyglucose) which is a glucose analog linked to the radioactive isotope fluorine 18 which is a source of positrons. The tracer is injected intravenously and the glucose is attracted to regions of heightened metabolic activity. (brain, kidney malignant and inflammatory tissue). The technology detects pairs of gamma rays emitted by a positron emitting radioisotope. field.
The technique requires that the patient be fasting for 6 hours, with a resultant relatively low blood sugar. Diabetic patients with relatively high blood sugars may be problematic.
Although the sensitivity for malignant disease is high, the specificity is limited because of the non specific uptake in any tissue that is hypermetabolic such as an infectious or inflammatory focus.
However it has been extremely helpful in the diagnostic process in the lymphomas, lung cancer, breast cancer, colorectal cancer, and melanoma.
|

Positive PET scan
|
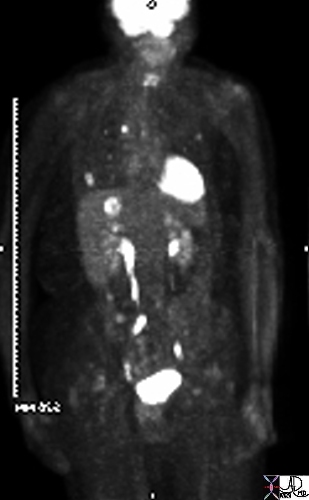
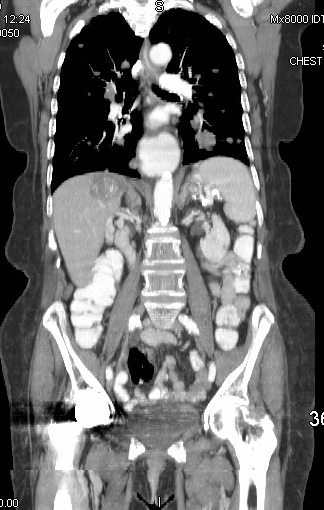
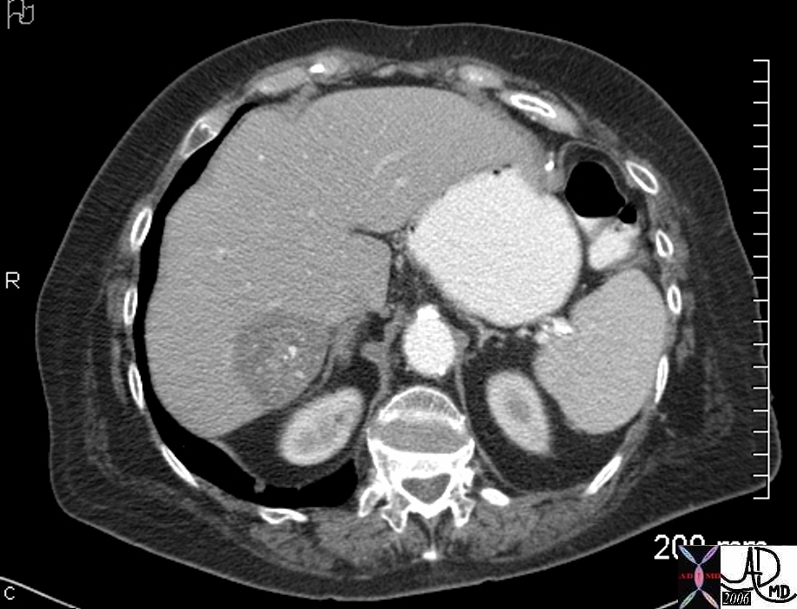
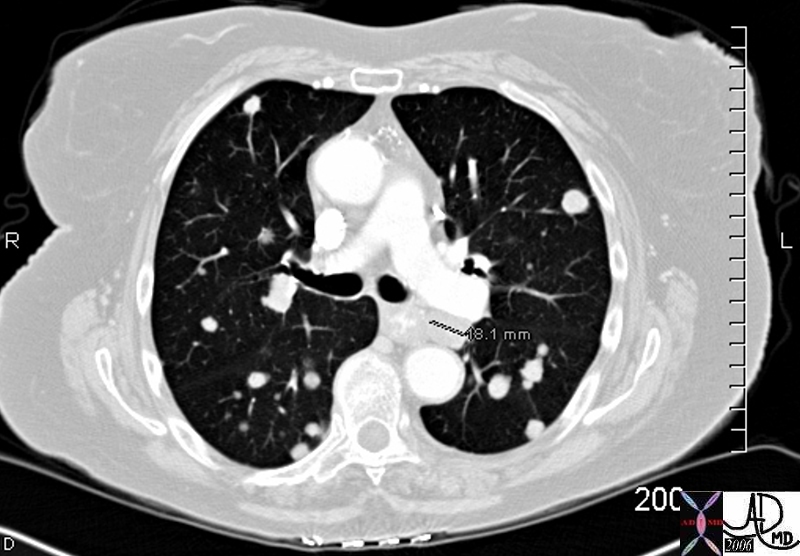
| The CT scan and PET scan are from a patient with both esophageal carcinoma and colon carcinoma that were treated in the past. Follow up CT scan of the chest showed a new nodule in the right upper lobe. (a,b, white arrow) and also showed thickening of the esophagus (red arrow). PET scan showed an isolated hot spot in the right upper lobe and no uptake in the esophagus where recurrence was a possibility based on the thickening. Biopsy confirmed metastatic colon carcinoma.
85224cb01.8s CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved |
It has also been helpful in staging disease. Lymph nodes that would otherwise have been considered by conventional imaging (CT for example) to be uninvolved in a patient with malignancy based on their small size, may prove to be PET positive, and likely to be a metastatic focus. This ability has significantly improved the accuracy of staging and hence the appropriate and prudent therapeutic approaches to a variety of cancers. It has also been used to determine efficacy of treatment.
PET scanning has superb contrast resolution but extremely poor spatial resolution, and hence as an isolated study the anatomic origin of the activity is often difficult to establish. The simultaneous acquisition of a CT scan during image acquisition is extremely helpful to determine the site of origin of the tumor. The CT should not be considered diagnostic since it is performed without contrast, is acquired while the patient may be breathing. It should be seen only as a guide to localizing the tumor and not as a diagnostic study itself.
Findings on Imaging Studies
The word cancer derives from the Greek word “kanker” which means crab. Galen a Roman physician is purported to have coined the term since he noted that the disease had a central rounded appearance reminiscent of the crabs body from which emanated irregular “veins” reminiscent of the crab’s legs.
|
Crab Like?
|
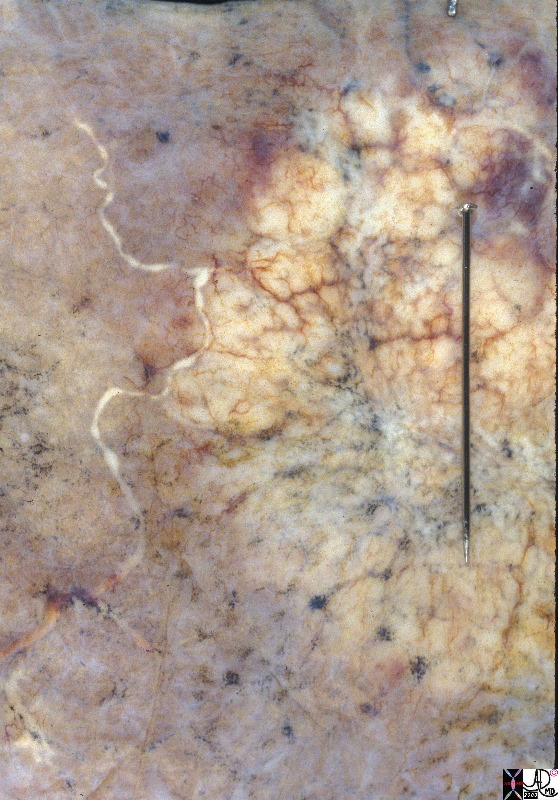
| The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics as seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image to the authors eye has a crab like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
32317.8s Courtesy Ashley Davidoff and Jeffrey Peirce A86-215 32317 copyright 2009 all rights reserved |
The body of the crab is always the nodule or the mass, and the legs may be caused by tumor extending into the surrounding tissue, lymphatics or veins. On the other hand one cannot assume that because the shape of the lesion on imaging is crab like that it is definitely represents a cancerous growth. The suspicion is raised and the patient then requires a biopsy to confirm the diagnosis. Two examples below have both proved to be cancer and have the characteristic crab like shape. Radiologists have preferred the adjective “spiculated” or “stellate” to describe this shape rather than the adjective “crab like”. The reasons for this avoidance are uncertain, but possibly because it is not absolutely pathognomonic for the diagnosis or because “spiculated” or “stellate” lesion is a more accurate description.
|
Spiculated Lung Nodule
|
| The shape of the lung nodule seen on the chest CT in the right upper lobe with radiating spokes or spicules is characteristic a lung carcinoma and was proven to be a primary cancer of the lung. The spicules represent sheets of tumor cells extending into lymphatics or interstitium, or obstructed vessels.
46361 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff |
|
Spiculated Mass in the Right Breast
|
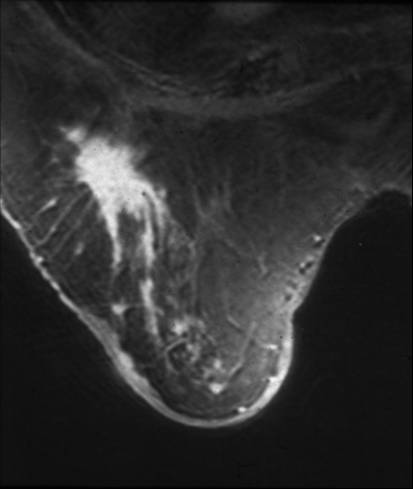
| This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology.
42977 Courtesy Priscilla Slanetz MD breast CASE 27: |
The morphology of a particular cancer depends not only on the disease process itself, but on the tissue and organ from which it arises, the restrictions or freedom with which it is allowed to occupy space, and the pattern of growth that is innate in the biology of a particular malignancy. A more common manifestation of colon cancer for example is growth and spread within in the layer below the inner lining called the submucosa. The initial space occupation occurs in a circumferential manner creating a broad band or belt around the bowel with progressive tightening of the belt, and slowly advancing obstruction. When barium is instilled into the colon the shape created by the band has been termed “apple core” deformity. Based on the shape of the sigmoid colon there is almost no other differential diagnosis but adenocarcinoma of the colon. The narrowed lumen with irregular mucosa with heaped up edges on either end are characteristic of a malignancy.
|
 
Apple Core Lesion in the Sigmoid Colon
|
| The images are from a double contrast barium enema. Contrast and air have been instilled into the rectum and images of the sigmoid colon were taken with fluoroscopic guidance. The first image reveals a narrow lumen, the second shows the apple core deformity (green)and the third has the overlay of where the tumor (light orange is positioned), and reveals how it causes the tight band like constriction of the lumen (green) to result in the apple core deformity described.
00878 00877 Courtesy Ashley Davidoff MD 5star aka applecore |
|

Pathological Specimen of an Apple core Deformity
|
| Portion of left colon with a constricting apple core carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
12313 Courtesy Barbara Banner MD aka applecore |
In general, the findings of tumors on imaging studies are not absolutely diagnostic but rather raise suspicion of malignancy. The diagnosis inevitably is the responsibility of the pathologist and is based on the microscopic appearance, not only for the verification but also in the evaluation of the aggressiveness of the disease.. The role of imaging therefore is to distinguish those findings that raise sufficient suspicion to warrant a more aggressive diagnostic approach such as a biopsy.
There are certain highly suspicious findings throughout the organs of the body that suggest cancer. In the brain, the most common form of malignancy is glioblastoma multiforme, and accounts for about 50% of primary brain tumors. Its appearance on MRI is not specific but becomes more specific if it crosses the midline through the corpus callosum creating the morphological classical “butterfly” glioma – a shape that results from the pattern of spread. Metastatic melanoma to the brain presents with lesion that is bright on a T1 weighted sequence. In a patient with known primary melanoma, this appearance would be almost pathognomonic.
In the colon, size of the lesion has implication. When polyps are less than a 1cms the possibility that they are malignant is less than 5%. As they grow into the 1-2cms range the chances of malignancy are in the 10% range. Once they grow beyond 2cms the chances of malignancy increase to 50%. There are three types of adenomatous polyps; tubular, tubulovillous, and villous. Tubular adenomas are the most common while villous adenoma has the greatest potential to become malignant.
Finding of a pancreatic mass in the head of the pancreas, associated with dilated bile ducts and dilated pancreatic duct (“double duct sign”) is almost pathognomonic.
Hepatocellular carcinoma is characterized by early arterial phase enhancement, fat in the lesion, or venous invasion usually in the setting of cirrhosis.
In the kidney any solid lesion is considered malignant and is surgically removed without a biopsy.
In the ovary a thickened enhancing septation is concerning while in the testicle s a solid lesion is malignant until otherwise proven.
The presence of an FDG avid lesion (“hot”) is also highly suspicious for malignancy, though inflammatory and infectious lesions may also be FDG avid, and the clinical background helps the diagnostic workup.
