When viewed from the front, it assumes the form of a gentle reversed ?S?. The upper of the two lateral curvatures is convex toward the left. The lower curvature, in the lower thorax and abdomen, is convex toward the right. From its commencement at the lower margin of the cricoid cartilage, the esophagus inclines slightly to the left until its left border projects approximately ¼? to the left of the tracheal margin. It then swings somewhat to the right, reaching the midline at about the level of the fourth thoracic vertebra behind the aortic arch. It continues its inclination to the right until about the level of the seventh thoracic vertebra, where it again turns left somewhat more sharply than in its precious curves, and in this direction it passes through the esophageal hiatus.
The course of the esophagus is marked by several indentations and constrictions:
1.) The first narrowing of the esophagus is found at its commencement, caused by the cricopharyngeus muscle and the cricoid cartilage. This narrowing is in fact the upper esophageal sphincter.
2.) The esophagus is indented on its left side by the arch of the aorta.
3.) The left main bronchus causes, generally, an impression on the left anterior aspect of the esophagus.
4.) At its lower end the esophagus is narrowed by the inferior esophageal sphincter and the esophagogastric vestibule.
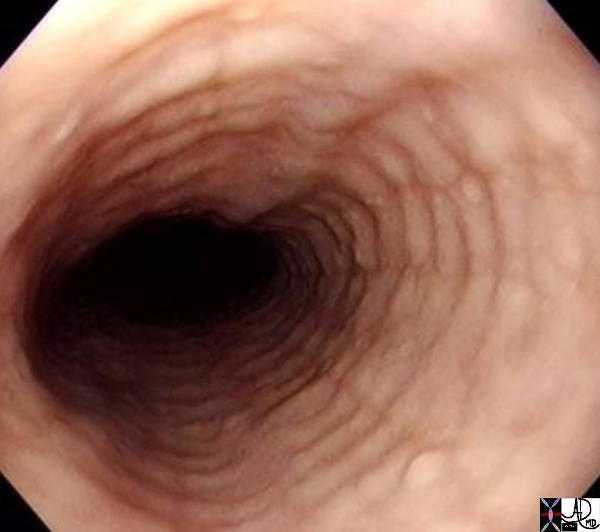
Although the esophagus is usually described as tubelike, in the resting state it is flattened anteroposteriorly so that the transverse axis is larger than its anteroposterior axis. In the resting state the esophageal walls approximate each other.
Given this property, air insufflation is a key component of endoscopic evaluation so that proper distension and visualization can be obtained. Below is a video capsule image of a normal esophagus which shows the narrow and non-distended lumen.
Image needed in JPEG
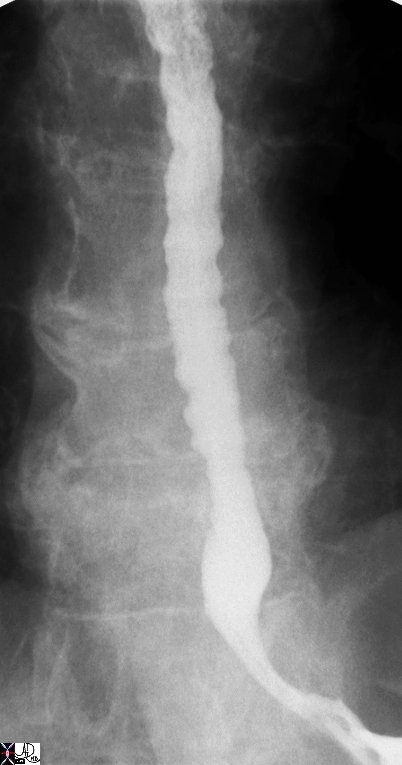
Shape of Esophagus – normal anatomy |
| 49742 esophagus GE junction gastroesophageal junction normal anatomy double contrast barium swallow upper GI Courtesy Ashley DAvidoff MD |

Circular Folds – Feline Esophagus
|
| 00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD |
Feline Esophagus by Endoscopy
|
| 73476 esophagus feline esophagus circumferential muscle contractions normal variant anatomy endoscopy endoscope Courtesy Joshua NAmias MD |
Tertiary Contraction Waves
|
| 76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD |
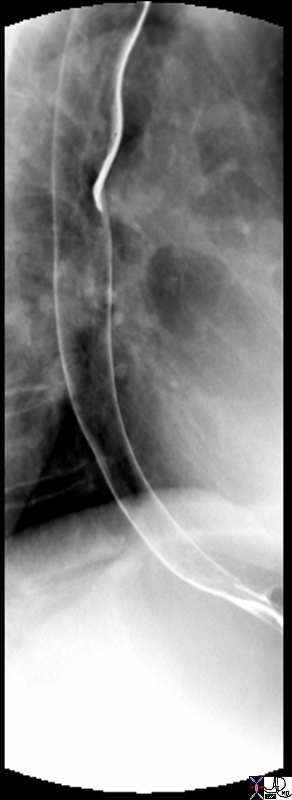
Alterations in this normal anatomic shape can be quite varied and cause significant symptoms to the patient. An example is seen below in a patient with a ?cork-screw? esophagus which in the adult population would be characteristic of diffuse esophageal spasm and in the elderly a manifestation of ?presbyesophagus? ? uncoordinated contraction due to the aging process. One can imagine that the passage of a food bolus could be quite difficult given the many, and often sharp, twists and turns. The patient whose barium study is shown below, would most certainly have a complaint of dysphagia.
01232.jpg
Shape of Esophagus – Corkscrew |
| Courtesy Ashley Davidoff MD 01232 code esophagus + fx corkscrew shape + dx diffuse esophageal spasm + barium swallow upper GI UGI imaging radiology contrast X-Ray |

