
“Do not despise your own place and hour. Every place is under the stars, every place is the center of the world.”
John Burroughs, Studies in Nature and Literature
PositionThe Common Vein copyright 2009
“Not invisible but unnoticed Watson.You did not know where to look so you missed all that was important.” said Sherlock Holmes in “A Case of Identity”.
A sign with this quote remained on my reading board for 16 years and its message is embedded in my psyche.
The position of the parts of the body and particularly positioning of parts in relation to each other is another critical aspect of structure. In the clinical realm, the position of the internal organs is determined by external landmarks; this is called surface anatomy.
The heart has a very characteristic position in the chest. It is a little off midline toward the left, with the left ventricular apex pointing down and slightly out and leftward. It can be palpated in the left midclavicular line in the fifth rib interspace. When the left ventricle is enlarged, the position of the apex shifts down and more leftward. The right ventricle is anterior to the left ventricle and lies just leftward of the sternum. Since it is a low pressure structure, it cannot be palpated under normal circumstances. When it enlarges a left parasternal heave is palpated.
The aortic valve lies on the right sternal border in the second rib interspace. One would have thought that as a left sided structure it would be on the left, but in fact it sits to the right of the pulmonary valve and to the right of the sternum. Thus the aortic valve it is best heard auscultated in the second interspace on the right side of the sternum. The pulmonary valve, on the other hand, is best evaluated in the second interspace on the left side. Odd, but true and important.
The reason for describing the surface anatomy of the heart is not to expect rote memorization, but rather to reiterate the principle of understanding the position of structure. This information carries important clinical relevance.
A few other examples demonstrating the relevance of position of structure at the bedside and even in life saving maneuvers follow.
There is no more critical time to know the position of structures than when performing resuscitative measures. Knowing the position of key structures and their neighbors is essential in a host of critical circumstances: when placing a femoral venous line or internal jugular line for rapid infusion of fluids during uncontrolled hemorrhage when blood pressure is falling; when positioning an endotracheal tube in the airway and avoiding the esophagus during airway maintenance in acute respiratory failure; when catheterizing the left coronary ostium during thrombolytic administration for acute coronary thrombosis; and when performing an emergency cricothyrotomy through the cricothyroid membrane for acute airway obstruction. These procedures all require knowledge of position of the structure and or knowledge of easily identified surface structures that are used as reference landmarks.
Situs inversus is a condition where all or some of the bodily organs are inverted in location across the midline. For some patients this condition represents a mere incidental anomaly which they may not be aware of, nor affected by. When associated anomalies are present in some patients, particularly when cardiac anomalies are present, death can ensue. Kartagener’s syndrome (immotile cilia syndrome) is characterized by situs inversus, bronchiectasis, chronic sinusitis and infertility. The most severe form of situs inversus is seen in the asplenia syndrome which is usually a fatal condition in infancy because of associated severe forms of congenital heart disease.
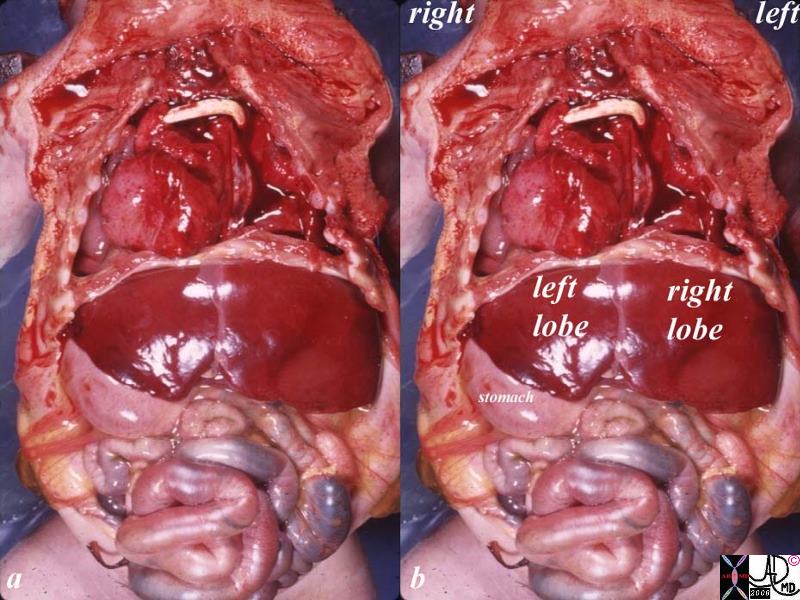
The image is from the post mortem of an unfortunate baby with severe congenital disorder that included situs inversus and and a cardiac anomaly that proved to be fatal following attempts at surgical correction. The heart is dominantly in the right chest and this is called dextrocardia. The yellow tube in the chest is a shunt suggesting a severe obstruction in the proximal circulation and that a bypass was needed to circumvent the obstruction. The detail of the disorder or the shunt is not known. The triangular shaped left lobe of the liver is on the right, the right lobe is on the left, and the stomach is on the right, all suggesting a diagnosis of situs inversus totalis.Courtesy Ashley Davidoff MD. 10850c01.8s code cardiac heart situs inversus liver stomach heart bypass congenital grosspathology
Central Gallbladder in Situs Ambiguus
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008
More scientifically challenging and deeply perplexing than malpositioned organs are the diseases associated with a single misplaced, displaced, or replaced amino acid in the DNA strand. These positional defects can result in devastating disease including thallasemia, sickle cell anemia, cystic fibrosis, or Huntington’s chorea. In these congenital disorders the most seemingly minor malposition of a single amino acid has far reaching clinical implications. The challenge of treating such disorders is on the horizon for the coming generations of scientists and doctors.
Position also infers and implicates the concept of space. Cells organs, people, families and nations need their own space in order to function and contribute to the society at large. One of the most significant consequences of malignant disease is that cancer occupies space but does not contribute to the well being of the “society” in which it resides. Malignant disease can be viewed as an aggressive and foreign group of cells (“squatters”) that embed in a mother organ, grow off the fat of the land, contribute nothing to the function of the society at large, and by multiplication take over space and displace normal and well functioning tissue. This is the nature of malignancy. Eventually it either impedes the function of the mother organ, or it sends seedlings directly into the surrounding tissues, into the lymph nodes, and or via the circulation to distant organs where it takes up more space and impedes the function of other organs. Eventually orderly society succumbs, together with the parasite, and all is lost.
The difficulty again relates to how a medical student can know which of the detail provided in the structural courses in medical school have clinical relevance. Is it important to know a seemingly minor anatomical point like “the intercostal arteries, veins and nerves run inferior to the ribs”? How can the medical student know or understand the relevance of this dry fact? How does one continually integrate the vast array of information with its practical relevance and make the dry knowledge come alive? An arborized integration with a computer program written by the basic scientists and subsequently integrated with clinical science and medicine written by practicing physicians is the solution to this problem. With current systems in place the best advice is for educators to point out as much as possible. It is important to know how the information can be applied. Failing this difficult task of continued integration of basic and clinical faculty, the student has to be aware that the principles being outlined here (parts, size, shape, and position so far), do have clinical relevance and will at some time be revisited in a clinical career.
Principles