Strategies
The strategy in the diagnostic workup starts with an informed knowledge by the radiologist that provides a pretest probability or likelihood of cancer. The patient with asbestosis and a history of cigarette smoking has a 90 times increased of malignancy compared to a patient without these risk factors. The patient with a family history of breast cancer or colon cancer is also at risk, and the threshold of the radiologist is lowered when a relevant aberrancy is noted or suspected.
The prevalence of cancer in the general population is also considered in screening programs. Yearly mammograms starting at age of 40, colonoscopy is recommended at age 50, PAP tests for cervical cancer should start about 3 years after beginning of vaginal intercourse, but no later than age 21 years, and PSA is performed annually after the age of 50 years. (American Cancer Society)
The society at large is cancer conscious and there is an understood phobia about the disorder that carries through to radiologists both as a responsibility as part of the job, as well as the legal implications when a lesion is “missed”. Cancer consciousness is therefore high among radiologists. On the other hand minor findings that have a low probability should not be pursued with aggressive and expensive evaluations.
The pulmonary nodule is a classical example of how cancer phobia led to a prolonged, expensive, and anxiety provoking 2 year course for many patients. Any non calcified nodule in the lung found on CXR in the past was destined to be followed over a two year period to ensure stability (Ost and Tan) CT programs for pulmonary nodules evolved (Aberle, Swensen, Henschke) with scans recommended at 3, ,12,18 and 24 month follow up.
The current data however suggests that only 1% of very small nodules (<5mm) become malignant (Henschke) and the Fleischner Society have proposed a modified and more reasonable strategy based on the size of the lesion, and the patient background dividing the population into a high risk and low risk group. Their recommendations are outlined below.
|
Nodule Size (mm)
|
Low risk patients
|
High risk patients
|
|
Less than or equal to 4
|
No follow-up needed.
|
Follow-up at 12 months. If no change, no further imaging needed.
|
|
>4 – 6
|
Follow-up at 12 months. If no change, no further imaging needed.
|
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
|
|
>6 – 8
|
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
|
Initial follow-up CT at 3 – 6 months and then at 9 -12 and 24 months if no change.
|
|
>8
|
Follow-up CTs at around 3, 9, and 24 months. Dynamic contrast enhanced CT, PET, and/or biopsy
|
Same at for low risk patients
|
Fleischner Society – Guidelines
Another common abnormality in patients over 50 is the renal cyst. 50% of patients over the age of 50 have cystic lesions of the kidney. Some of these have malignant features and Bosniak has developed criteria on the CTscan that allows radiologists to determine which of these lesions require surgical intervention.
Biopsy
Once a suspicious lesion as described above is identified then the usual next step is the pursuit of a pathological diagnosis. In the brain it requires neurosurgical biopsy. In the lung diagnosis by endoscopic technique or by CT guided percutaneous aspiration and core biopsy is utilized. Mediastinal biopsy is directed at suspicious nodes either based on their size, or their avidity for FDG. These nodes can sometimes be reached by the thoracic surgeon and more recently by transesophageal ultrasound.
Ultrasound guided biopsy is the preferred method for liver lesions since it is inexpensive, and does not involve radiation. This technique is highly effective when the lesion and the advancing needle are readily visualized.
Solid masses in the kidney ovary and the testis generally undergo surgical removal without a preoperative biopsy due in part of the high level of suspicion, and also to some extent the concern for spread of the disease by the invading needle.
Pancreatic biopsy using percutaneous technique is controversial, and it appears that this is more safely performed by endoscopic methods.
Endometrial biopsy is performed by the gynecologists per vaginally. Lymph node biopsy for lymphoma, or leukemia or for metastatic disease is usually performed using CT guidance, surgical biopsy if palpable, or by bone marrow aspiration.
The function of the pathologist at this stage is to document the diagnosis and to assess the type of cancer, and its innate biology and aggressiveness using morphological criteria. For example a lung biopsy specimen that shows carcinoma may be of the small cell or non small cell variety. If it is of the non small cell variety it can be squamous carcinoma, adenocarcinoma, (including bronchioalveolar) or large cell carcinoma. Within these categories it is defined as well differentiated, or poorly differentiated and some are dedifferentiated. The treatment algorithms and prognosis are in part based on this evaluation, but staging of the disease is the other arm that directs management and prognosis.

Classification system of carcinoma of the lung based on histological subtype
|
|
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02.jpg code lungs pulmonary neoplasm primary malignant malignancy small cell carcinoma non small cell NSCC classification histopathology
|
Staging
Cancer staging systems describe how far cancer has spread anatomically and attempt to put patients with similar prognosis and treatment in the same staging group(Ost). The prognosis of a cancer as well as treatment options depend upon the staging of the cancer and hence assigning a newly diagnosed cancer with a stage is an important step.
The stage is usually represented by Roman numerals from I to IV. Oftentimes alphabets are used as suffixes for precise staging.
In general stage I cancers are localized cancers and are curable and options such as surgery or local radiation may be curative. Subgroupings such as a, b, and c are commonly used as suffixes to better define size and depth of invasion. Stage II and III are locally advanced cancer usually with involvement of locoregional lymph nodes. Stage IV are tumors that have spread to other organs such as liver lung or bone. Tumor staging may vary quite a bit depending on the type and site of the tumor.
TNM Staging
In the TNM system, TNM stands for Tumor, Nodes, and Metastases. Each of these is categorized separately and classified with a number to give the total stage. Thus a T1N1M0 cancer means the patient has a T1 tumor, N1 lymph node involvement, and no distant metastases. The definitions of T, N and M are specific to each cancer.
T: Tumor
T Classifies the extent of the primary tumor, and is normally given as T0 through T4. T0 represents a tumor that has not even started to invade the local tissues. This is called “In Situ”. T4 on the other hand represents a large primary tumor that has probably invaded other organs by direct extension, and which is usually inoperable.
N: Lymph Nodes
N classifies the amount of regional lymph node involvement. It is important to understand that only the lymph nodes draining the area of the primary tumor are considered in this classification. Involvement of distant lymph nodes is considered to be metastatic disease. The definition of which lymph nodes are regional depends on the type of cancer. N0 means no lymph node involvement while N4 means extensive involvement.
M: Metastasis
M is either M0 if there are no metastases or M1 if there are metastases.
As with the other system, the exact definitions for T and N are different for each different kind of cancer.
Recurrence of cancer may be defined as local recurrence or distant recurrence. It is not unusual for some cancer to recur as metastatic disease and be incurable.
Management
Principles
The patient should have realistic expectations as some treatment may work better in one person and not in another. The goal of treatment is multifold and includes attempt to cure, control disease, palliation of symptoms and prolongation of life. However the treatment is potentially toxic and should be used judiciously.
Surgery:
Surgery has the following roles in the cancer patient: cure, debulking of the tumor, amelioration of symptoms.
Chemotherapy:
Chemotherapy consists of potentially toxic therapy that target rapidly dividing cancer cells. However, most cancer drugs have severe adverse effects and therefore treatment should be tailored to each patient and their ability to withstand aggressive measures should be taken in to account. The field has broadened quite a bit in recent years with targeted therapies that target particular enzymes or substrate that may be unique to a particular cancer.
Radiation therapy:
Radiation therapy also has similar goals such as cure, control of disease and control of symptoms.
No treatment: patient that do not wish to undergo or are not candidates for aggressive treatment . Every effort should be made to control the bothersome symptoms as well as services such as hospice should be provided.
Like all patients, the oncologic patient, in particular, requires a holistic approach. This includes careful attention to the anatomic and physiologic uniqueness of the human body, the uniqueness of a particular malignancy, and also the context of the psychosocial milieu.
The, patient’s activities of daily living (ADL’s) serve as a backdrop to daily care, as well as strong predictors of prognosis. A diagnosis of cancer places enormous stress on individual patient as well as family and friends. Thus, the successful approach to the individual oncology patient hinges on an integrative understanding that ranges from cellular processes to family and community dynamics. In that vein, comprehensive oncologic assessment and care employs not only medical health professionals, but members of the patient’s family, and social workers as well. Additionally, quality cancer care traces the patient’s steps, literally and figuratively, from their home setting to the point of the evaluation in order to truly understand the context of that patient’s health and disease. Whether cancer therapy involves major surgery, chemotherapy or radiation, it is very challenging and a strong supportive environment increases the odds of successfully completing the therapy.
Multiple disciplines are involved in care of cancer patient, including primary care physicians, surgeons, radiation oncologists, pathologists, radiologists, nurses, nutritionists, physical therapists and above all the patient and the patient’s family. This interdisciplinary effort is essential and the core of cancer management.
Oncology Team
Psychological Aspects
Critical illness leaves no aspect of life untouched. Diagnosis of cancer, as well as stress associated with cancer, is trying for most patients. The initial period is dominated by medical aspects of obtaining diagnostic information and undertaking primary or adjuvant therapy. Fear anxiety and pain are common at this stage. Coping with therapy requires all the adaptive energies of most patients. Following treatment, there is an extended period when patients adjust to the follow up after acute treatment. Providing psychosocial support to patients during these phases is essential.
Families and friends are an important source of psychological support. Social workers are also an important source of support to patients. For patient in terminal stages of cancer patient may have fear, pain and felling of helplessness and loss of control over their lives. It is important allow patients to take control of their lives and treatment decisions. Patients also worry about being a burden on their families. Therefore it is important to allow the patients to make decisions about where they want to be treated.
Family
Family member undergo considerable psychological turmoil when a loved one is diagnosed with cancer. The distress may at times be considerable enough to affect the patient. Best way to deal with these issues to educate and provide support to family members as sometimes they may be the primary caregiver of the patients. Some patients may not like the family members to be involved in their care.
Social
Cancer affects many aspect of a person’s life. There may be challenges in the family environment, friends as well as work.
Most patients are anxious when they are told that they have cancer. They may worry abut whether they will be able to work while they are being treated. There every day life is affected and they may have questions such as …. Will I lose my hair? Will my appearance change? How will my social life be impacted? Will I be able to go out and enjoy a meal in the restaurant?
Most patients are able to work through their diagnosis and treatment. The ability to that depends on patient’s age and performance status prior to beginning the therapy. Patient may feel conscious about hair loss while going out in public therefore an effort should be made to address this issue at the outset. The oncology nurse will usually go over with the patient about wigs and uses. Most patients are able to go out and spend time with the family and friends however if they are neutropenic than it is recommended that they avoid crowded places and certain foods. Patient undergoing transplant may be asked to make lifelong dietary changes to eat only well done meats.
Nutritional
Nutrition is an important aspect of any cancer patients’ care. Patient may lose weight and appetite secondary to the cancer. Challenges to nutrition are in form of Chemotherapy induced nausea, vomiting , mucositis and diarrhea and radiation induced mucositis and diarrhea . Patient may become severely dehydrated and their nutrition may suffer severely. It is important to take a good nutritional history as well as history of any adverse effect that may severely impact oral intake. A focused exam should include looking for mucositis. Patient may do well with nutritional shakes and soft diet while these symptoms abate. A nutritional consult is often helpful in determining the available options.
Chemotherapy
Chemotherapy – the use of medications to treat cancer – has played a major role in cancer treatment for half a century. The cancer drugs work by killing the rapidly dividing cells. Since cancer cell are rapidly dividing they are affected more than the other tissues. However there are certain normal cells in the body that have very rapid turnover and are affected by chemotherapy such as bone marrow and gastrointestinal epithelium and hair follicles. Therefore patients receiving chemotherapy may suffer decrease blood cell counts, hair loss and diarrhea. Unlike radiation and surgery which are much more localized chemotherapy can target cancer cells that have escaped from the original tumor site and may cause metastasis.
Chemotherapy may be used for following goals depending upon staging and type of cancer.
- Cure of the cancer by eliminating all cancer cells in your body, even when cancer is widespread
- Prolong life by controlling cancer growth and spread
- Relieve symptoms and enhance quality of life
- In conjunction with radiation as radiosensitizers making cancer cells more susceptible to radiation
- Following surgery to enhance results called as adjuvant therapy.
- Prior to surgery or radiation making disease more amenable to treatment and is called as neoadjuvant therapy.
Modes of administrations:
- Intravenous (IV). Chemotherapy is injected into a vein, This allows rapid distribution of the chemotherapy throughout entire body.
- Oral. In form of a pill
- Topical. This type of drug is applied to skin to treat localized skin cancers.
- Injection. Intramuscular injection.
Side effects
Symptomatic – Pain /Nausea
Temporary side effects might include:
- Hair loss
- Dry mouth
- Mouth sores (stomatitis)
- Difficult or painful swallowing (esophagitis)
- Nausea
- Vomiting
- Diarrhea
- Constipation
- Fatigue
- Bleeding
- Susceptibility to infection
- Infertility
- Loss of appetite
- Changes in the way food tastes
- Cognitive impairment, sometimes referred to as “chemo brain”
- Liver damage
- Heart damage
- Nerve damage
- Lung damage
How long these temporary side effects last depends on what drug or combination of drugs and treatment duration. Most chemotherapy side effects will subside shortly after conclusion of treatments. And most short-term side effects can be minimized with medication
Long-term or late chemotherapy side effects
As people with cancer live longer after treatment, doctors are discovering that some treatments cause long-lasting side effects or side effects that become apparent long after treatment ends. These long-term side effects are rare. Some chemotherapy drugs can cause:
- Organ damage, including problems with your heart, lungs and kidneys
- Nerve damage
- Blood in your urine (hemorrhagic cystitis)
- Another cancer, including Hodgkin’s disease and non-Hodgkin’s lymphoma, leukemia and some tumors
Chemotherapy nausea and vomiting: Prevention is best defense
Following factors affect nausea and vomiting 15
Chemotherapy drugs : Are divided in to categories as per the emetogenic potential; category 1 is low risk , category 2 and 3 are intermediate risk and category 4 are high risk,
Patient parameters : patient with following parameters are more susceptible :
Younger age less than 50 yrs
Women
Anxious individual
Previous history of nausea and vomiting
What antinausea medication is used is dependent on chemotherapeutic regimen
commonly used anti-nausea medications include following categories
High efficacy
5 HT 3 antagonists
- Ondansetron (Zofran)
- Dolasetron (Anzemet)
- Granisetron (Kytril)
- Palonosetron (Aloxi)
Steroids
NK 1 inhibitors
Aprepitant
Fosaprepitant
Low efficacy
Prochlorperazine
Metoclopramide (Reglan)
Haloperidol
Lorazepam (Ativan)
Patient instructions
- Eat small meals. Stagger small meals throughout the day rather than eating fewer, larger meals..
