Dermoid/Teratoma
Elisa Flower MD and Asim Mian MD
The Common Vein Copyright 2010
Definition
A dermoid is considered a congenital lesion and like epidermoids are thought be caused by abnormal location of surface ectoderm which may be a result of abnormal migration during neural tube closure. They are usually located in the midline and when they are intracranial they are frequently within the posterior fossa in the cisterna magna, fourth ventricle and prepontine cistern. They may also be located in a supratentorial location, usually in the suprasellar region. They are a common cause of orbital lesions in young patients as well.
They may grow slowly over time due to the accumulation of desquamated debris and gland products. Dermoids may also rupture which can result in chemical meningitis or other conditions such as seizure or hydrocephalus. Rarely they may degenerate into squamous cell carcinoma.
Pathologically, dermoids are made up of ectodermal elements including squamous epithelium in combination with dermal appendage structures such as apocrine, sweat and sebaceous glands in addition to hair follicles. They are characterized by a thick lined unilocular cystic structure which may contain lipid or proteinaceous debris
Presenting symptoms includes headache and seizure. Suprasellar lesions may also result in visual disturbances.
On imaging, dermoids appear as unilocular cystic lesions. On CT the internal cyst contents may match fat attenuation on CT. The wall may be slightly thick, contain calcification and enhance. On MRI, the cyst contents may be hyperintense on T1 in regions due to high lipid content of the sebaceous material within the cyst. Fat-fluid levels may also be seen. Alternatively, some dermoids can look exactly like epidermoids.
Total surgical resection is the only effective treatment. Incomplete resection may result in recurrence.
Suprasellar Dermoid/Teratoma |
|
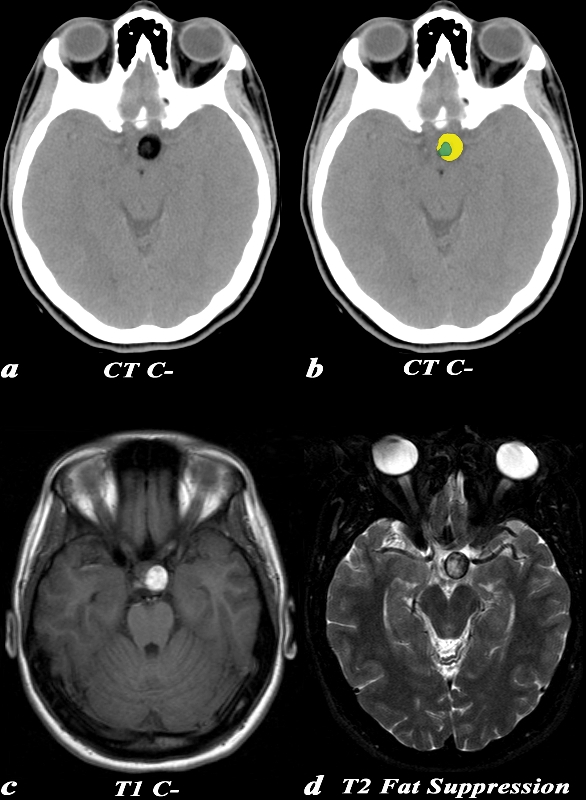
This 20 year old female presented with a headache. CT: (a,b) There is a well circumscribed low density lesion in the suprasellar region on this unenhanced
CT (a,b).
The density of this lesion for the most part matches that of fat (yellow d), which can also be seen on this image, for comparison, normally be seen in the subcutaneous tissues. There are also some internal subtle areas of higher density (green in d), consistent with the heterogeneous nature of this lesion.
MRI: (c,d) On a T1 weighted image (c), this suprasellar mass has predominantly high signal matching that of fat. T2 weighted image (d) which is acquired with a technique that suppresses signal from fat demonstrates mixed signal intensity. This shows areas of both fat (the hypointense areas) and soft tissue (the hyperintense areas).