13275b01i01e12u08 sperm egg ovum conception time Davidoff Art
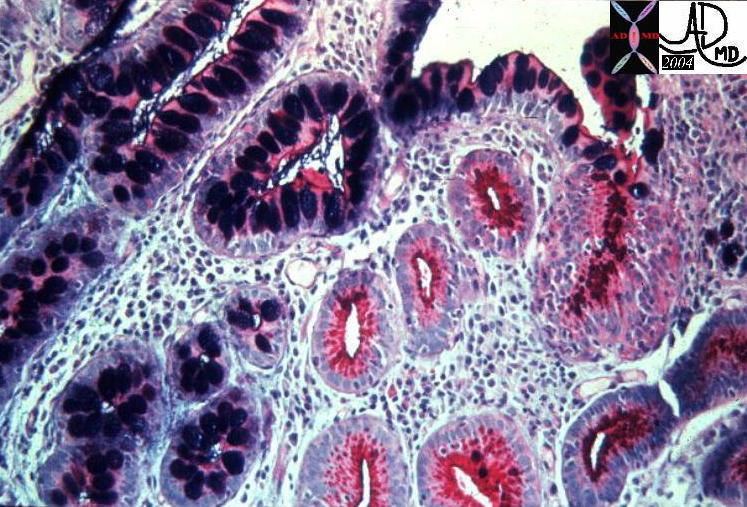
This is a classic example of a simple, single layered epithelium surrounding a central ductule. This histology is taken from the stomach but the structure is common to many other glands in the body 12269 Courtesy Barbara Banner MD
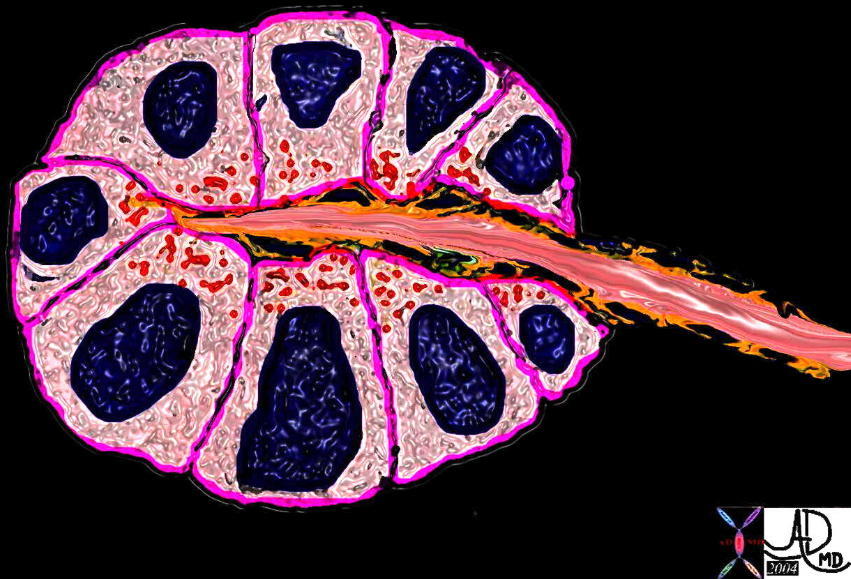
A classical acinus, with a simple single layered epithelium surrounding a central lumen and subtended by a ductule 39939b04 Courtesy Ashley Davidoff MD
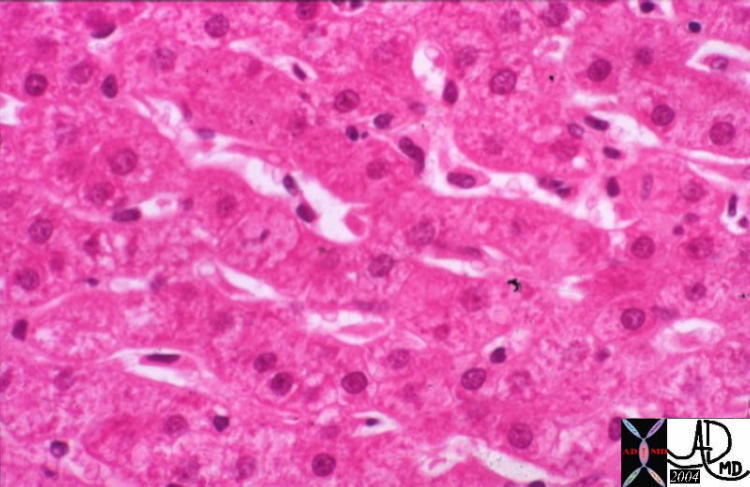
The cells of the liver are organized in cords and plates and are organized like spokes of a wheel around the central vein. The plates and cords are lined by the sinusoids which are the channels which carry blood to the liver. Just below the sinusoids, between the wall of the sinusoid and the capsule of the liver there is a space called the space of Disse which carries the lymphatic fluid of the liver. (Image courtesy of Barbara Banner M.D.) 13445
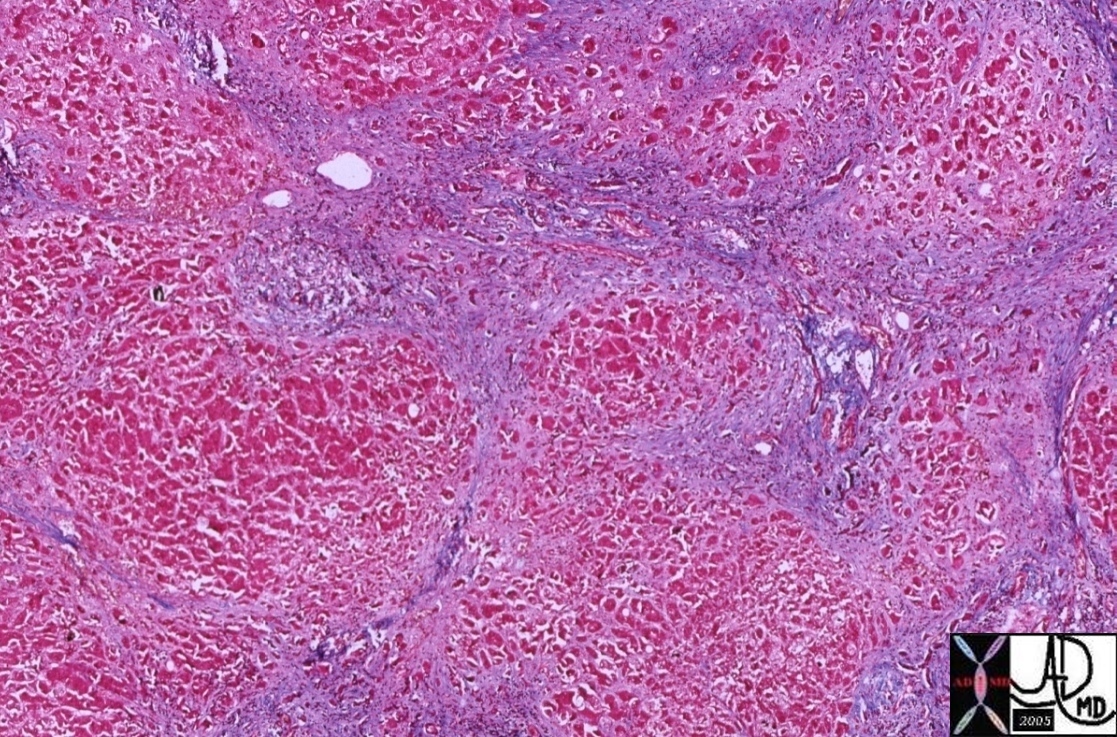
In cirrhosis the fibrotic tissue (blue) distorts the architecture so that the alignment of the cells in cords is distorted and hence the sinusoids are distorted. The “rivers” of portal flow thus meet resistance rather than flowing freely, and so portal hypertension results. 00375 liver hepatic cirrhosis fx fibrosis fx nodules fx bridging between the triads histopathology Courtesy Barbara Banner
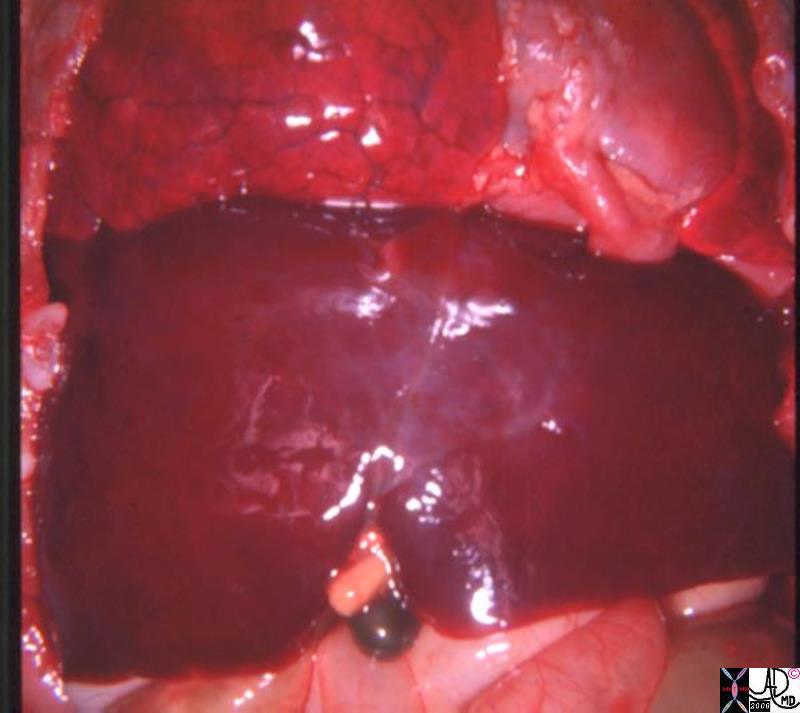
The liver in this patient is normal. Each cell has its space and position and can therefore function effectively and the macroscopic result is a normal appearing liver.13456 liver normal anatomy gallbladder stones cholelithiasis gross pathology