- Eat what appeals to you. However try , to avoid foods that are sweet, fried or fatty. In addition, cool foods may give off less-bothersome odors. Cook and freeze meals in advance of treatment to avoid cooking when you’re not feeling well. Or have someone else cook for you.
- Drink lots of fluids. Such as water, avoid carbonated or caffeinated drinks.
- Avoid unpleasant smells. Certain smells may trigger nausea and vomiting
- Make yourself comfortable. After eating, rest, but don’t lie flat for a couple of hours. Try wearing loose fitting clothing and keeping yourself distracted.
- Use relaxation techniques. Examples include meditation and deep breathing.
Surgery
Cancer surgery may be used to achieve one or more goals. Common reasons to undergo cancer surgery include:
- Cancer prevention. In patients with genetic predisposition to cancer such as BRCA mutation prophylactic surgery may be considered as preventive measure.
- Diagnosis. A mass may have to be removed entirely or partially to obtain a histopathological diagnosis
- Staging. Cancer surgery helps define Stage of the cancer
- Primary treatment. For many tumors, cancer surgery is the best chance for a cure, especially if the cancer is localized and hasn’t spread.
- Debulking. When it’s not possible to remove all of a cancerous tumor – for example, because doing so may severely harm an organ -doctor may remove as much as possible (debulking) in order to make chemotherapy or radiation more effective.
- Relieving symptoms or side effects. Sometimes surgery is used to improve quality of life rather than to treat the cancer itself – for example, to relieve pain caused by a tumor that’s pressing on a nerve or bone or to remove a tumor that’s obstructing the bowels.
Surgery is often combined with other cancer treatments, such as chemotherapy and radiation.
Radiation
About half of all people treated for cancer receive some form of radiation therapy – the use of high-powered radiation to kill cancer cells. The majority of people receive radiation therapy from a machine outside of their body, a treatment called external beam radiation therapy. Brachytherapy allows doctors to place radioactive material inside the patients’ body and delivers high radiation to specific area of the body.
Radiation oncology doctors use a CT scan to simulate the area to be irradiated/
Side effects of radiation are following
GI effects; Esophagitis, Diarrhea
Local effects such as skin break down or burn
Bone marrow suppression
Tiredness and fatigue
|
Range of Cancer Therapies
|
| This is a collage of the usual treatments available for lung cancer. Top left depicts the XRT option while the Caravaggio of the sacrifice of Isaac is the surgical option and bottom left the chemotherapeutic option.
Courtesy Ashley Davidoff MD. 31432c code lung pulmonary mass neoplasm malignant primary malignancy carcinoma imaging radiology CTscan treatment |
New Advances
The field of cancer is changing everyday. There are new and improved drugs that are coming out or in pipeline
Targeted therapy: These drugs target a particular abnormality or receptor in the cancer cells and therefore normal cells may be spared from chemotherapy.
Radioimmunotherapy: radioactive ligands such as iodine are tagged on to antibody targeting a specific molecule and thus allow for targeted radiation and immunotherapy
Defining risk and response in the patients: Scientists are looking for parameters that may predict if a tumor will respond to a particular chemotherapy and therefore allowing the patient to be treated only if they have responsive disease.
End of Life Issues
End of life issues are major part of caring for a cancer patient. It is important to help a patient and family understand their prognosis and help them cope with their terminal illness.
Hospice:
Hospice care is a philosophy about care of people who are nearing the end of their lives. Hospice care is designed to relieve pain, or other symptoms, and provide as much quality time as possible with family and friends. The focus of hospice care is no longer on curing or treating the underlying disease. The goal of hospice care is to provide the highest quality of life for whatever time remains.
It is important to emphasize to the patient that by discussing hospice you are not abandoning them. Instead you are helping them focus on care and spending time with the family.
There are two types of hospice care: home hospice and residential hospice in an institution. Any one of these may be chosen depending upon patients family situation and social support.
A hospice care team consists of following:
Doctor: provides a treatment plan tailored to the patient and as well as performs a supervisory role.
Hospice nurses are trained professional who are expert in providing pain and symptom relief to a terminally ill patient.
Home health aides: provide care to a patient
Prognosis
Prognosis is usually defined as by parameters such as 5 or 10 year overall survival, event free survival and recurrence free survival. It is important to always pay attention to overall survival while reviewing treatment options as some treatments my appear to confer benefit but do not improve overall survival
Prognosis is usually dependent on following factors:
Type of cancer: some cancer by nature may be curable and have low tendency to recur while other cancers that are biologically aggressive tend to recur or are more likely to be metastasized. Cancer such as indolent lymphomas may be indolent for many years and are also incurable.
Location: Location of cancer is an important factor as surgery may not be an option in such case, for example some areas of brain. On the other hand pancreatic cancer is usually discovered late as it is retroperitoneal organ and does not produce symptoms until it fairly large in size when it is mostly inoperable.
Staging: Staging a single most important factor in a patient with cancer. Most but not all early stage cancer are curable. Metastatic cancers by and large have poor prognosis.
Grade: Grade of tumor is a very important factor. The higher the grade more aggressive a tumor is and thus worse prognosis
Performance status of the patient: while aggressive chemotherapy may cure certain cancer it may not be possible to treat all patients aggressively. Oftentimes chemotherapy may be modified according to a patient’s baseline performance status and advanced age.
Identification of biochemical markers or presence of targeted therapy: Development of Imatinib which is BCR ABL inhibitor has revolutionized the treatment of chronic myeloid leukemia. Similarly the presence of estrogen and progesterone receptors and her 2 over expression in breast cancer is amenable to treatment with hormonal therapy and trastuzumab which is a monoclonal antibody against herceptin. Targeted therapies have the advantage of destroying tumors cell with minimal effect on normal cells and thus are going to be very important in future.
Red Flags
The following conditions should warrant concern and a comprehensive emergency room evaluation in the oncology patient, as they may be signs of a life-threatening condition:
Fever
New or sudden chest, back or abdominal pain
Night sweats and extreme fatigue
Pre-syncope or syncope
Severe eye or headache
Change in mental status, including but not limited to confusion and lethargy.
Focal weakness.
Dysphagia
Productive cough
Hemoptysis
Tachypnea .
Tachycardia,
Bony pain
New abdominal distension.
Bloody or black tarry stools with or without symptoms.
Fall with or without head trauma
Patient / Family information
Evaluation and care of the Oncology patient can markedly complex, yet their integration and simplification is the key to success. Recognition of subtle warning signs, like confusion, or not so subtle signs high fever, can be the difference between life and death in oncology patients at home. That being said, the emergency room is rarely the first stop in managing oncological medical problems. Rather, often times phone management, clinic appointments and prompt hospitalizations when required are a preferable alternative, when possible. It is ideal for patient to have access to support from friend and families and 24 hour access to medical team for any complication that may arise.
References
AJCC cancer staging manual ; 6th addition
1. Ost D, Fein AM, Feinsilver SH. The solitary pulmonary nodule. N Engl J Med 2003; 348:2535-2542.
2. Tan BF, Kazerooni E, Iannettoni M. The solitary pulmonary nodule. Chest, 2003; 123: p. 89S-96S.
6. Aberle D, Gamsu G, Henschke CI, Naidich DP, Swensen SJ. A consensus statement of the society of thoracic radiology screening for lung cancer with helical computed tomography. Journal of Thoracic Imaging, 2001; 16: p.65-68. 21
7. Swensen SJ, Jett JR, Hartman T, Midthun D, Sloan J, Sykes A, Aughenbaugh G, Clemens M. Screening for lung cancer with CT: Mayo Clinic experience. Radiology, 2003; 226: p. 756-761.
8. Henschke CI, Naidich DP, Yankelevitz DF, McGuinness G, et al. Early lung cancer action project: initial findings on repeat screening. Cancer, 2001; 92: p. 153-159.
Henschke CY, Naidich DP, McCauley, D, McGuinness, G, Libby, Smith J.P, Pasmantier MW, Miettinen O. CT Screening for lung cancer: suspiciousness of nodules according to size on baseline scans. Radiology, 2004; 231: p. 164-168.
9 . Henschke CI, McCauley DI, Yankelevitz D, et al. Early lung cancer action project:
Karpozilos A, Pavlidis N (2004). “The treatment of cancer in Greek antiquity”. Eur. J. Cancer 40 (14): 2033-40.
10 . Cancer Research UK
11. Joseph S. Paganoa, Martin Blaserb, Marie-Annick Buendiac, Blossom Damaniad, Kamel Khalilie, Nancy Raab-Traubf and Bernard Roizmang Infectious agents and cancer: criteria for a causal relation Seminars in Cancer Biology Volume 14, Issue 6, December 2004, Pages 453-471
12. Croce CM (January 2008). “Oncogenes and cancer“. The New England journal of medicine 358 (5): 502-11.
13. C. A. Klein, The metastasis cascade. Science 321, 1785-1787 (2008).
14. The Cancer Cachexia Syndrome: A Review of Metabolic and Clinical Manifestations
Dema Halasa Esper, MS, RD, CNSD* and Wael A. Harb, MD
15 Chemotherapy-Induced Nausea and Vomiting
Hesketh PJ NEJM , June 5, 2008
MCQ
Questions
1.What are * somatic events
2. Which of the following is a true statement?
(a) Cancer cells are similar in appearance to normal tissue.
(b) Cancer cells are functionally similar to normal tissue.
(c) cancer cells acquire abnormal ability to divide and lose the capability of programmed cell death (apoptosis).
(d) Cancer cells usually have no mutations.
3. A 50 year old woman has noticed a left breast lump and referred to your center.
What should be done next?
- (a) Mammogram to define the lump and to rule out any suspicious areas in the opposite breast.
- (b) Biopsy of the lump
- (c) Mastectomy
- (d) Chemotherapy
4. Which of the following will increase the risk of the woman in question number 3 for breast cancer/
- (a) Breast feeding
- (b) Vegetarian diet
- (c) Early menopause
- (d) History of breast cancer in mother and sister
5. A 67 year old Spanish speaking woman has been referred to your clinic with diagnosis of metastatic colon cancer. Her family does not want to tell her about her diagnosis and requests you to treat her aggressively. How will you manage this situation?
(a) Comply with the family’s wishes?
(b) Refuse to treat the patient
(c) Talk to the patient through an interpreter to determine if she wished to know her diagnosis.
(d) Go ahead and tell the patient her diagnosis and treatment options
6. T in the TNM staging signifies
(a) Number of lymphnodes
(b) Number of primary tumors
(c) spread to other organs
(d) Tumor size
7. A woman who is currently undergoing treatment for lung cancer with chemotherapy and radiation comes in with severe mucositis of her mouth. In addition to symptomatic management what nutrition advice will you give her.
(a) To eat low salt, low fat diet
(b) To eat soft or pureed diet to avoid irritation to the mucosa of mouth and esophagus
(c) To eat green vegetables.
(d) Reduce oral intake as much as possible.
8. A woman returns to clinic 10 days after her last chemotherapy session. Her total white count is 500 (normal is 4000-10000).
What instruction should you give her?
- (a) To avoid cooked food
- (b) To check temperature three times a day and call the doctor if temperature is more than 100.4 F
- (c) To avoid taking a bath
- (d) Avoid any other medications
- Chemotherapy has made tremendous strides in last few years; what are the major changes in treatment in last few years.
- (a) Treatment is more aggressive
- (b) There are new drugs that more toxic to cancer cells as well as
- (c) All patient are being treated per protocols
- (d) Increasingly the treatment is individualized and targeted to maximize outcome and avoid toxicity.
10.What is the role of PET scan in management of cancer?
- (a) Diagnosis of cancer
- (b) Staging
- (c) Differentiation between benign and malignant cancer
- (d) All of the above
11.which of the following is not commonly used anti nausea medication for cancer patients.
- (a) 5 HT3 antagonist
- (b) NKV1 inhibitor
- (c) Steroids
- (d) Amitryptilline
12. A 54 year old year woman returns to clinic for annual you will recommend all screening modalities except.
(a) mammogram
(b) Pap smear
(c) CT scan of chest
(d)Colonoscopy
13.