Shape of Esophagus – Corkscrew |
| Courtesy Ashley Davidoff MD 01238 sophagus + fx corkscrew shape + fx irregular + dx presbyesophagus + barium swallow upper GI UGI imaging radiology contrast X-Ray |

Size and Shape Abnormality
|
| 76166c esophagus dysphagia retained food bezoar stricture pulsion diverticuli barium pill did not pass peptic stricture obstruction mechanical shape single contrast barium swallow Courtesy Ashley Davidoff MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Size and Shape Abnormality
76166c esophagus dysphagia retained food bezoar stricture pulsion diverticuli barium pill did not pass peptic stricture obstruction mechanical shape single contrast barium swallow Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Size and Shape Abnormality
76166c esophagus dysphagia retained food bezoar stricture pulsion diverticuli barium pill did not pass peptic stricture obstruction mechanical shape single contrast barium swallow Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 76166c esophagus dysphagia retained food bezoar stricture pulsion diverticuli barium pill did not pass peptic stricture obstruction mechanical shape single contrast barium swallow Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 76166c esophagus dysphagia retained food bezoar stricture pulsion diverticuli barium pill did not pass peptic stricture obstruction mechanical shape single contrast barium swallow Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Size and Shape Abnormality
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Size and Shape Abnormality
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Shape of Esophagus – Corkscrew
Courtesy Ashley Davidoff MD 01238 sophagus + fx corkscrew shape + fx irregular + dx presbyesophagus + barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Shape of Esophagus – Corkscrew
Courtesy Ashley Davidoff MD 01238 sophagus + fx corkscrew shape + fx irregular + dx presbyesophagus + barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Courtesy Ashley Davidoff MD 01238 sophagus + fx corkscrew shape + fx irregular + dx presbyesophagus + barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Courtesy Ashley Davidoff MD 01238 sophagus + fx corkscrew shape + fx irregular + dx presbyesophagus + barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Shape of Esophagus – Corkscrew
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Shape of Esophagus – Corkscrew
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Shape of Esophagus – Corkscrew
Courtesy Ashley Davidoff MD 01232 code esophagus + fx corkscrew shape + dx diffuse esophageal spasm + barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Shape of Esophagus – Corkscrew
Courtesy Ashley Davidoff MD 01232 code esophagus + fx corkscrew shape + dx diffuse esophageal spasm + barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Courtesy Ashley Davidoff MD 01232 code esophagus + fx corkscrew shape + dx diffuse esophageal spasm + barium swallow upper GI UGI imaging radiology contrast X-Ray
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Courtesy Ashley Davidoff MD 01232 code esophagus + fx corkscrew shape + dx diffuse esophageal spasm + barium swallow upper GI UGI imaging radiology contrast X-Ray
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Shape of Esophagus – Corkscrew
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Shape of Esophagus – Corkscrew
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Tertiary Contraction Waves
76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Tertiary Contraction Waves
76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 76208 esophagus tertiary contraction waves normal function single contrast barium swallow Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Tertiary Contraction Waves
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Tertiary Contraction Waves
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Feline Esophagus by Endoscopy
73476 esophagus feline esophagus circumferential muscle contractions normal variant anatomy endoscopy endoscope Courtesy Joshua NAmias MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Feline Esophagus by Endoscopy
73476 esophagus feline esophagus circumferential muscle contractions normal variant anatomy endoscopy endoscope Courtesy Joshua NAmias MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 73476 esophagus feline esophagus circumferential muscle contractions normal variant anatomy endoscopy endoscope Courtesy Joshua NAmias MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 73476 esophagus feline esophagus circumferential muscle contractions normal variant anatomy endoscopy endoscope Courtesy Joshua NAmias MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Feline Esophagus by Endoscopy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Feline Esophagus by Endoscopy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Circular Folds – Feline Esophagus
00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Circular Folds – Feline Esophagus
00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 00567b01 esophagus circular folds feline esophagus anatomy normal Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Circular Folds – Feline Esophagus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Circular Folds – Feline Esophagus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Shape of Esophagus – normal anatomy
49742 esophagus GE junction gastroesophageal junction normal anatomy double contrast barium swallow upper GI Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Shape of Esophagus – normal anatomy
49742 esophagus GE junction gastroesophageal junction normal anatomy double contrast barium swallow upper GI Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49742 esophagus GE junction gastroesophageal junction normal anatomy double contrast barium swallow upper GI Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49742 esophagus GE junction gastroesophageal junction normal anatomy double contrast barium swallow upper GI Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Shape of Esophagus – normal anatomy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Shape of Esophagus – normal anatomy
)