#brain cerebral cerebrum lateral ventricle anterior horn fx subependymal calcification ddx CMV cytomegalovirus toxoplasmosis, rubella and tuberous sclerosis. toxoplasmosis basal ganglia and the cortex are the commonly involved – diffusely scattered. rubella are evenly distributed. Tuberous sclerosis can be similar to CMV infection but in TS hypodense cortical tubers and subependymal enhancing nodules near foramen of Monro CTscan Davidoff MD 49498
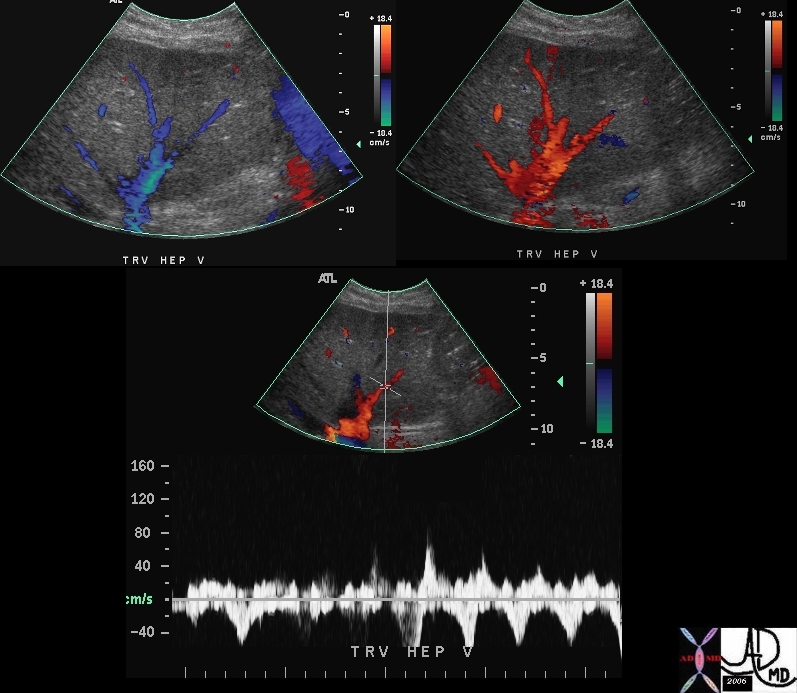
# liver hepatic veins acv waves normal anatomy physiology venous drainage Doppler flow color flow direction USscan Davidoff MD
46538c01