Ultrasound is imaging modality of choice in all except
- (a) Metastatic lung cancer
- (b) Ovarian cancer
- (c) Testicular neoplasm
- (d) Renal vein thrombosis
14. Which if the following is not a part of hospice care
- (a) Pain medication including opiates
- (b) Oxygen
- (c) Treatment of acute infections
- (d) Active treatment of a terminal cancer
- 15. Which of the following is a red flag for cancer
- (a) unexplained fever
- (b) blood in bowel movements
- (c) fatigue
- (d) all of the above
- 16. Which of the following statement is false
- (a) Diagnosis of cancer is life altering for most patients
- (b) Most patient on chemotherapy are too sick to do anything else
- (c) Cancer patients require lot of support during treatment
- (d) Chemotherapy may induce fatigue in most patient
17. Which of the following is risk factor for nausea vomiting
- (a) Anxiety
- (b) Older age
- (c) Male gender
- (d) Alcohol use
18. Which if the following is a common laboratory abnormality seen in cancer patients
- (a) Anemia
- (b) High blood sugar
- (c) High creatinine
- (d) Low potassium
Answers 2.c, 3 . A 4. D 5.C. 6. D 7. B 8 B, 9. D 10. D, 11 D , 12 C. 13 A, 14 D, 15. D , 16 B, 17 A, 19 A
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Range of Cancer Therapies
This is a collage of the usual treatments available for lung cancer. Top left depicts the XRT option while the Caravaggio of the sacrifice of Isaac is the surgical option and bottom left the chemotherapeutic option.
Courtesy Ashley Davidoff MD. 31432c code lung pulmonary mass neoplasm malignant primary malignancy carcinoma imaging radiology CTscan treatment
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Range of Cancer Therapies
This is a collage of the usual treatments available for lung cancer. Top left depicts the XRT option while the Caravaggio of the sacrifice of Isaac is the surgical option and bottom left the chemotherapeutic option.
Courtesy Ashley Davidoff MD. 31432c code lung pulmonary mass neoplasm malignant primary malignancy carcinoma imaging radiology CTscan treatment
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a collage of the usual treatments available for lung cancer. Top left depicts the XRT option while the Caravaggio of the sacrifice of Isaac is the surgical option and bottom left the chemotherapeutic option.
Courtesy Ashley Davidoff MD. 31432c code lung pulmonary mass neoplasm malignant primary malignancy carcinoma imaging radiology CTscan treatment
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a collage of the usual treatments available for lung cancer. Top left depicts the XRT option while the Caravaggio of the sacrifice of Isaac is the surgical option and bottom left the chemotherapeutic option.
Courtesy Ashley Davidoff MD. 31432c code lung pulmonary mass neoplasm malignant primary malignancy carcinoma imaging radiology CTscan treatment
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Range of Cancer Therapies
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Range of Cancer Therapies
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Classification system of carcinoma of the lung based on histological subtype
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02.jpg code lungs pulmonary neoplasm primary malignant malignancy small cell carcinoma non small cell NSCC classification histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Classification system of carcinoma of the lung based on histological subtype
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02.jpg code lungs pulmonary neoplasm primary malignant malignancy small cell carcinoma non small cell NSCC classification histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02.jpg code lungs pulmonary neoplasm primary malignant malignancy small cell carcinoma non small cell NSCC classification histopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02.jpg code lungs pulmonary neoplasm primary malignant malignancy small cell carcinoma non small cell NSCC classification histopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Classification system of carcinoma of the lung based on histological subtype
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Classification system of carcinoma of the lung based on histological subtype
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Nodule Size (mm)
Low risk patients
High risk patients
Less than or equal to 4
No follow-up needed.
Follow-up at 12 months. If no change, no further imaging needed.
>4 – 6
Follow-up at 12 months. If no change, no further imaging needed.
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
>6 – 8
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
Initial follow-up CT at 3 – 6 months and then at 9 -12 and 24 months if no change.
>8
Follow-up CTs at around 3, 9, and 24 months. Dynamic contrast enhanced CT, PET, and/or biopsy
Same at for low risk patients
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Nodule Size (mm)
Low risk patients
High risk patients
Less than or equal to 4
No follow-up needed.
Follow-up at 12 months. If no change, no further imaging needed.
>4 – 6
Follow-up at 12 months. If no change, no further imaging needed.
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
>6 – 8
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
Initial follow-up CT at 3 – 6 months and then at 9 -12 and 24 months if no change.
>8
Follow-up CTs at around 3, 9, and 24 months. Dynamic contrast enhanced CT, PET, and/or biopsy
Same at for low risk patients
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Same at for low risk patients
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Same at for low risk patients
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Follow-up CTs at around 3, 9, and 24 months. Dynamic contrast enhanced CT, PET, and/or biopsy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Follow-up CTs at around 3, 9, and 24 months. Dynamic contrast enhanced CT, PET, and/or biopsy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
>8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
>8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Initial follow-up CT at 3 – 6 months and then at 9 -12 and 24 months if no change.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Initial follow-up CT at 3 – 6 months and then at 9 -12 and 24 months if no change.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
>6 – 8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
>6 – 8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Initial follow-up CT at 6 -12 months and then at 18 – 24 months if no change.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Follow-up at 12 months. If no change, no further imaging needed.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Follow-up at 12 months. If no change, no further imaging needed.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
>4 – 6
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
>4 – 6
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Follow-up at 12 months. If no change, no further imaging needed.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Follow-up at 12 months. If no change, no further imaging needed.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
No follow-up needed.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
No follow-up needed.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Less than or equal to 4
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Less than or equal to 4
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
High risk patients
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
High risk patients
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Low risk patients
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Low risk patients
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Nodule Size (mm)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Nodule Size (mm)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pathological Specimen of an Apple core Deformity
Portion of left colon with a constricting apple core carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
12313 Courtesy Barbara Banner MD aka applecore
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pathological Specimen of an Apple core Deformity
Portion of left colon with a constricting apple core carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
12313 Courtesy Barbara Banner MD aka applecore
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Portion of left colon with a constricting apple core carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
12313 Courtesy Barbara Banner MD aka applecore
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Portion of left colon with a constricting apple core carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
12313 Courtesy Barbara Banner MD aka applecore
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pathological Specimen of an Apple core Deformity
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pathological Specimen of an Apple core Deformity
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Apple Core Lesion in the Sigmoid Colon
The images are from a double contrast barium enema. Contrast and air have been instilled into the rectum and images of the sigmoid colon were taken with fluoroscopic guidance. The first image reveals a narrow lumen, the second shows the apple core deformity (green)and the third has the overlay of where the tumor (light orange is positioned), and reveals how it causes the tight band like constriction of the lumen (green) to result in the apple core deformity described.
00878 00877 Courtesy Ashley Davidoff MD 5star aka applecore
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Apple Core Lesion in the Sigmoid Colon
The images are from a double contrast barium enema. Contrast and air have been instilled into the rectum and images of the sigmoid colon were taken with fluoroscopic guidance. The first image reveals a narrow lumen, the second shows the apple core deformity (green)and the third has the overlay of where the tumor (light orange is positioned), and reveals how it causes the tight band like constriction of the lumen (green) to result in the apple core deformity described.
00878 00877 Courtesy Ashley Davidoff MD 5star aka applecore
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The images are from a double contrast barium enema. Contrast and air have been instilled into the rectum and images of the sigmoid colon were taken with fluoroscopic guidance. The first image reveals a narrow lumen, the second shows the apple core deformity (green)and the third has the overlay of where the tumor (light orange is positioned), and reveals how it causes the tight band like constriction of the lumen (green) to result in the apple core deformity described.
00878 00877 Courtesy Ashley Davidoff MD 5star aka applecore
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The images are from a double contrast barium enema. Contrast and air have been instilled into the rectum and images of the sigmoid colon were taken with fluoroscopic guidance. The first image reveals a narrow lumen, the second shows the apple core deformity (green)and the third has the overlay of where the tumor (light orange is positioned), and reveals how it causes the tight band like constriction of the lumen (green) to result in the apple core deformity described.
00878 00877 Courtesy Ashley Davidoff MD 5star aka applecore
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Apple Core Lesion in the Sigmoid Colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Apple Core Lesion in the Sigmoid Colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Spiculated Mass in the Right Breast
This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology.
42977 Courtesy Priscilla Slanetz MD breast CASE 27:
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Spiculated Mass in the Right Breast
This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology.
42977 Courtesy Priscilla Slanetz MD breast CASE 27:
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology.
42977 Courtesy Priscilla Slanetz MD breast CASE 27:
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology.
42977 Courtesy Priscilla Slanetz MD breast CASE 27:
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Spiculated Mass in the Right Breast
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Spiculated Mass in the Right Breast
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Spiculated Lung Nodule
The shape of the lung nodule seen on the chest CT in the right upper lobe with radiating spokes or spicules is characteristic a lung carcinoma and was proven to be a primary cancer of the lung. The spicules represent sheets of tumor cells extending into lymphatics or interstitium, or obstructed vessels.
46361 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Spiculated Lung Nodule
The shape of the lung nodule seen on the chest CT in the right upper lobe with radiating spokes or spicules is characteristic a lung carcinoma and was proven to be a primary cancer of the lung. The spicules represent sheets of tumor cells extending into lymphatics or interstitium, or obstructed vessels.
46361 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The shape of the lung nodule seen on the chest CT in the right upper lobe with radiating spokes or spicules is characteristic a lung carcinoma and was proven to be a primary cancer of the lung. The spicules represent sheets of tumor cells extending into lymphatics or interstitium, or obstructed vessels.
46361 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The shape of the lung nodule seen on the chest CT in the right upper lobe with radiating spokes or spicules is characteristic a lung carcinoma and was proven to be a primary cancer of the lung. The spicules represent sheets of tumor cells extending into lymphatics or interstitium, or obstructed vessels.
46361 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Spiculated Lung Nodule
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Spiculated Lung Nodule
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Crab Like?
The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics as seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image to the authors eye has a crab like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
32317.8s Courtesy Ashley Davidoff and Jeffrey Peirce A86-215 32317 copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Crab Like?
The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics as seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image to the authors eye has a crab like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
32317.8s Courtesy Ashley Davidoff and Jeffrey Peirce A86-215 32317 copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics as seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image to the authors eye has a crab like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
32317.8s Courtesy Ashley Davidoff and Jeffrey Peirce A86-215 32317 copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The post mortem specimen of the lung and overlying pleura is from a patient who died of metastatic cancer. A surface metastasis to the pleura causes obstruction and distension of the pleural lymphatics as seen as white irregular vessels coursing to (or from) the mass. These lymphatics are normally about the thickness of a hair and not commonly visualized. In this instance they are obstructed by the tumor, and are therefore distended with white lymph and at about .05mm (thickness of the pin) they are readily seen. This image to the authors eye has a crab like shape with the nodule representing the body, and the lymphatics reminiscent of the legs.
32317.8s Courtesy Ashley Davidoff and Jeffrey Peirce A86-215 32317 copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Crab Like?
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Crab Like?
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Positive PET scan
The CT scan and PET scan are from a patient with both esophageal carcinoma and colon carcinoma that were treated in the past. Follow up CT scan of the chest showed a new nodule in the right upper lobe. (a,b, white arrow) and also showed thickening of the esophagus (red arrow). PET scan showed an isolated hot spot in the right upper lobe and no uptake in the esophagus where recurrence was a possibility based on the thickening. Biopsy confirmed metastatic colon carcinoma.
85224cb01.8s CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Positive PET scan
The CT scan and PET scan are from a patient with both esophageal carcinoma and colon carcinoma that were treated in the past. Follow up CT scan of the chest showed a new nodule in the right upper lobe. (a,b, white arrow) and also showed thickening of the esophagus (red arrow). PET scan showed an isolated hot spot in the right upper lobe and no uptake in the esophagus where recurrence was a possibility based on the thickening. Biopsy confirmed metastatic colon carcinoma.
85224cb01.8s CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CT scan and PET scan are from a patient with both esophageal carcinoma and colon carcinoma that were treated in the past. Follow up CT scan of the chest showed a new nodule in the right upper lobe. (a,b, white arrow) and also showed thickening of the esophagus (red arrow). PET scan showed an isolated hot spot in the right upper lobe and no uptake in the esophagus where recurrence was a possibility based on the thickening. Biopsy confirmed metastatic colon carcinoma.
85224cb01.8s CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CT scan and PET scan are from a patient with both esophageal carcinoma and colon carcinoma that were treated in the past. Follow up CT scan of the chest showed a new nodule in the right upper lobe. (a,b, white arrow) and also showed thickening of the esophagus (red arrow). PET scan showed an isolated hot spot in the right upper lobe and no uptake in the esophagus where recurrence was a possibility based on the thickening. Biopsy confirmed metastatic colon carcinoma.
85224cb01.8s CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Positive PET scan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Positive PET scan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Anterior and Posterior Commissures
The T1 weighted sagittal image of the midbrain shows a hyperintense lesion in this patient with melanoma. Hyperintensity on T1 is most commonly associated with acute hemorrhage, but is also seen in melanoma.
21731 brain fx mass dx metastasis dx melanoma MRI T1 sagittal Courtesy James Donnelly MD Uploaded RP
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Anterior and Posterior Commissures
The T1 weighted sagittal image of the midbrain shows a hyperintense lesion in this patient with melanoma. Hyperintensity on T1 is most commonly associated with acute hemorrhage, but is also seen in melanoma.