These findings are consistent with a dermoid (teratoma)
Image Courtesy Elisa Flower MD and Asim Mian MD 97640c01.8
|
Archives of the AFIP — RadioGraphics 1995; 15: 1437-1455
References
J G Smirniotopoulos, E J Rushing, and H Mena. Pineal region masses: differential diagnosis. Radiographics May 1992 12:577-596
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Suprasellar Dermoid/Teratoma
This 20 year old female presented with a headache. CT: (a,b) There is a well circumscribed low density lesion in the suprasellar region on this unenhanced
CT (a,b).
The density of this lesion for the most part matches that of fat (yellow d), which can also be seen on this image, for comparison, normally be seen in the subcutaneous tissues. There are also some internal subtle areas of higher density (green in d), consistent with the heterogeneous nature of this lesion.
MRI: (c,d) On a T1 weighted image (c), this suprasellar mass has predominantly high signal matching that of fat. T2 weighted image (d) which is acquired with a technique that suppresses signal from fat demonstrates mixed signal intensity. This shows areas of both fat (the hypointense areas) and soft tissue (the hyperintense areas).
These findings are consistent with a dermoid (teratoma)
Image Courtesy Elisa Flower MD and Asim Mian MD 97640c01.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Suprasellar Dermoid/Teratoma
This 20 year old female presented with a headache. CT: (a,b) There is a well circumscribed low density lesion in the suprasellar region on this unenhanced
CT (a,b).
The density of this lesion for the most part matches that of fat (yellow d), which can also be seen on this image, for comparison, normally be seen in the subcutaneous tissues. There are also some internal subtle areas of higher density (green in d), consistent with the heterogeneous nature of this lesion.
MRI: (c,d) On a T1 weighted image (c), this suprasellar mass has predominantly high signal matching that of fat. T2 weighted image (d) which is acquired with a technique that suppresses signal from fat demonstrates mixed signal intensity. This shows areas of both fat (the hypointense areas) and soft tissue (the hyperintense areas).
These findings are consistent with a dermoid (teratoma)
Image Courtesy Elisa Flower MD and Asim Mian MD 97640c01.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 6
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 20 year old female presented with a headache. CT: (a,b) There is a well circumscribed low density lesion in the suprasellar region on this unenhanced
CT (a,b).
The density of this lesion for the most part matches that of fat (yellow d), which can also be seen on this image, for comparison, normally be seen in the subcutaneous tissues. There are also some internal subtle areas of higher density (green in d), consistent with the heterogeneous nature of this lesion.
MRI: (c,d) On a T1 weighted image (c), this suprasellar mass has predominantly high signal matching that of fat. T2 weighted image (d) which is acquired with a technique that suppresses signal from fat demonstrates mixed signal intensity. This shows areas of both fat (the hypointense areas) and soft tissue (the hyperintense areas).
These findings are consistent with a dermoid (teratoma)
Image Courtesy Elisa Flower MD and Asim Mian MD 97640c01.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 20 year old female presented with a headache. CT: (a,b) There is a well circumscribed low density lesion in the suprasellar region on this unenhanced
CT (a,b).
The density of this lesion for the most part matches that of fat (yellow d), which can also be seen on this image, for comparison, normally be seen in the subcutaneous tissues. There are also some internal subtle areas of higher density (green in d), consistent with the heterogeneous nature of this lesion.
MRI: (c,d) On a T1 weighted image (c), this suprasellar mass has predominantly high signal matching that of fat. T2 weighted image (d) which is acquired with a technique that suppresses signal from fat demonstrates mixed signal intensity. This shows areas of both fat (the hypointense areas) and soft tissue (the hyperintense areas).
These findings are consistent with a dermoid (teratoma)
Image Courtesy Elisa Flower MD and Asim Mian MD 97640c01.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Suprasellar Dermoid/Teratoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Suprasellar Dermoid/Teratoma
)