70294 acv waves hepatic veins doppler tricuspid valve regurgitation TR velocity Ultrasound Echocardiogram Davidoff MD
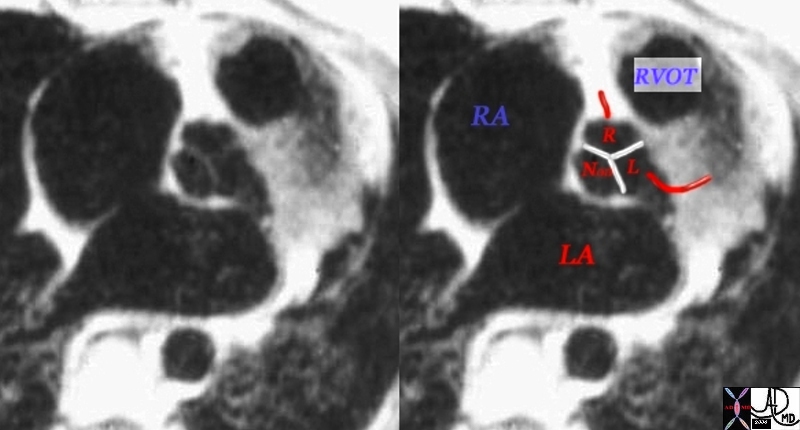
# heart cardiac aorta aortic valve infundibulum RVOT right ventricular outflow tract position relation MRI scan Davidoff MD
07954bWduo

# bone hand metacarpal fx fracture dx boxer’s fracture position alignment post pinning X-ray plain film Davidoff MD Davidoff MD
46806

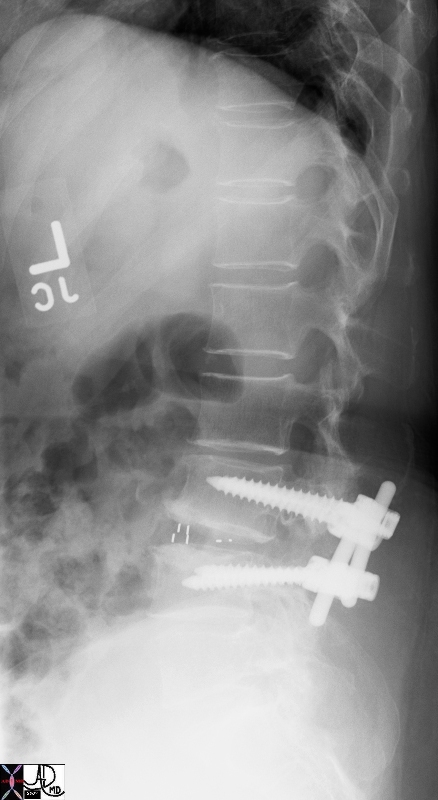
# bone spine lumbar spine L-S spine post op treatment retrolisthesis L3 onL 4 positional change degenerative disc disease osteoarthritis rod screws fixation sclerosis X-ray plain film of lumbar spine Courtesy Ashley Davidoff MD 72733 72734.800
Kartagener’s syndrome TCV page in the Heart module

49456 bone hand finger phalanx distal interphalangeal joint DIP 4th finger ring finger fracture through joint space probable avulsion fracture plain X-ray Davidoff MD 49456b01

46704 abdomen pregnancy fetus baby head brain lungs amniotic cavity amniotic fluid normal anatomy physiology MRI T2 weighted Davidoff MD
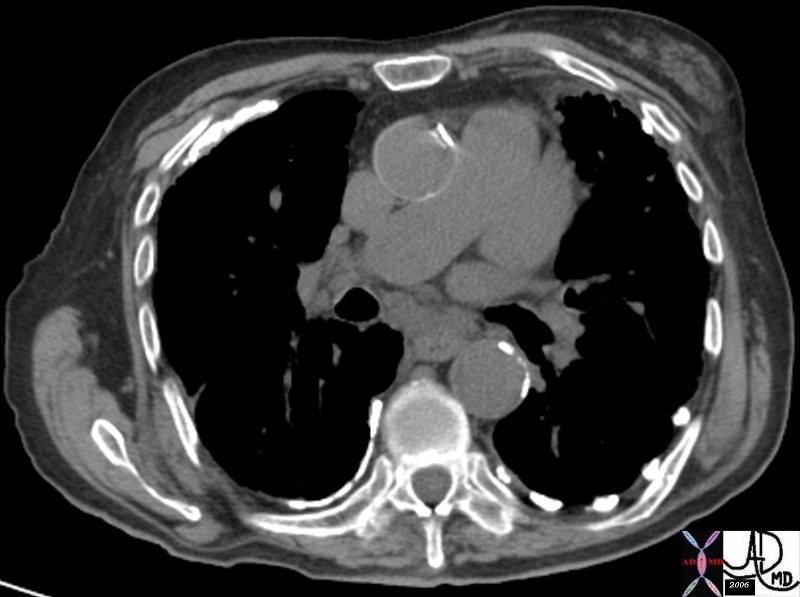
46624 hx 77 year old male with SOB breast pleura fx gynecomastia pleural calcification dx asbestos related disease dx asbestosis CTscan Davidoff MD 46621 46623 46624 46622

The buildings in this town in Muizenberg South Africa, like all towns are positioned around the streets, optimally in rectangular format, to allow for eficient access through the town.57927.800 Davidoff photography