21731 brain fx mass dx metastasis dx melanoma MRI T1 sagittal Courtesy James Donnelly MD Uploaded RP
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The T1 weighted sagittal image of the midbrain shows a hyperintense lesion in this patient with melanoma. Hyperintensity on T1 is most commonly associated with acute hemorrhage, but is also seen in melanoma.
21731 brain fx mass dx metastasis dx melanoma MRI T1 sagittal Courtesy James Donnelly MD Uploaded RP
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The T1 weighted sagittal image of the midbrain shows a hyperintense lesion in this patient with melanoma. Hyperintensity on T1 is most commonly associated with acute hemorrhage, but is also seen in melanoma.
21731 brain fx mass dx metastasis dx melanoma MRI T1 sagittal Courtesy James Donnelly MD Uploaded RP
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Anterior and Posterior Commissures
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Anterior and Posterior Commissures
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Lung Biopsy
The CT is from an 81 year old man with remote history of smoking who presents with an asymtomatic lung mass. The lesion was PET positive, without nodal activitiy suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
85221c01.8s Courtesy Ashley Davidoff MD all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Lung Biopsy
The CT is from an 81 year old man with remote history of smoking who presents with an asymtomatic lung mass. The lesion was PET positive, without nodal activitiy suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
85221c01.8s Courtesy Ashley Davidoff MD all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CT is from an 81 year old man with remote history of smoking who presents with an asymtomatic lung mass. The lesion was PET positive, without nodal activitiy suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
85221c01.8s Courtesy Ashley Davidoff MD all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CT is from an 81 year old man with remote history of smoking who presents with an asymtomatic lung mass. The lesion was PET positive, without nodal activitiy suggesting that it was either an infection, inflammatory lesion or a primary lung cancer. A biopsy revealed adenocarcinoma of the lung. In the image the patient has been placed in the prone projection. The needle (arrow is shown) within the spiculated lesion. The radiologist needed to avoid the major fissure which is seen as a fine curvilinear structure posteriorly (red arrow), negotiate the scapula and two closely spaced ribs. Without CT guidance this procedure would have been almost impossible to biopsy.
85221c01.8s Courtesy Ashley Davidoff MD all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Lung Biopsy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Lung Biopsy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cyst – (right) and Solid Cancer in the Kidney (left)
This ultrasound scan demonstrates the classical features of a cyst with absence of internal echoes, back wall enhancement and through transmission of sound waves. This cyst was exophytic off the right kidney. The second image shows a solid mass off the inferior aspect of the right kidney with internal echoes. The cyst is simple and requires no further diagnostic attention, while the solid mass requires surgical intervention.
Courtesy Ashley DAvidoff MD 39051b 39052b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cyst – (right) and Solid Cancer in the Kidney (left)
This ultrasound scan demonstrates the classical features of a cyst with absence of internal echoes, back wall enhancement and through transmission of sound waves. This cyst was exophytic off the right kidney. The second image shows a solid mass off the inferior aspect of the right kidney with internal echoes. The cyst is simple and requires no further diagnostic attention, while the solid mass requires surgical intervention.
Courtesy Ashley DAvidoff MD 39051b 39052b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This ultrasound scan demonstrates the classical features of a cyst with absence of internal echoes, back wall enhancement and through transmission of sound waves. This cyst was exophytic off the right kidney. The second image shows a solid mass off the inferior aspect of the right kidney with internal echoes. The cyst is simple and requires no further diagnostic attention, while the solid mass requires surgical intervention.
Courtesy Ashley DAvidoff MD 39051b 39052b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This ultrasound scan demonstrates the classical features of a cyst with absence of internal echoes, back wall enhancement and through transmission of sound waves. This cyst was exophytic off the right kidney. The second image shows a solid mass off the inferior aspect of the right kidney with internal echoes. The cyst is simple and requires no further diagnostic attention, while the solid mass requires surgical intervention.
Courtesy Ashley DAvidoff MD 39051b 39052b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cyst – (right) and Solid Cancer in the Kidney (left)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cyst – (right) and Solid Cancer in the Kidney (left)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] =>
[lastChild] =>
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] =>
[lastChild] =>
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] =>
[lastChild] =>
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be reduced in patient with lymphoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be reduced in patient with lymphoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Cell mediated immunity
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cell mediated immunity
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Increased with prostate cancer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Increased with prostate cancer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
PSA
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
PSA
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Is associated with ovarian cancer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Is associated with ovarian cancer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Ca 125
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Ca 125
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Is high in colon cancer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Is high in colon cancer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
CEA
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CEA
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hypercalcemia is a common electrolyte abnormality in cancer patients.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hypercalcemia is a common electrolyte abnormality in cancer patients.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Calcium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Calcium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cancer can cause renal failure either by tumor lysis syndrome or abnormal protein
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cancer can cause renal failure either by tumor lysis syndrome or abnormal protein
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
GFR
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
GFR
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hypoxia may be associated with lung cancers
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hypoxia may be associated with lung cancers
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
PaO2
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
PaO2
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Many cancers can cause hypercalcemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Many cancers can cause hypercalcemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Calcium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Calcium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be increased with tumor lysis syndrome
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be increased with tumor lysis syndrome
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Potassium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Potassium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be increased with ovarian cancer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be increased with ovarian cancer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be increased due to thyroid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be increased due to thyroid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
T3
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
T3
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be increased with sex cord tumors
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be increased with sex cord tumors
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Testosterone
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Testosterone
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be increased with some adrenal tumors
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be increased with some adrenal tumors
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
DHEA
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
DHEA
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
ACTH producing tumor may cause hyperglycemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
ACTH producing tumor may cause hyperglycemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Insulin blood sugar
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Insulin blood sugar
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
May be reduced by cancer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
May be reduced by cancer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
WBC and platelets
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
WBC and platelets
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
cancer patients are usually anemic but renal cancer may cause polycythemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
cancer patients are usually anemic but renal cancer may cause polycythemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
hemoglobin
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
hemoglobin
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => td
[nodeValue] =>
Lab Value
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Lab Value
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Bilateral Adrenal Metastases
The CTscan of the upper abdomen is from a patient with known lung carcinoma. The size, bilaterality and the heterogeneous appearance, particularly on the right are reminiscent of metastatic disease. In image b the adrenal tumors have been overlaid in green.
25767c01.8s Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasn malignant metastasis metastases primary lung imaging radiology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Bilateral Adrenal Metastases
The CTscan of the upper abdomen is from a patient with known lung carcinoma. The size, bilaterality and the heterogeneous appearance, particularly on the right are reminiscent of metastatic disease. In image b the adrenal tumors have been overlaid in green.
25767c01.8s Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasn malignant metastasis metastases primary lung imaging radiology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CTscan of the upper abdomen is from a patient with known lung carcinoma. The size, bilaterality and the heterogeneous appearance, particularly on the right are reminiscent of metastatic disease. In image b the adrenal tumors have been overlaid in green.
25767c01.8s Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasn malignant metastasis metastases primary lung imaging radiology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CTscan of the upper abdomen is from a patient with known lung carcinoma. The size, bilaterality and the heterogeneous appearance, particularly on the right are reminiscent of metastatic disease. In image b the adrenal tumors have been overlaid in green.
25767c01.8s Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasn malignant metastasis metastases primary lung imaging radiology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Bilateral Adrenal Metastases
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Bilateral Adrenal Metastases
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Metastatic Lung Nodules from Sigmoid Carcinoma
carcinoma. Multiple metastatic lesions are noted in the lungs of varying sizes but universally round. They have a soft tissue density, except for one lesion in the mid right lung that has a central region of air characteristic of a cavitation. This reflects central necrosis.
45139 Courtesy Ashley Davidoff MD 45132 45133 45134 45135 45136 45139 45141
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Metastatic Lung Nodules from Sigmoid Carcinoma
carcinoma. Multiple metastatic lesions are noted in the lungs of varying sizes but universally round. They have a soft tissue density, except for one lesion in the mid right lung that has a central region of air characteristic of a cavitation. This reflects central necrosis.
45139 Courtesy Ashley Davidoff MD 45132 45133 45134 45135 45136 45139 45141
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => carcinoma. Multiple metastatic lesions are noted in the lungs of varying sizes but universally round. They have a soft tissue density, except for one lesion in the mid right lung that has a central region of air characteristic of a cavitation. This reflects central necrosis.
45139 Courtesy Ashley Davidoff MD 45132 45133 45134 45135 45136 45139 45141
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => carcinoma. Multiple metastatic lesions are noted in the lungs of varying sizes but universally round. They have a soft tissue density, except for one lesion in the mid right lung that has a central region of air characteristic of a cavitation. This reflects central necrosis.
45139 Courtesy Ashley Davidoff MD 45132 45133 45134 45135 45136 45139 45141
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Metastatic Lung Nodules from Sigmoid Carcinoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Metastatic Lung Nodules from Sigmoid Carcinoma
)
https://beta.thecommonvein.net/wp-content/uploads/2023/06/45141.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45139.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45136.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45135.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45134.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45133.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/06/45132.jpg
http://www.thecommonvein.net/media/45139.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Diffuse Infiltration
The ultrasound of the liver is from a 72 year old patient with metastatic breast carcinoma. There is a region (overlaid in green ) that is hyperechoic and diffusely infiltrating without clear nor rounded borders. No obvious mass or nodule can be defined. This finding represents the less common infiltrating metastatic pattern, characteristically, but not exclusively, observed in patients with breast carcinoma.
code liver cancer malignancy malignant carcinoma metastasis infiltrating infiltrative US USscan ultrasound Courtsy Ashley DAvidoff MD copyright 2009 all rights reserved 24012c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Diffuse Infiltration
The ultrasound of the liver is from a 72 year old patient with metastatic breast carcinoma. There is a region (overlaid in green ) that is hyperechoic and diffusely infiltrating without clear nor rounded borders. No obvious mass or nodule can be defined. This finding represents the less common infiltrating metastatic pattern, characteristically, but not exclusively, observed in patients with breast carcinoma.
code liver cancer malignancy malignant carcinoma metastasis infiltrating infiltrative US USscan ultrasound Courtsy Ashley DAvidoff MD copyright 2009 all rights reserved 24012c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The ultrasound of the liver is from a 72 year old patient with metastatic breast carcinoma. There is a region (overlaid in green ) that is hyperechoic and diffusely infiltrating without clear nor rounded borders. No obvious mass or nodule can be defined. This finding represents the less common infiltrating metastatic pattern, characteristically, but not exclusively, observed in patients with breast carcinoma.
code liver cancer malignancy malignant carcinoma metastasis infiltrating infiltrative US USscan ultrasound Courtsy Ashley DAvidoff MD copyright 2009 all rights reserved 24012c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The ultrasound of the liver is from a 72 year old patient with metastatic breast carcinoma. There is a region (overlaid in green ) that is hyperechoic and diffusely infiltrating without clear nor rounded borders. No obvious mass or nodule can be defined. This finding represents the less common infiltrating metastatic pattern, characteristically, but not exclusively, observed in patients with breast carcinoma.
code liver cancer malignancy malignant carcinoma metastasis infiltrating infiltrative US USscan ultrasound Courtsy Ashley DAvidoff MD copyright 2009 all rights reserved 24012c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Diffuse Infiltration
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Diffuse Infiltration
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Diffuse Metastatic Infiltration in the Right Lobe
This gross specimen of the liver obtained from a post mortem was from a patient who had metastatic liver disease from adenocarcinoma of the pancreas. There are both nodular components and diffuse infiltrative components of metastatic disease. The right lobe is almost completely replaced by infiltrative disease while the left lobe is only mildly affected with discrete nodules.
code liver grosspathology mets metatstatic disease metastases metastasis space occupation Courtesy Ashley Davidoff MD copyright 2009 allrights reserved 02692b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Diffuse Metastatic Infiltration in the Right Lobe
This gross specimen of the liver obtained from a post mortem was from a patient who had metastatic liver disease from adenocarcinoma of the pancreas. There are both nodular components and diffuse infiltrative components of metastatic disease. The right lobe is almost completely replaced by infiltrative disease while the left lobe is only mildly affected with discrete nodules.
code liver grosspathology mets metatstatic disease metastases metastasis space occupation Courtesy Ashley Davidoff MD copyright 2009 allrights reserved 02692b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This gross specimen of the liver obtained from a post mortem was from a patient who had metastatic liver disease from adenocarcinoma of the pancreas. There are both nodular components and diffuse infiltrative components of metastatic disease. The right lobe is almost completely replaced by infiltrative disease while the left lobe is only mildly affected with discrete nodules.
code liver grosspathology mets metatstatic disease metastases metastasis space occupation Courtesy Ashley Davidoff MD copyright 2009 allrights reserved 02692b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This gross specimen of the liver obtained from a post mortem was from a patient who had metastatic liver disease from adenocarcinoma of the pancreas. There are both nodular components and diffuse infiltrative components of metastatic disease. The right lobe is almost completely replaced by infiltrative disease while the left lobe is only mildly affected with discrete nodules.
code liver grosspathology mets metatstatic disease metastases metastasis space occupation Courtesy Ashley Davidoff MD copyright 2009 allrights reserved 02692b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Diffuse Metastatic Infiltration in the Right Lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Diffuse Metastatic Infiltration in the Right Lobe
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pathological fracture – Lung Cancer with Metastasis to the Femur
cThis combination represents a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) in this patient with COPD. A metastatic lesion to the right femur is complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD. 32202c code lung cancer carrcinoma squamous cell carcinoma malignant metastases metastasis bone pathological fracture CXR CTscan grosspathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pathological fracture – Lung Cancer with Metastasis to the Femur
cThis combination represents a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) in this patient with COPD. A metastatic lesion to the right femur is complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD. 32202c code lung cancer carrcinoma squamous cell carcinoma malignant metastases metastasis bone pathological fracture CXR CTscan grosspathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => cThis combination represents a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) in this patient with COPD. A metastatic lesion to the right femur is complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD. 32202c code lung cancer carrcinoma squamous cell carcinoma malignant metastases metastasis bone pathological fracture CXR CTscan grosspathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => cThis combination represents a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) in this patient with COPD. A metastatic lesion to the right femur is complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD. 32202c code lung cancer carrcinoma squamous cell carcinoma malignant metastases metastasis bone pathological fracture CXR CTscan grosspathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Pathological fracture – Lung Cancer with Metastasis to the Femur
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Pathological fracture – Lung Cancer with Metastasis to the Femur
)
https://beta.thecommonvein.net/wp-content/uploads/2023/05/32202c.jpg
http://www.thecommonvein.net/lungs/wp-content/uploads/2021/11/32202c02.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Two Ulcerating Malignant Nodules in a Surgical Breast Specimen
In this surgical specimen of a mastectomy, two malignant ulcerating nodules have grown through the skin of the breast. The skin is the flesh colored bruised area and the two fungating nodules have grown through onto the surface.
