Medulloblastoma
Sumit Karia MD
The Common Vein Copyright 2010
Definition
Medulloblastoma is a primary malignant tumor of the brain derived from cells of the primitive neuroectoderm. It originates in the cerebellum or posterior fossa, and is the most common malignant tumor of childhood, affecting males twice as much as females. It is also present in adulthood, mostly in adults in their 20?s.
Morphologically, the tumor is a granular mass with necrosis; desmoplastic variants are rich in protein ? reticullin and collagen.
Functionally, it produces intracranial hypertension symptoms – headaches, nausea & vomiting, ataxia, dizziness, focal and brainstem symptoms are all possible symptoms at presentation. Ataxia, diplopia and general cerebellar dysfunction, most often positional dizziness and nystagmus, are also frequent.
On imaging, with CT and MRI show an enhancing tumor, usually with calcification, and distorting the fourth ventricle. Since many times there is an obstruction to the normal flow of the CSF, hydrocephalic pattern is seen. The neuroaxis should be imaged as well, to rule out metastasis, given its propensity to produce secondary deposits.
Treatment is initiated with surgical resection, which also has great symptomatic relieve, by diminishing intracranial pressure and mass compression. It is followed by radiotherapy, and chemotherapy can be used as an adjuvant, specially in high-risk patients, because it improves survival in this group.
|
Midline Medulloblastoma |
|
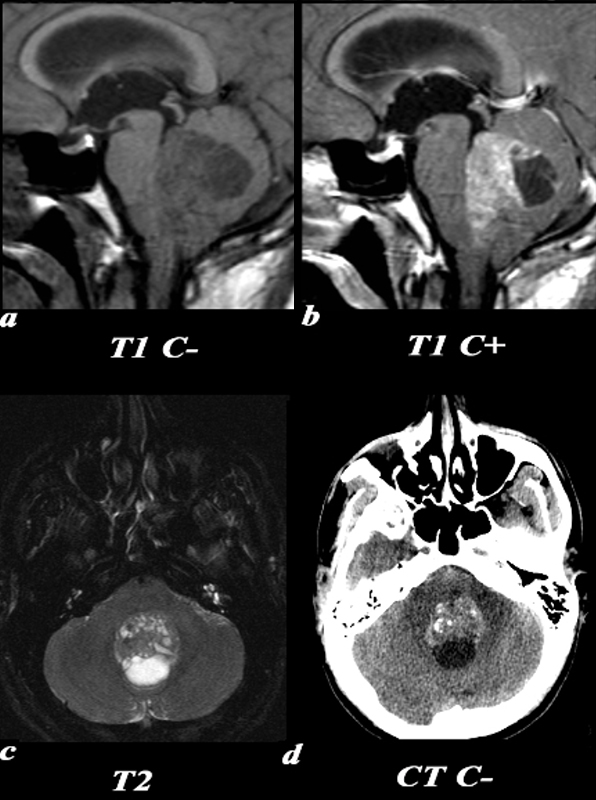
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting.
T1 pre (a,c) and post (b,d): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum.
T2 (e): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas.
CT(f): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced.
Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81
|
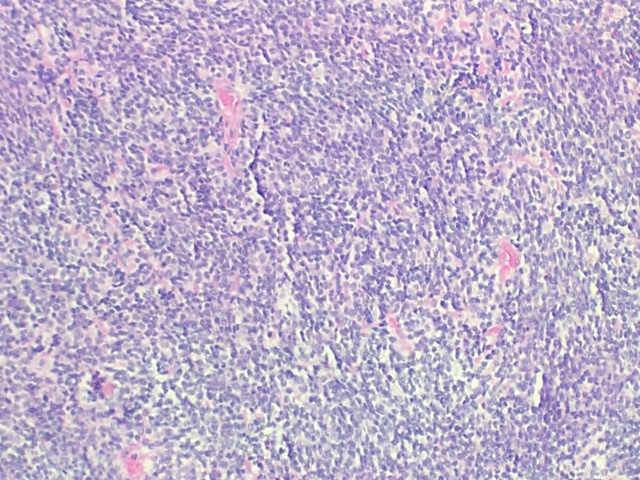
H&E Low Power
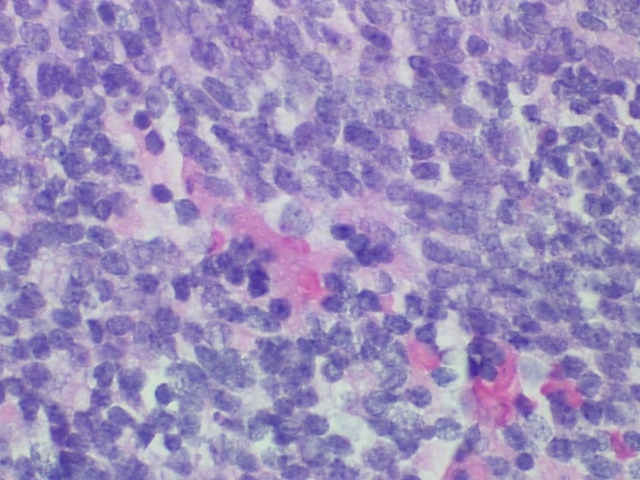
H&E High Power
Medulloblastoma |
| These low and high power polymicrographs demonstrate densely packed small blue cells. Better seen on high power is the large size of the nuclei relative to the small amount of surrounding cytoplasm within the cell. The nuclei have a ?salt and pepper? appearance of the chromatin which suggests neural differentiation. Notice that some of the nuclei are elongated, or carrot shaped as well.
Image Courtesy of Cheryl Spencer, M.A. and Ivana Delalle, MD, PhD Department of Pathology Boston University School of Medicine 98509/10 (S07-13587)
|
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => These low and high power polymicrographs demonstrate densely packed small blue cells. Better seen on high power is the large size of the nuclei relative to the small amount of surrounding cytoplasm within the cell. The nuclei have a ?salt and pepper? appearance of the chromatin which suggests neural differentiation. Notice that some of the nuclei are elongated, or carrot shaped as well.
Image Courtesy of Cheryl Spencer, M.A. and Ivana Delalle, MD, PhD Department of Pathology Boston University School of Medicine 98509/10 (S07-13587)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => These low and high power polymicrographs demonstrate densely packed small blue cells. Better seen on high power is the large size of the nuclei relative to the small amount of surrounding cytoplasm within the cell. The nuclei have a ?salt and pepper? appearance of the chromatin which suggests neural differentiation. Notice that some of the nuclei are elongated, or carrot shaped as well.
Image Courtesy of Cheryl Spencer, M.A. and Ivana Delalle, MD, PhD Department of Pathology Boston University School of Medicine 98509/10 (S07-13587)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Midline Medulloblastoma
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting.
T1 pre (a,c) and post (b,d): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum.
T2 (e): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas.
CT(f): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced.
Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Midline Medulloblastoma
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting.
T1 pre (a,c) and post (b,d): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum.
T2 (e): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas.
CT(f): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced.
Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 5
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting.
T1 pre (a,c) and post (b,d): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum.
T2 (e): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas.
CT(f): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced.
Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 26 year old male presented with a three week history of progressive headache, nausea and vomiting.
T1 pre (a,c) and post (b,d): The exact origin of this mass can be difficult to ascertain given its large size. It clearly grows into the fourth ventricle, widening the lower portion of the Sylvian aqueduct. Note the smooth interface with the posterior aspect of the pons with associated mass effect verses the more irregular margin posteriorly where it arises from the cerebellum.
T2 (e): The solid component of the medulloblastoma matches gray matter signal. Cystic or necrotic areas are demonstrated by higher T2 signal areas.
CT(f): The unenhanced CT scan demonstrates a predominately hyperdense mass with punctuate calcifications in the region of the fourth ventricle . The low density area posteriorly is a cystic or necrotic component of the mass while the fourth ventricle is completely effaced.
Image Courtesy Elisa Flower MD and Asim Mian MD 97668c01.81
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Midline Medulloblastoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Midline Medulloblastoma
)