The CT reveals an obviously aggressive lesion in the left breast of a 66year old female. It is extending as an irregular mass invading the chest wall posteriorly and projecting through the skin anteriorly. Courtesy Ashley Davidoff MD 43615
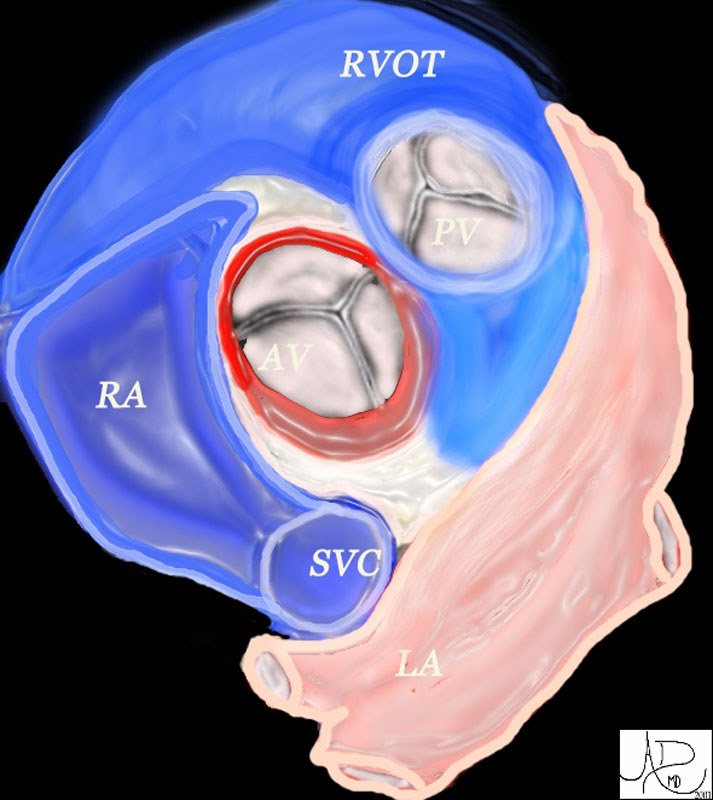
The aortic valve (AV) lies central to many structures including the right ventricular outflow tract (RVOT), pulmonary valve(PV), left atrium (LA), right atrium (RA), and superior vena cava (SVC). aorta from above47681 heart cardiac aortic valve aorta right atrium right atrial appendage left atrial appendage LAA RAA pulmonary valve right ventricular outflow tract left atrium LA RA RVOT anatomy normal position relations Davidoff art Davidoff MD
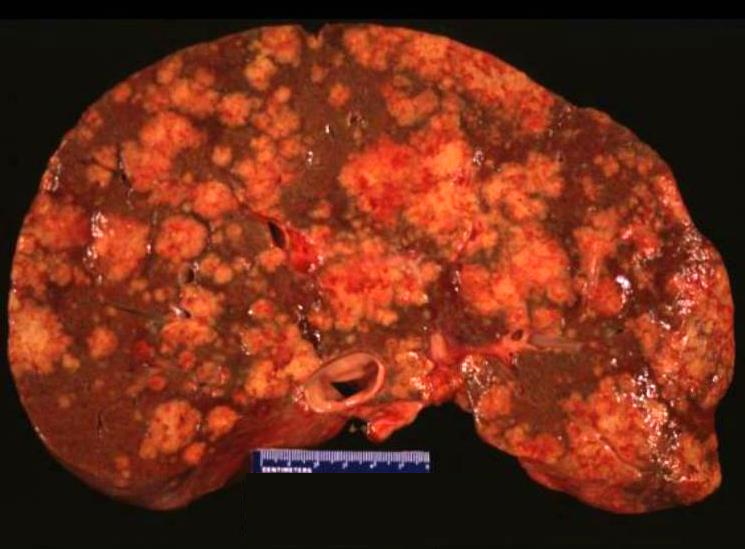
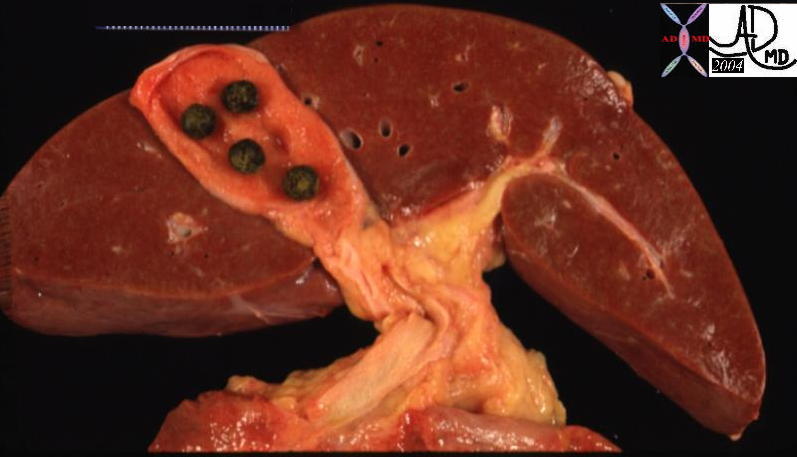
The normal liver cells have been displaced from their normal position in the liver and have been overridden by squatters who cannot function like normal liver cells. In fact in this instance the squatters are malignant cells and they cause the demise of the organ and eventually the organism, by their relentless displacement of the normal tissue.02639
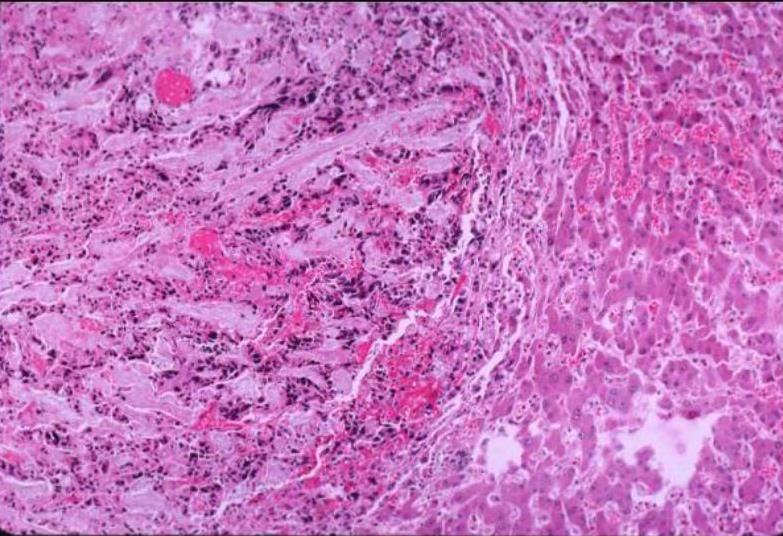
The malignant tissue is to your left and the normal liver tissue is on the right. The malignant tissue is pushing the normal liver out of its way. In the top right hand part of the image the tumor is displacing, compressing the normal liver and causing congestion.02638
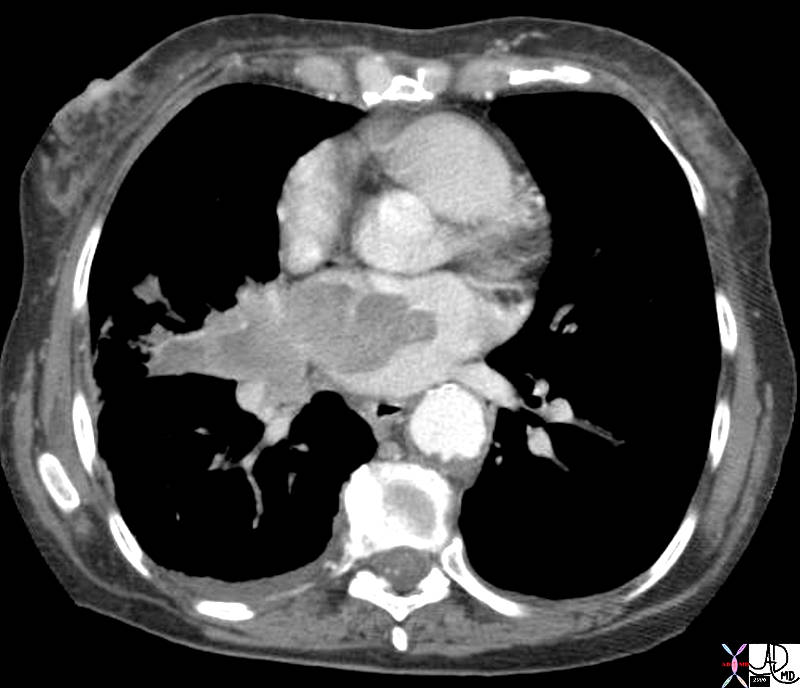
42379.800 heart cardiac pulmonary veins LA left atrium fx mass dx lung carcinoma invading the left atrium CTscan Davidoff MD space tumor aggressive space