13526b04 skin + fx ulcer ulceration dx carcinoma complicated by skin invasion grosspathology Courtesy Frank Reale MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Two Ulcerating Malignant Nodules in a Surgical Breast Specimen
In this surgical specimen of a mastectomy, two malignant ulcerating nodules have grown through the skin of the breast. The skin is the flesh colored bruised area and the two fungating nodules have grown through onto the surface.
13526b04 skin + fx ulcer ulceration dx carcinoma complicated by skin invasion grosspathology Courtesy Frank Reale MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this surgical specimen of a mastectomy, two malignant ulcerating nodules have grown through the skin of the breast. The skin is the flesh colored bruised area and the two fungating nodules have grown through onto the surface.
13526b04 skin + fx ulcer ulceration dx carcinoma complicated by skin invasion grosspathology Courtesy Frank Reale MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this surgical specimen of a mastectomy, two malignant ulcerating nodules have grown through the skin of the breast. The skin is the flesh colored bruised area and the two fungating nodules have grown through onto the surface.
13526b04 skin + fx ulcer ulceration dx carcinoma complicated by skin invasion grosspathology Courtesy Frank Reale MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Two Ulcerating Malignant Nodules in a Surgical Breast Specimen
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Two Ulcerating Malignant Nodules in a Surgical Breast Specimen
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Breast Cancer Invading the Skin Chest Wall and Heart
In this CT scan a patient with breast carcinoma is exemplified in image (a) with color overlays of the CT scan in b. The patient already has had a mastectomy for cancer and the prosthesis (orange) overlies the mastectomy site. A recurrence of the cancer has occurred (green) and it has invaded the skin and is exposed on the outside between the involved skin (pink )which is thickened either due to radiation and or the recurrent cancer. The break in the skin (green exposed through the pink) represents an ulcerating mass. The tumor also invades through the chest wall and has started to erode the pericardium (yellow).
78387c breast skin heart pericardium invasion space occupation prosthesis CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Breast Cancer Invading the Skin Chest Wall and Heart
In this CT scan a patient with breast carcinoma is exemplified in image (a) with color overlays of the CT scan in b. The patient already has had a mastectomy for cancer and the prosthesis (orange) overlies the mastectomy site. A recurrence of the cancer has occurred (green) and it has invaded the skin and is exposed on the outside between the involved skin (pink )which is thickened either due to radiation and or the recurrent cancer. The break in the skin (green exposed through the pink) represents an ulcerating mass. The tumor also invades through the chest wall and has started to erode the pericardium (yellow).
78387c breast skin heart pericardium invasion space occupation prosthesis CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this CT scan a patient with breast carcinoma is exemplified in image (a) with color overlays of the CT scan in b. The patient already has had a mastectomy for cancer and the prosthesis (orange) overlies the mastectomy site. A recurrence of the cancer has occurred (green) and it has invaded the skin and is exposed on the outside between the involved skin (pink )which is thickened either due to radiation and or the recurrent cancer. The break in the skin (green exposed through the pink) represents an ulcerating mass. The tumor also invades through the chest wall and has started to erode the pericardium (yellow).
78387c breast skin heart pericardium invasion space occupation prosthesis CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this CT scan a patient with breast carcinoma is exemplified in image (a) with color overlays of the CT scan in b. The patient already has had a mastectomy for cancer and the prosthesis (orange) overlies the mastectomy site. A recurrence of the cancer has occurred (green) and it has invaded the skin and is exposed on the outside between the involved skin (pink )which is thickened either due to radiation and or the recurrent cancer. The break in the skin (green exposed through the pink) represents an ulcerating mass. The tumor also invades through the chest wall and has started to erode the pericardium (yellow).
78387c breast skin heart pericardium invasion space occupation prosthesis CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Breast Cancer Invading the Skin Chest Wall and Heart
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Breast Cancer Invading the Skin Chest Wall and Heart
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Renal Cell Carcinoma Metastasis with Edema
The long orange line from front to back of the brain represents the middle and the small horizontal orange line shows midline shift of about 4mm. In this instance steroids would help reduce the edema and would help limit the pressure caused by the edema.
77300c01 bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Renal Cell Carcinoma Metastasis with Edema
The long orange line from front to back of the brain represents the middle and the small horizontal orange line shows midline shift of about 4mm. In this instance steroids would help reduce the edema and would help limit the pressure caused by the edema.
77300c01 bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The long orange line from front to back of the brain represents the middle and the small horizontal orange line shows midline shift of about 4mm. In this instance steroids would help reduce the edema and would help limit the pressure caused by the edema.
77300c01 bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The long orange line from front to back of the brain represents the middle and the small horizontal orange line shows midline shift of about 4mm. In this instance steroids would help reduce the edema and would help limit the pressure caused by the edema.
77300c01 bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Renal Cell Carcinoma Metastasis with Edema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Renal Cell Carcinoma Metastasis with Edema
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Renal Cell Carcinoma Metastasis with Edema
In this MRI image of the brain there is a metastatic nodule (green) that measures just over 2cms, but it has created a ring of edema which is causing mass effect by space occupation by a volume that is at least 3 times its size. (yellow). This has resulted in subtle midline shift.
77300c bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Renal Cell Carcinoma Metastasis with Edema
In this MRI image of the brain there is a metastatic nodule (green) that measures just over 2cms, but it has created a ring of edema which is causing mass effect by space occupation by a volume that is at least 3 times its size. (yellow). This has resulted in subtle midline shift.
77300c bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this MRI image of the brain there is a metastatic nodule (green) that measures just over 2cms, but it has created a ring of edema which is causing mass effect by space occupation by a volume that is at least 3 times its size. (yellow). This has resulted in subtle midline shift.
77300c bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this MRI image of the brain there is a metastatic nodule (green) that measures just over 2cms, but it has created a ring of edema which is causing mass effect by space occupation by a volume that is at least 3 times its size. (yellow). This has resulted in subtle midline shift.
77300c bilateral RCC mets to lung hemorrhagic mets to brain mass edema mass effect midline shift edema MRI T2 weighted Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Renal Cell Carcinoma Metastasis with Edema
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Renal Cell Carcinoma Metastasis with Edema
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Liver and Single Group of Cancer Cells
These two cases represent the microscopic events described in the macroscopic examples above. The left image shows normal liver cords at high power, while the image on the right shows slightly lower power of the liver cords in pink, and a blue, rounded, space occupying metastasis.
13445 11440 liver cords sinusoids hepatocytes Kuppfer cells TCV concepts histology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Liver and Single Group of Cancer Cells
These two cases represent the microscopic events described in the macroscopic examples above. The left image shows normal liver cords at high power, while the image on the right shows slightly lower power of the liver cords in pink, and a blue, rounded, space occupying metastasis.
13445 11440 liver cords sinusoids hepatocytes Kuppfer cells TCV concepts histology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These two cases represent the microscopic events described in the macroscopic examples above. The left image shows normal liver cords at high power, while the image on the right shows slightly lower power of the liver cords in pink, and a blue, rounded, space occupying metastasis.
13445 11440 liver cords sinusoids hepatocytes Kuppfer cells TCV concepts histology Courtesy Barbara Banner MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These two cases represent the microscopic events described in the macroscopic examples above. The left image shows normal liver cords at high power, while the image on the right shows slightly lower power of the liver cords in pink, and a blue, rounded, space occupying metastasis.
13445 11440 liver cords sinusoids hepatocytes Kuppfer cells TCV concepts histology Courtesy Barbara Banner MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Liver and Single Group of Cancer Cells
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Liver and Single Group of Cancer Cells
)
https://beta.thecommonvein.net/wp-content/uploads/2023/09/13445.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/05/11440.jpg
http://www.thecommonvein.net/media/13445_1.jpg http://www.thecommonvein.net/media/11440.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Liver – (left) and Cancer in the Liver (right)
The liver on the left is normal except for gallstones in the gallbladder. Gallstones are squatters but they usually do not have aggressive tendencies unless they block the outflow of bile. The liver shown in the right image is from a patient who succumbed to metastatic pancreatic carcinoma. The normal liver cells have been displaced and have been overridden by metastatic squatters. The metastases have contributed to the demise of the patient by their relentless displacement of normal tissue, causing progressive impairment of function.
13456 13448b01 liver normal anatomy gallbladder stones cholelithiasis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Liver – (left) and Cancer in the Liver (right)
The liver on the left is normal except for gallstones in the gallbladder. Gallstones are squatters but they usually do not have aggressive tendencies unless they block the outflow of bile. The liver shown in the right image is from a patient who succumbed to metastatic pancreatic carcinoma. The normal liver cells have been displaced and have been overridden by metastatic squatters. The metastases have contributed to the demise of the patient by their relentless displacement of normal tissue, causing progressive impairment of function.
13456 13448b01 liver normal anatomy gallbladder stones cholelithiasis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The liver on the left is normal except for gallstones in the gallbladder. Gallstones are squatters but they usually do not have aggressive tendencies unless they block the outflow of bile. The liver shown in the right image is from a patient who succumbed to metastatic pancreatic carcinoma. The normal liver cells have been displaced and have been overridden by metastatic squatters. The metastases have contributed to the demise of the patient by their relentless displacement of normal tissue, causing progressive impairment of function.
13456 13448b01 liver normal anatomy gallbladder stones cholelithiasis grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The liver on the left is normal except for gallstones in the gallbladder. Gallstones are squatters but they usually do not have aggressive tendencies unless they block the outflow of bile. The liver shown in the right image is from a patient who succumbed to metastatic pancreatic carcinoma. The normal liver cells have been displaced and have been overridden by metastatic squatters. The metastases have contributed to the demise of the patient by their relentless displacement of normal tissue, causing progressive impairment of function.
13456 13448b01 liver normal anatomy gallbladder stones cholelithiasis grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Liver – (left) and Cancer in the Liver (right)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Liver – (left) and Cancer in the Liver (right)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Battleground
The reenactment of the war that was fought between the American revolutionaries seen here, and the loyalists to the English king depicts the battlefield in the fields of Lincoln Massachusetts in 1775. The concept of cancerous tissue vs normal in a battlefield has parallels . Left untreated the cancer is victorious. The normal well meaning tissues need assistance of clever therapies to attain victory. Left unchecked the cancer is inevitably victorious.
84022p.800 baby Lincoln Massachusetts Minuteman State PArk Reenactment of the days of the Revolution America circa 1775 men army gun horses Boston Davidoff photography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Battleground
The reenactment of the war that was fought between the American revolutionaries seen here, and the loyalists to the English king depicts the battlefield in the fields of Lincoln Massachusetts in 1775. The concept of cancerous tissue vs normal in a battlefield has parallels . Left untreated the cancer is victorious. The normal well meaning tissues need assistance of clever therapies to attain victory. Left unchecked the cancer is inevitably victorious.
84022p.800 baby Lincoln Massachusetts Minuteman State PArk Reenactment of the days of the Revolution America circa 1775 men army gun horses Boston Davidoff photography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The reenactment of the war that was fought between the American revolutionaries seen here, and the loyalists to the English king depicts the battlefield in the fields of Lincoln Massachusetts in 1775. The concept of cancerous tissue vs normal in a battlefield has parallels . Left untreated the cancer is victorious. The normal well meaning tissues need assistance of clever therapies to attain victory. Left unchecked the cancer is inevitably victorious.
84022p.800 baby Lincoln Massachusetts Minuteman State PArk Reenactment of the days of the Revolution America circa 1775 men army gun horses Boston Davidoff photography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The reenactment of the war that was fought between the American revolutionaries seen here, and the loyalists to the English king depicts the battlefield in the fields of Lincoln Massachusetts in 1775. The concept of cancerous tissue vs normal in a battlefield has parallels . Left untreated the cancer is victorious. The normal well meaning tissues need assistance of clever therapies to attain victory. Left unchecked the cancer is inevitably victorious.
