
The liver resides in the upper and right quadrants of the abdominal cavity, nearly occupying the entire right hypochondrium, the greater part of the epigastrium, and not uncommonly extending into the left hypochondrium as far as the mammillary line. Position of the liver
This plain film of the abdomen shows the position of the liver in the abdominal cavity. Note it lies just below the right hemidiaphragm and it occupies almost the entire right upper quadrant. The metallic object in the center of the abdomen is an umbilical ring. (Image courtesy of Ashley Davidoff M.D.)
Position of the liver
The thick blue line that traverses the green gallbladder represents the position of the middle hepatic vein that divides the liver into right and left lobes. The thinner line represents the position of the falciform ligament which divides the left lobe into a medial rightward segment (IV)and a lateral leftward segment. (II and III) Part of the left lobe usually lies toward the right side. (Image courtesy of Ashley Davidoff M.D.)The left lobe is usually mostly on the right side of the body. Sometimes the lateral segments of the left lobe will cross the midline to lie leftward of the midline. The medial segment, segment IV, usually remains on the right side.Position of the liverIn this cross sectional image the liver is seen in relation to the J shaped stomach just medial the spleen posteriorly and the colon laterally. It occupies almost the entire right upper quadrant. (Image courtesy of Ashley Davidoff M.D.)Although unusual, some day you may come across a patient with situs inversus, which can make you look twice. In these patients, the position of the organs are reversed, with the liver on the left! Position of the liverThis image shows a contrast enhanced CT of a patient with situs inversus where the position of the internal organs are reversed from right to left and left to right. Notice the liver on the right side of the image and the left side of the body. (Image courtesy of Ashley Davidoff M.D.)Question free air?This image shows a curvilinear air shadow that suggests free ar under the diaphragm. The patient was asymptomatic and so a subsequent upright KUB was performed. See next image (Image courtesy of Ashley Davidoff M.D.) 45758 45759Question free air?This upright iamge of the abdomen clearly shows that the air under the diapragm is part of air within the lumen of a loop of bowel in the right upper quadrant. (Image courtesy of Ashley Davidoff M.D.) 45761Chilaiditi syndrome – interposition the colonThis coronal image of the abdomen shows the colon and specifically the hepatic flexure malpositioned under the diaphragm and mimics the presence of free air under the diaphragm as noted in the above images. The liver is displaced from its usual position by the colon which makes its way anteriorly (in front of the liver), and superiorly (below the diaphragm), so that if there is air within this loop it will masquerades as “free air” (Image courtesy of Ashley Davidoff M.D.) 45765Chilaiditi syndrome – interposition the colonThis axial image of the abdomen shows the colon and specifically the hepatic flexure malpositioned anterior to the liver. The liver is displaced from its usual position by the colon which makes its way anteriorly (in front of the liver), and superiorly (below the diaphragm), so that if there is air within this loop it will masquearades as “free air” (Image courtesy of Ashley Davidoff M.D.) 45768
Abnormal l liver position left sided liver caused in the congenital conditions situs inversus seen in situs inversus (partial or total) Kartageners syndrome asplenia syndrome polysplenia syndrome herniations of the liver can occur into chest lateral abdominal wall anterior abdominal wall left lobe sometimes curls around spleen females particularly Riedel’s lobe is a normal variant where the right lobe extends to the right lower quadrant
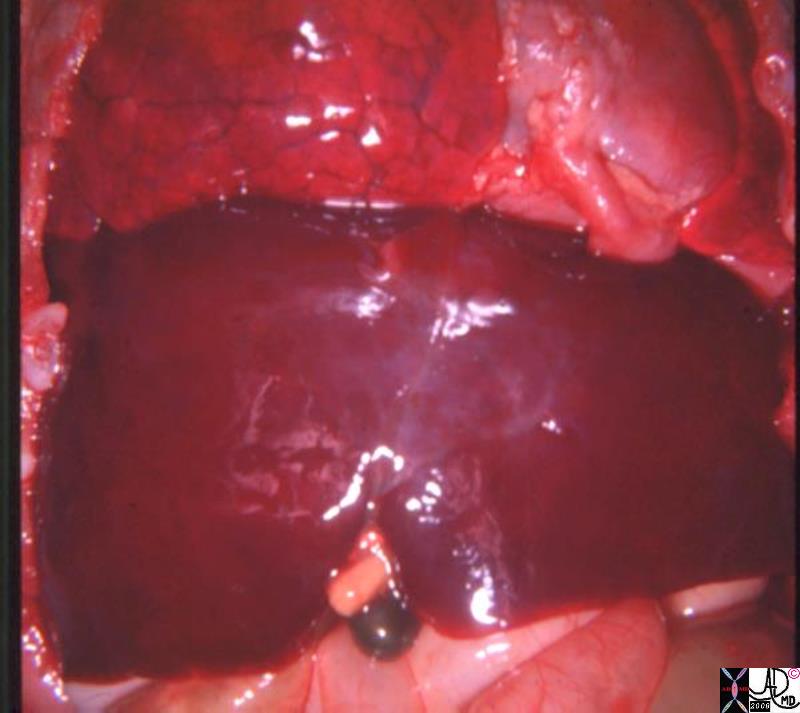
Central Gallbladder Situs Ambiguus |
| 82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008 |