19701 gallbladder + wall + fx calcification + cholecystoses + hyperplastic cholecystoses cholesterolosis imaging radiology CTscan Aschoff -Rokitansky sinuses

28007b02 Courtesy Ashley Davidoff MD abdomen liver pancreas IVC gallbladder fx situs inversus normal anatomy anatomic variant position congenital growth
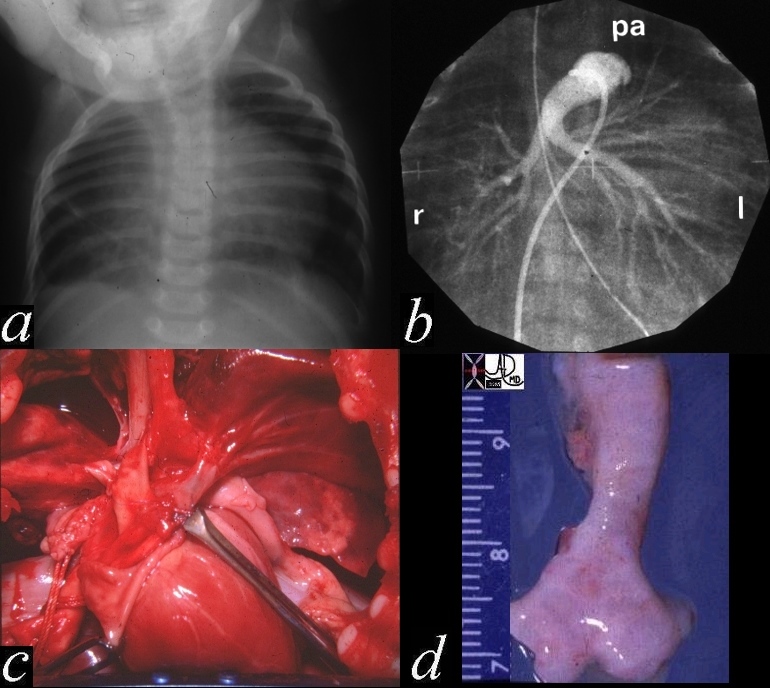
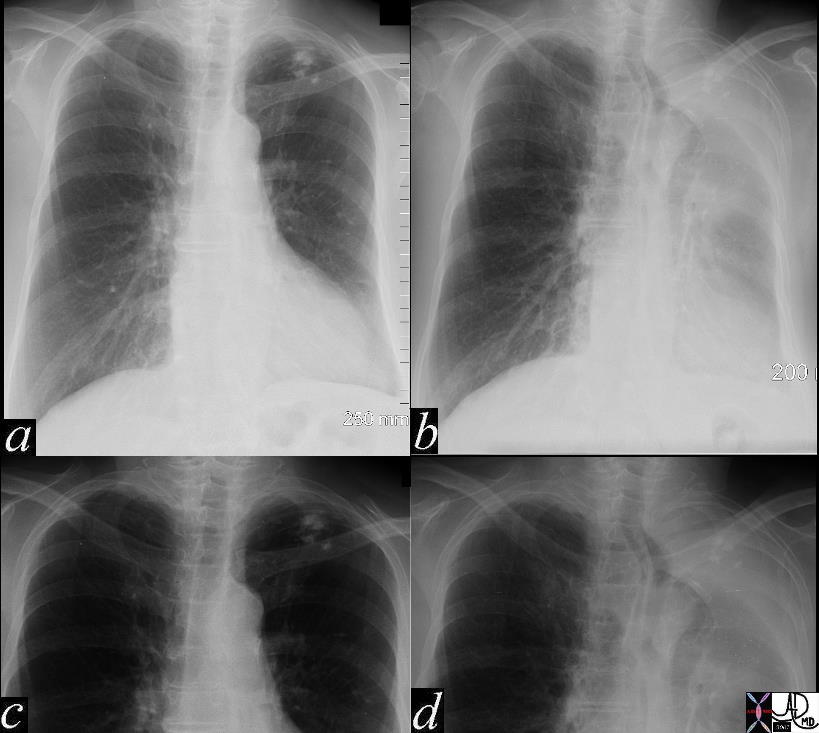
This autopsy is from a neonate who had respiratory difficulty at birth and showed a hyperinflated right lung with secondary leftward mediastinal shift. (a) A pulmonary angiogram showed the ight pulmonary artery arisingfrom th left PA rather than from the MPA (b) The gross in situ pathology shows the RPA coursing behind the trachea (c), while the last image (d) shows the narrowing of the left distal trachea. Histologically there was tracheomalacia secondary to the pressure effects of the LPA n the right side of the trachea causing right died bronchial obstruction with air trapping in the right lung.01533c02 Davidoff MD
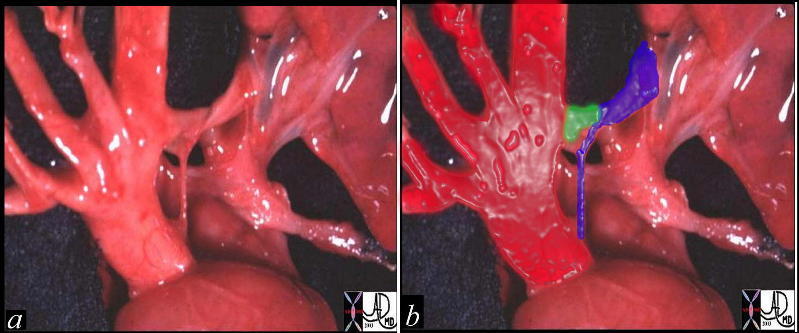
This pathological specimen shows an anteriorly positioned larger aorta (bright red in b)in front and to the right of the the string like atretic , posteriorly placed main pulmonary artery (royal blue in b). The ductus arteriosus (green overlay in b) is one of the mechanism via which the pulmonary circulation is able to maintain flow. Courtesy Ashley Davidoff MD 01473c02