84022p.800 baby Lincoln Massachusetts Minuteman State PArk Reenactment of the days of the Revolution America circa 1775 men army gun horses Boston Davidoff photography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Battleground
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Battleground
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Battleground – Tumor vs Healthy Tissue
The histopathology of a surgically resected hepatic metastasis from a primary colon carcinoma shows a mucinous secreting tumor at the bottom of the image labeled “advancing tumor”. The cellular detail is not well seen in the low power view but the columnar epithelial nature, hyperchromicity, and bizarre appearance of squatter tissue in the liver are recognized as malignant characteristics. The white spaces in between the cellular structure, represents mucin in the tumor. The edge of the tumor shows a rounded and aggressive push into the liver where the injured liver in the battlefield is recognized as compressed normal liver with linear areas of hemorrhage evidenced by a curvilinear line at 11 and 12 oclock of increased area of redness representing extravascular red cells (“layer of “injured liver”). The uppermost layer represents the normal liver which at this time looks healthy but is in jeopardy.
The The radial red spokes seen at the edge of the tumor are artifacts of preparation but are indicators of the direction of the battle.
03028b01.81s Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Battleground – Tumor vs Healthy Tissue
The histopathology of a surgically resected hepatic metastasis from a primary colon carcinoma shows a mucinous secreting tumor at the bottom of the image labeled “advancing tumor”. The cellular detail is not well seen in the low power view but the columnar epithelial nature, hyperchromicity, and bizarre appearance of squatter tissue in the liver are recognized as malignant characteristics. The white spaces in between the cellular structure, represents mucin in the tumor. The edge of the tumor shows a rounded and aggressive push into the liver where the injured liver in the battlefield is recognized as compressed normal liver with linear areas of hemorrhage evidenced by a curvilinear line at 11 and 12 oclock of increased area of redness representing extravascular red cells (“layer of “injured liver”). The uppermost layer represents the normal liver which at this time looks healthy but is in jeopardy.
The The radial red spokes seen at the edge of the tumor are artifacts of preparation but are indicators of the direction of the battle.
03028b01.81s Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The histopathology of a surgically resected hepatic metastasis from a primary colon carcinoma shows a mucinous secreting tumor at the bottom of the image labeled “advancing tumor”. The cellular detail is not well seen in the low power view but the columnar epithelial nature, hyperchromicity, and bizarre appearance of squatter tissue in the liver are recognized as malignant characteristics. The white spaces in between the cellular structure, represents mucin in the tumor. The edge of the tumor shows a rounded and aggressive push into the liver where the injured liver in the battlefield is recognized as compressed normal liver with linear areas of hemorrhage evidenced by a curvilinear line at 11 and 12 oclock of increased area of redness representing extravascular red cells (“layer of “injured liver”). The uppermost layer represents the normal liver which at this time looks healthy but is in jeopardy.
The The radial red spokes seen at the edge of the tumor are artifacts of preparation but are indicators of the direction of the battle.
03028b01.81s Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The histopathology of a surgically resected hepatic metastasis from a primary colon carcinoma shows a mucinous secreting tumor at the bottom of the image labeled “advancing tumor”. The cellular detail is not well seen in the low power view but the columnar epithelial nature, hyperchromicity, and bizarre appearance of squatter tissue in the liver are recognized as malignant characteristics. The white spaces in between the cellular structure, represents mucin in the tumor. The edge of the tumor shows a rounded and aggressive push into the liver where the injured liver in the battlefield is recognized as compressed normal liver with linear areas of hemorrhage evidenced by a curvilinear line at 11 and 12 oclock of increased area of redness representing extravascular red cells (“layer of “injured liver”). The uppermost layer represents the normal liver which at this time looks healthy but is in jeopardy.
The The radial red spokes seen at the edge of the tumor are artifacts of preparation but are indicators of the direction of the battle.
03028b01.81s Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Battleground – Tumor vs Healthy Tissue
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Battleground – Tumor vs Healthy Tissue
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Nicotene
These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d code RS pulmonary lung alveolus smake amoking cigarettes nicotene accessory pathology histopathology drawing
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Nicotene
These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d code RS pulmonary lung alveolus smake amoking cigarettes nicotene accessory pathology histopathology drawing
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d code RS pulmonary lung alveolus smake amoking cigarettes nicotene accessory pathology histopathology drawing
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These diseases are all about cigarettes and the garbage that they deposit in our lungs.
Courtesy Ashley Davidoff MD. 32646d code RS pulmonary lung alveolus smake amoking cigarettes nicotene accessory pathology histopathology drawing
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Nicotene
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Nicotene
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Infiltrative and Nodular Form
The gross and histopathological specimens are from the autopsy of a patient who died of breast carcinoma that was metastatic to the liver. The right lobe of the liver shows two patterns of metastases. In the posterior aspect of the right lobe of the liver, there is diffuse disease, and in the anterior aspect there are innumerable nodules of varying sizes. The left lobe is relatively spared, and the pattern is of a nodular nature. The low power histopathological section shows a diffuse infiltrate of hyperchromatic malignant nuclii in the bottom of the image and relatively normal liver in the upper portion.
03034c.8s code liver metastases metastasis breast primary cancer malignant space occupation infiltration infiltrative pattern right lobe left lobe grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved GW question
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Infiltrative and Nodular Form
The gross and histopathological specimens are from the autopsy of a patient who died of breast carcinoma that was metastatic to the liver. The right lobe of the liver shows two patterns of metastases. In the posterior aspect of the right lobe of the liver, there is diffuse disease, and in the anterior aspect there are innumerable nodules of varying sizes. The left lobe is relatively spared, and the pattern is of a nodular nature. The low power histopathological section shows a diffuse infiltrate of hyperchromatic malignant nuclii in the bottom of the image and relatively normal liver in the upper portion.
03034c.8s code liver metastases metastasis breast primary cancer malignant space occupation infiltration infiltrative pattern right lobe left lobe grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved GW question
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The gross and histopathological specimens are from the autopsy of a patient who died of breast carcinoma that was metastatic to the liver. The right lobe of the liver shows two patterns of metastases. In the posterior aspect of the right lobe of the liver, there is diffuse disease, and in the anterior aspect there are innumerable nodules of varying sizes. The left lobe is relatively spared, and the pattern is of a nodular nature. The low power histopathological section shows a diffuse infiltrate of hyperchromatic malignant nuclii in the bottom of the image and relatively normal liver in the upper portion.
03034c.8s code liver metastases metastasis breast primary cancer malignant space occupation infiltration infiltrative pattern right lobe left lobe grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved GW question
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The gross and histopathological specimens are from the autopsy of a patient who died of breast carcinoma that was metastatic to the liver. The right lobe of the liver shows two patterns of metastases. In the posterior aspect of the right lobe of the liver, there is diffuse disease, and in the anterior aspect there are innumerable nodules of varying sizes. The left lobe is relatively spared, and the pattern is of a nodular nature. The low power histopathological section shows a diffuse infiltrate of hyperchromatic malignant nuclii in the bottom of the image and relatively normal liver in the upper portion.
03034c.8s code liver metastases metastasis breast primary cancer malignant space occupation infiltration infiltrative pattern right lobe left lobe grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved GW question
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Infiltrative and Nodular Form
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Infiltrative and Nodular Form
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Primary Duodenal Cancer- Metastases to the Liver
The post mortem specimen (a) shows a 2cms primary duodenal carcinoma (white arrow) with extensive nodular hepatic metastases occupying 80% of the liver. (b) In image c, the metastasis reflects an overall a blue hue caused by the increased nuclear presence. The image reveals an irregular and advancing threat on the normal liver. The higher power view in d, shows a rind of compressed liver that is in the process of destruction and hemorrhage (red patches) in the tumor, in the border, as well as in the normal liver. This image is reminiscent of an advancing enemy in a battlefield with victory apparent for the aggressor.
02643c03.8s code liver duodenum adenocarcinoma metastases metastasis cancer malignant space occupation pressure atrophy death grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Primary Duodenal Cancer- Metastases to the Liver
The post mortem specimen (a) shows a 2cms primary duodenal carcinoma (white arrow) with extensive nodular hepatic metastases occupying 80% of the liver. (b) In image c, the metastasis reflects an overall a blue hue caused by the increased nuclear presence. The image reveals an irregular and advancing threat on the normal liver. The higher power view in d, shows a rind of compressed liver that is in the process of destruction and hemorrhage (red patches) in the tumor, in the border, as well as in the normal liver. This image is reminiscent of an advancing enemy in a battlefield with victory apparent for the aggressor.
02643c03.8s code liver duodenum adenocarcinoma metastases metastasis cancer malignant space occupation pressure atrophy death grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The post mortem specimen (a) shows a 2cms primary duodenal carcinoma (white arrow) with extensive nodular hepatic metastases occupying 80% of the liver. (b) In image c, the metastasis reflects an overall a blue hue caused by the increased nuclear presence. The image reveals an irregular and advancing threat on the normal liver. The higher power view in d, shows a rind of compressed liver that is in the process of destruction and hemorrhage (red patches) in the tumor, in the border, as well as in the normal liver. This image is reminiscent of an advancing enemy in a battlefield with victory apparent for the aggressor.
02643c03.8s code liver duodenum adenocarcinoma metastases metastasis cancer malignant space occupation pressure atrophy death grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The post mortem specimen (a) shows a 2cms primary duodenal carcinoma (white arrow) with extensive nodular hepatic metastases occupying 80% of the liver. (b) In image c, the metastasis reflects an overall a blue hue caused by the increased nuclear presence. The image reveals an irregular and advancing threat on the normal liver. The higher power view in d, shows a rind of compressed liver that is in the process of destruction and hemorrhage (red patches) in the tumor, in the border, as well as in the normal liver. This image is reminiscent of an advancing enemy in a battlefield with victory apparent for the aggressor.
02643c03.8s code liver duodenum adenocarcinoma metastases metastasis cancer malignant space occupation pressure atrophy death grosspathology histopathology Courtesy Ashley DAvidoff MD copyright 2009 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Primary Duodenal Cancer- Metastases to the Liver
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Primary Duodenal Cancer- Metastases to the Liver
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Metastatic Leiomyosarcoma
The collage consists of a CT scan (a) showing a focal well circumscribed low density liver lesion. Biopsy of this lesion yielded the histopathological specimen (b) that shows hyperchromatic nuclii and spindle shaped cells, in a swirling pattern characteristic of leiomyosarcoma. The cytological aspirate (c) shows spindle shaped nuclii with pleomorphism and hyperchromicity.
code malignant cancer sarcoma histopathology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 03057c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Metastatic Leiomyosarcoma
The collage consists of a CT scan (a) showing a focal well circumscribed low density liver lesion. Biopsy of this lesion yielded the histopathological specimen (b) that shows hyperchromatic nuclii and spindle shaped cells, in a swirling pattern characteristic of leiomyosarcoma. The cytological aspirate (c) shows spindle shaped nuclii with pleomorphism and hyperchromicity.
code malignant cancer sarcoma histopathology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 03057c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The collage consists of a CT scan (a) showing a focal well circumscribed low density liver lesion. Biopsy of this lesion yielded the histopathological specimen (b) that shows hyperchromatic nuclii and spindle shaped cells, in a swirling pattern characteristic of leiomyosarcoma. The cytological aspirate (c) shows spindle shaped nuclii with pleomorphism and hyperchromicity.
code malignant cancer sarcoma histopathology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 03057c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The collage consists of a CT scan (a) showing a focal well circumscribed low density liver lesion. Biopsy of this lesion yielded the histopathological specimen (b) that shows hyperchromatic nuclii and spindle shaped cells, in a swirling pattern characteristic of leiomyosarcoma. The cytological aspirate (c) shows spindle shaped nuclii with pleomorphism and hyperchromicity.
code malignant cancer sarcoma histopathology CTscan Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 03057c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Metastatic Leiomyosarcoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Metastatic Leiomyosarcoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Colon Carcinoma
The low power view of the malignant colonic mucosa shows somewhat normal mucosa to the left of the image, but ringed in purple in image b is a group of renegade cells that has broken away from the orderly “test tube” format and has advanced into the submucosa. Although it is difficult to evaluate accurately, very little cytoplasm can be appreciated and the overall “blueness” of the mass suggests hyperchromicity.
02746c02.8s The low power view of the malignant colonic mucosa shows basicar cells that have hyperchromicity, lack cytoplasm and have invaded into the submucosa code colon carcinoma malignant primary histopathology Courtesy Barbara Banner MD copyright 2009 allrights reserved GW question
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Colon Carcinoma
The low power view of the malignant colonic mucosa shows somewhat normal mucosa to the left of the image, but ringed in purple in image b is a group of renegade cells that has broken away from the orderly “test tube” format and has advanced into the submucosa. Although it is difficult to evaluate accurately, very little cytoplasm can be appreciated and the overall “blueness” of the mass suggests hyperchromicity.
02746c02.8s The low power view of the malignant colonic mucosa shows basicar cells that have hyperchromicity, lack cytoplasm and have invaded into the submucosa code colon carcinoma malignant primary histopathology Courtesy Barbara Banner MD copyright 2009 allrights reserved GW question
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The low power view of the malignant colonic mucosa shows somewhat normal mucosa to the left of the image, but ringed in purple in image b is a group of renegade cells that has broken away from the orderly “test tube” format and has advanced into the submucosa. Although it is difficult to evaluate accurately, very little cytoplasm can be appreciated and the overall “blueness” of the mass suggests hyperchromicity.