This angiogram in RAO projection shows prolapse of both the anterior and posterior leaflets of the mitral valve with mitral regurgitation. Note also the bulbous appearance of the aortic sinuses. The back wall of the left atrium is flattened against the spine suggesting a narrow A-P diameter or pectus excavatum. These findings are characteristic of Maran’s syndrome Courtesy Ashley Davidoff MD. 34810c

Beaver tail shape of the left lobe of the liver wrapping around the spleen. It is a normal variant
22383
spleen + liver double moon (dupla lua ) + fx large left lobe of liver + imaging radiology USscan

39177.800 bone shoulder joint clavicle fx healed fracture trauma normal humerus normal scapula plain X-ray Davidoff MD

This is a T1 weighted coronal MRI through the chest in this young patient showing dextrocardia and a malpositioned ascending aorta. The patient has a diagnosis of single ventricle with situs inversus, L-loop, an aortic valve which is right sided base with respect to the expected position of the pulmonary valve which in this case is atretic. Davidoff MD. 16947b
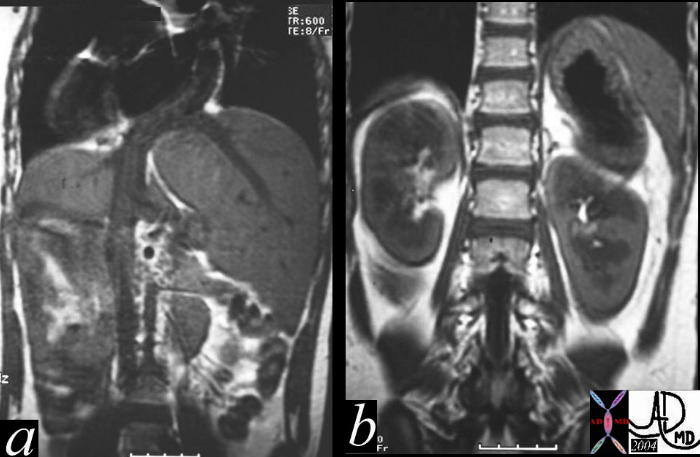
Courtesy Ashley Davidoff MD 26650c code stomach + fx normal + liver inversus heart cardiac fx situs inversus dx situs ambiguus + dx dextrocardia + dx asplenia syndrome + MRI T1 position

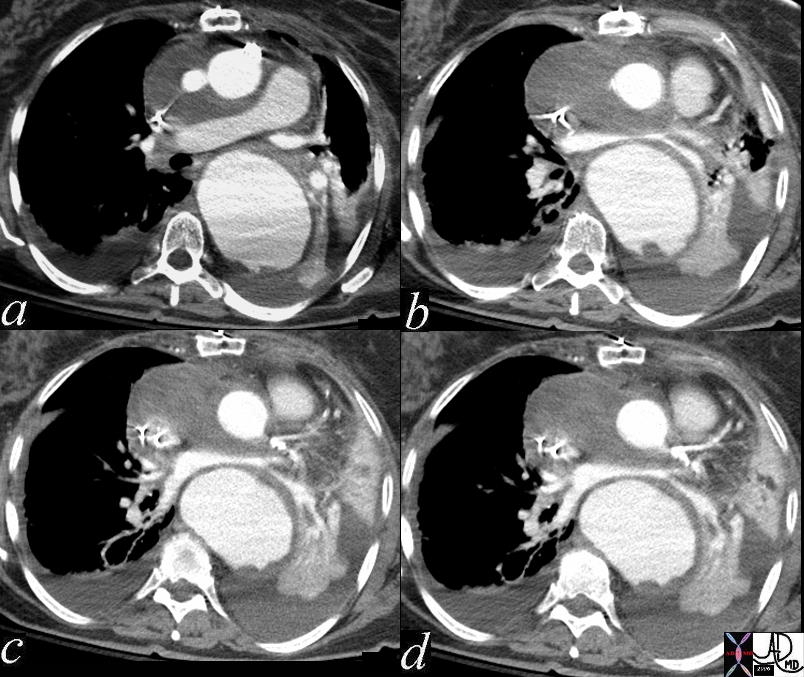
The left retrocardiac mass of fat density seen in the axial CTscans a, and b and the coronal scans in c and d, is reminiscent of fat herniating through a diaphragmatic defect. The finding is characteristic of a Bochdalek hernia Davidoff MD 39235c01
The image is from the post mortem of an unfortunate baby with severe congenital disorder that included situs inversus and and a cardiac anomaly that proved to be fatal following attempts at surgical correction. The heart is dominantly in the right chest and this is called dextrocardia. The yellow tube in the chest is a shunt suggesting a severe obstruction in the proximal circulation and that a bypass was needed to circumvent the obstruction. The detail of the disorder or the shunt is not known. The triangular shaped left lobe of the liver is on the right, the right lobe is on the left, and the stomach is on the right, all suggesting a diagnosis of situs inversus totalis.Courtesy Ashley Davidoff MD. 10850c01.8s code cardiac heart situs inversus liver stomach heart bypass congenital grosspathology

15018b cardiac heart coronary artery coronary ostium malposition bicuspid aortic valve aorta hypoplastic grosspathology Courtesy Ashley Davidoff MD
49460c03 respiratory system lung left upper lobe fx atelecatsis compensation mediastinal shift lung shift volume loss plain CXR chest X-ray popcorn calcification Davidoff MD 49460c02.800