02746c02.8s The low power view of the malignant colonic mucosa shows basicar cells that have hyperchromicity, lack cytoplasm and have invaded into the submucosa code colon carcinoma malignant primary histopathology Courtesy Barbara Banner MD copyright 2009 allrights reserved GW question
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The low power view of the malignant colonic mucosa shows somewhat normal mucosa to the left of the image, but ringed in purple in image b is a group of renegade cells that has broken away from the orderly “test tube” format and has advanced into the submucosa. Although it is difficult to evaluate accurately, very little cytoplasm can be appreciated and the overall “blueness” of the mass suggests hyperchromicity.
02746c02.8s The low power view of the malignant colonic mucosa shows basicar cells that have hyperchromicity, lack cytoplasm and have invaded into the submucosa code colon carcinoma malignant primary histopathology Courtesy Barbara Banner MD copyright 2009 allrights reserved GW question
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Colon Carcinoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Colon Carcinoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Colonic Mucosa
This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, “test tube”-like arrangement of the straight tubular glands which comprise the colonic crypts. The nuclii are seen in orderly fashion at the base of the columnar cell as dark purple dots while the cytoplasm is seen with vacuoles of mucin reflecting a nuclear cytoplasmic ratio of 1:4 or even 1:6. The underlying submucosa is not seen in this image although submucosa between the crypts is noted.
12860 Normal Colon Mucosa. This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, ?test tube?-like arrangement of the straight tubular glands which comprise the colonic crypts. colon large bowel mucosa submucosa crypts histology Courtesy Barbara Banner MD 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Colonic Mucosa
This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, “test tube”-like arrangement of the straight tubular glands which comprise the colonic crypts. The nuclii are seen in orderly fashion at the base of the columnar cell as dark purple dots while the cytoplasm is seen with vacuoles of mucin reflecting a nuclear cytoplasmic ratio of 1:4 or even 1:6. The underlying submucosa is not seen in this image although submucosa between the crypts is noted.
12860 Normal Colon Mucosa. This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, ?test tube?-like arrangement of the straight tubular glands which comprise the colonic crypts. colon large bowel mucosa submucosa crypts histology Courtesy Barbara Banner MD 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, “test tube”-like arrangement of the straight tubular glands which comprise the colonic crypts. The nuclii are seen in orderly fashion at the base of the columnar cell as dark purple dots while the cytoplasm is seen with vacuoles of mucin reflecting a nuclear cytoplasmic ratio of 1:4 or even 1:6. The underlying submucosa is not seen in this image although submucosa between the crypts is noted.
12860 Normal Colon Mucosa. This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, ?test tube?-like arrangement of the straight tubular glands which comprise the colonic crypts. colon large bowel mucosa submucosa crypts histology Courtesy Barbara Banner MD 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, “test tube”-like arrangement of the straight tubular glands which comprise the colonic crypts. The nuclii are seen in orderly fashion at the base of the columnar cell as dark purple dots while the cytoplasm is seen with vacuoles of mucin reflecting a nuclear cytoplasmic ratio of 1:4 or even 1:6. The underlying submucosa is not seen in this image although submucosa between the crypts is noted.
12860 Normal Colon Mucosa. This is a low power photo micrograph of normal colon mucosa illustrating extremely orderly, rigid, ?test tube?-like arrangement of the straight tubular glands which comprise the colonic crypts. colon large bowel mucosa submucosa crypts histology Courtesy Barbara Banner MD 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Colonic Mucosa
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Colonic Mucosa
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Malignant Liver Cells
In this cytopathology specimen the nuclear cytoplasmic ratio is closer to 1:1 and sometimes as in the cell in the lower right hand corner the nucleus is 4 or 5 times larger than the cytoplasm. This appearance is characteristic of malignant tissue. This is an example of a hepatocellular carcinoma.
13447 liver HCC hepatocellular carcinoma cytopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Malignant Liver Cells
In this cytopathology specimen the nuclear cytoplasmic ratio is closer to 1:1 and sometimes as in the cell in the lower right hand corner the nucleus is 4 or 5 times larger than the cytoplasm. This appearance is characteristic of malignant tissue. This is an example of a hepatocellular carcinoma.
13447 liver HCC hepatocellular carcinoma cytopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this cytopathology specimen the nuclear cytoplasmic ratio is closer to 1:1 and sometimes as in the cell in the lower right hand corner the nucleus is 4 or 5 times larger than the cytoplasm. This appearance is characteristic of malignant tissue. This is an example of a hepatocellular carcinoma.
13447 liver HCC hepatocellular carcinoma cytopathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this cytopathology specimen the nuclear cytoplasmic ratio is closer to 1:1 and sometimes as in the cell in the lower right hand corner the nucleus is 4 or 5 times larger than the cytoplasm. This appearance is characteristic of malignant tissue. This is an example of a hepatocellular carcinoma.
13447 liver HCC hepatocellular carcinoma cytopathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Malignant Liver Cells
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Malignant Liver Cells
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Liver Cells
The volume ratio of nucleus to cytoplasm is 1:4 or even 1:6 and the cytoplasm is a light pink (eosinophillic) The shape of the cell is polygonal.
13440 liver hepatocytes cells cytology histology normal 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Liver Cells
The volume ratio of nucleus to cytoplasm is 1:4 or even 1:6 and the cytoplasm is a light pink (eosinophillic) The shape of the cell is polygonal.
13440 liver hepatocytes cells cytology histology normal 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The volume ratio of nucleus to cytoplasm is 1:4 or even 1:6 and the cytoplasm is a light pink (eosinophillic) The shape of the cell is polygonal.
13440 liver hepatocytes cells cytology histology normal 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The volume ratio of nucleus to cytoplasm is 1:4 or even 1:6 and the cytoplasm is a light pink (eosinophillic) The shape of the cell is polygonal.
13440 liver hepatocytes cells cytology histology normal 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Liver Cells
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Liver Cells
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Abnormal Programming Multiplication and Space Occupation
The image represents the evolution of a single cancer cell (a) that fails to conform to the normal time cycle. In image a, the normal columnar mucosa is composed of rectangular cells supported by a thin purple basement membrane. One cell becomes aberrant, and is characterized by a large blue nucleus, scanty cytoplasm and a a change in it shape and overall appearance. The cell grows, multiplies, (b,c,d) and then invades the space of other parts of the tissue like the submucocsa (yellow) and muscular layer (maroon) in e and finally the serosal layer in f(outer white layer).
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198fc02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Abnormal Programming Multiplication and Space Occupation
The image represents the evolution of a single cancer cell (a) that fails to conform to the normal time cycle. In image a, the normal columnar mucosa is composed of rectangular cells supported by a thin purple basement membrane. One cell becomes aberrant, and is characterized by a large blue nucleus, scanty cytoplasm and a a change in it shape and overall appearance. The cell grows, multiplies, (b,c,d) and then invades the space of other parts of the tissue like the submucocsa (yellow) and muscular layer (maroon) in e and finally the serosal layer in f(outer white layer).
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198fc02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The image represents the evolution of a single cancer cell (a) that fails to conform to the normal time cycle. In image a, the normal columnar mucosa is composed of rectangular cells supported by a thin purple basement membrane. One cell becomes aberrant, and is characterized by a large blue nucleus, scanty cytoplasm and a a change in it shape and overall appearance. The cell grows, multiplies, (b,c,d) and then invades the space of other parts of the tissue like the submucocsa (yellow) and muscular layer (maroon) in e and finally the serosal layer in f(outer white layer).
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198fc02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The image represents the evolution of a single cancer cell (a) that fails to conform to the normal time cycle. In image a, the normal columnar mucosa is composed of rectangular cells supported by a thin purple basement membrane. One cell becomes aberrant, and is characterized by a large blue nucleus, scanty cytoplasm and a a change in it shape and overall appearance. The cell grows, multiplies, (b,c,d) and then invades the space of other parts of the tissue like the submucocsa (yellow) and muscular layer (maroon) in e and finally the serosal layer in f(outer white layer).
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198fc02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Abnormal Programming Multiplication and Space Occupation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Abnormal Programming Multiplication and Space Occupation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
A Cancer Cell – Aberrant Sense of Time
The image represents the life of a single set of columnar cells showing a progression of generations as the cell lives dies and is regenerated. The orange secretions of the cell are seen in the background of the pink cytoplasm and the purple nucleus. The nucleus of the newest generation and cell is seen as a clock that has become distorted causing time to become disordered. This is the forerunner of a malignant process.
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198j03s.81s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
A Cancer Cell – Aberrant Sense of Time
The image represents the life of a single set of columnar cells showing a progression of generations as the cell lives dies and is regenerated. The orange secretions of the cell are seen in the background of the pink cytoplasm and the purple nucleus. The nucleus of the newest generation and cell is seen as a clock that has become distorted causing time to become disordered. This is the forerunner of a malignant process.
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198j03s.81s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The image represents the life of a single set of columnar cells showing a progression of generations as the cell lives dies and is regenerated. The orange secretions of the cell are seen in the background of the pink cytoplasm and the purple nucleus. The nucleus of the newest generation and cell is seen as a clock that has become distorted causing time to become disordered. This is the forerunner of a malignant process.
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198j03s.81s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The image represents the life of a single set of columnar cells showing a progression of generations as the cell lives dies and is regenerated. The orange secretions of the cell are seen in the background of the pink cytoplasm and the purple nucleus. The nucleus of the newest generation and cell is seen as a clock that has become distorted causing time to become disordered. This is the forerunner of a malignant process.
histology time malignancy cancer columnar cell histopathology Davidoff art copyright 2009 all rights reserved 85198j03s.81s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
A Cancer Cell – Aberrant Sense of Time
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A Cancer Cell – Aberrant Sense of Time
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Malignant Process Left Unchecked
The nature of malignancy is outlined in the evolution of a malignant cell in the gastrointestinal tract. The bowel consists of 4 basic layers with an inner epithelial layer (pink) a submucosal layer (yellow), a muscular layer (red) and an outer serosal or adventitial layer (blue). The bowel lumen lies between two layers of bowel wall (black and white). In image 1, a single cell of the mucosa seen in the background of white, becomes “aberrant” and plays no role in the function of the mucosa. It multiplies and its progeny occupies a larger space (image 2). As it continues to grow it breaks through the mucosa and into the submucosa (yellow) and muscularis (red) in 3. Its uninhibited growth into the veins (blue) and lymph nodes (orange) results in metastatic disease to secondary sites. In the meantime it continues to invade locally encircling the intestinal tract, narrowing the bowel lumen, and eventually causing obstruction of the tract. (image 5).
Courtesy Ashley Davidoff MD. 32336c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Malignant Process Left Unchecked
The nature of malignancy is outlined in the evolution of a malignant cell in the gastrointestinal tract. The bowel consists of 4 basic layers with an inner epithelial layer (pink) a submucosal layer (yellow), a muscular layer (red) and an outer serosal or adventitial layer (blue). The bowel lumen lies between two layers of bowel wall (black and white). In image 1, a single cell of the mucosa seen in the background of white, becomes “aberrant” and plays no role in the function of the mucosa. It multiplies and its progeny occupies a larger space (image 2). As it continues to grow it breaks through the mucosa and into the submucosa (yellow) and muscularis (red) in 3. Its uninhibited growth into the veins (blue) and lymph nodes (orange) results in metastatic disease to secondary sites. In the meantime it continues to invade locally encircling the intestinal tract, narrowing the bowel lumen, and eventually causing obstruction of the tract. (image 5).
Courtesy Ashley Davidoff MD. 32336c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The nature of malignancy is outlined in the evolution of a malignant cell in the gastrointestinal tract. The bowel consists of 4 basic layers with an inner epithelial layer (pink) a submucosal layer (yellow), a muscular layer (red) and an outer serosal or adventitial layer (blue). The bowel lumen lies between two layers of bowel wall (black and white). In image 1, a single cell of the mucosa seen in the background of white, becomes “aberrant” and plays no role in the function of the mucosa. It multiplies and its progeny occupies a larger space (image 2). As it continues to grow it breaks through the mucosa and into the submucosa (yellow) and muscularis (red) in 3. Its uninhibited growth into the veins (blue) and lymph nodes (orange) results in metastatic disease to secondary sites. In the meantime it continues to invade locally encircling the intestinal tract, narrowing the bowel lumen, and eventually causing obstruction of the tract. (image 5).
Courtesy Ashley Davidoff MD. 32336c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The nature of malignancy is outlined in the evolution of a malignant cell in the gastrointestinal tract. The bowel consists of 4 basic layers with an inner epithelial layer (pink) a submucosal layer (yellow), a muscular layer (red) and an outer serosal or adventitial layer (blue). The bowel lumen lies between two layers of bowel wall (black and white). In image 1, a single cell of the mucosa seen in the background of white, becomes “aberrant” and plays no role in the function of the mucosa. It multiplies and its progeny occupies a larger space (image 2). As it continues to grow it breaks through the mucosa and into the submucosa (yellow) and muscularis (red) in 3. Its uninhibited growth into the veins (blue) and lymph nodes (orange) results in metastatic disease to secondary sites. In the meantime it continues to invade locally encircling the intestinal tract, narrowing the bowel lumen, and eventually causing obstruction of the tract. (image 5).
Courtesy Ashley Davidoff MD. 32336c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Malignant Process Left Unchecked
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Malignant Process Left Unchecked
)