49675c01 brain cerebrum cerebral frontal lobe parietal lobe young woman hx of brain trauma after MVA fx focally dilated right anterior ventricle volume loss frontoparietal region dx trumatic brain injury with gliosis volume loss and ex vacuo changes CTscan Davidoff MD
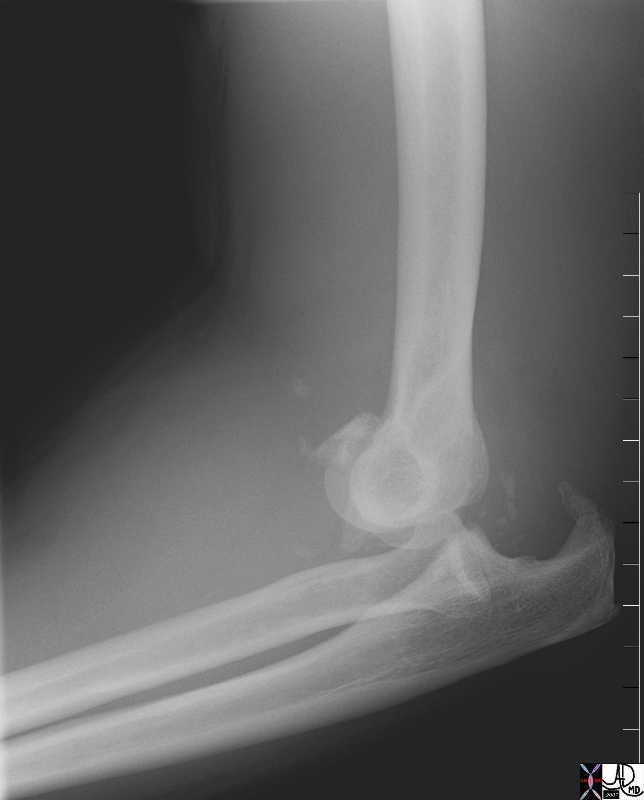
72041.800 elbow bone olecronon fracture humerus ulna radius fx dislocation position trauma plain X-ray Davidoff MD
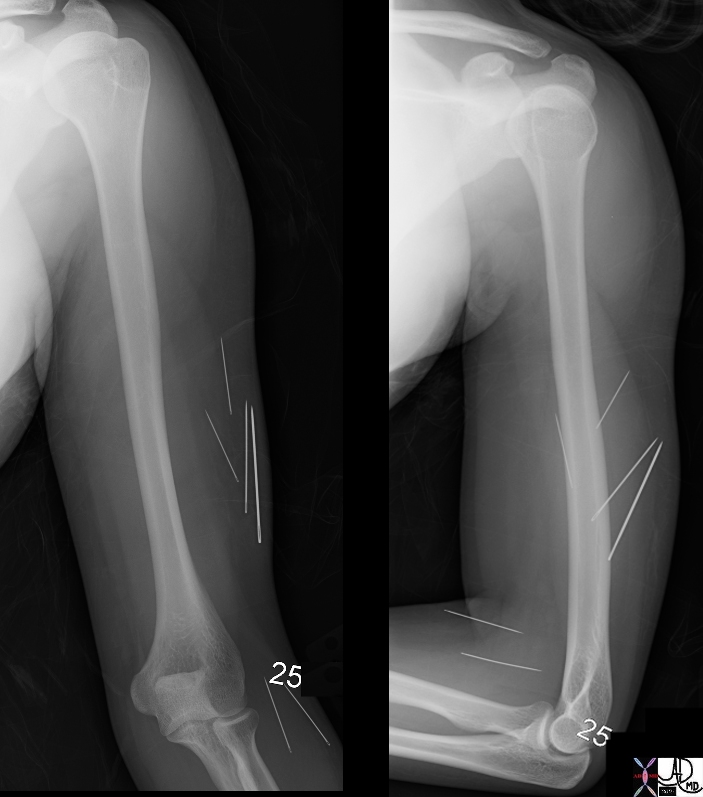
70038c01 humerus bone elbow shoulder soft tissue foreign bodies sewing needles psychiatric illness disorder Davidoff MD

75763c02 75753c01 25 female positive HCG which doubled in 48 hours uterus showed prolifrative endometrium ovary right adnexa right ovary ectopic pregnancy position 2.5cms right ovarian cyst yolk sac gestational sac USscan Courtesy Ashley Davidoff MD
47752c01 61 year olsd female post op repair of ascending aortic aneurysm with Bental procedure with dropping blood pressure and odecreasing oxygen saturation aorta left atrium LA heart cardiacmediastinum fx compression of left atrium from anterior post operative nediastinal hematoma and posterior aneurysm of the descending aorta fx lingula atelectatasis and left lower lobe atelectasis bilateral pleural effusions dx supravalvular mitral stenosis CTscan Davidoff MD
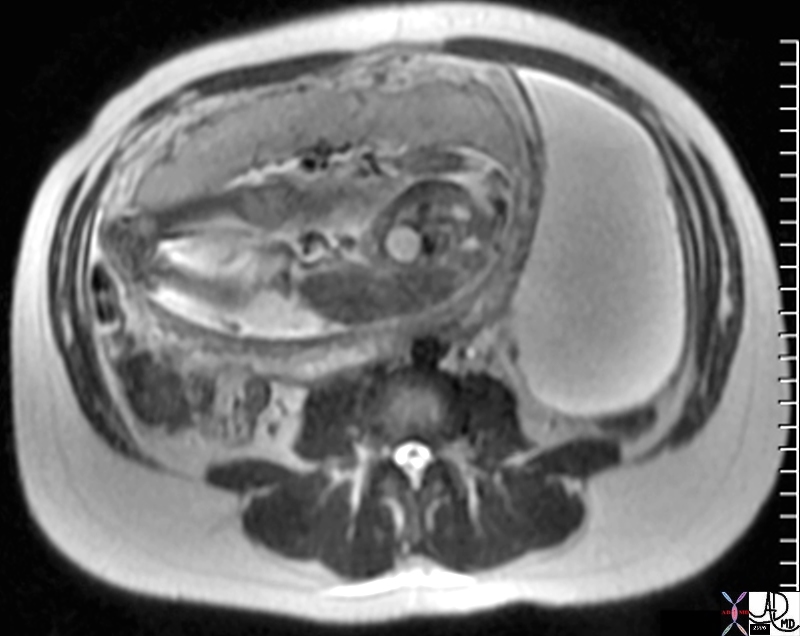
47753 24 week pregnancy ovary OB fetus amniotic sac placenta bladder fx large left ovarian cyst compressed by pregnancy pressure character water T2 bright MRI scan Davidoff MD concepts
Critical Location

70045.800 brain third ventricle foramen of Munro third ventricle headaches, vertigo, memory deficits, diplopia, and behavioral disturbances. smooth, round hyperdense endodermal origin, typically located at the foramen of Munro in the anterior aspect of the third ventricle. T benign filled with gelatinous material and cholesterol crystals cause hyperdensity potential complication can cause hydrocephalus by obstructing third ventricle usual Rx is surgery CTscan Davidoff MD
Position in Treatment

72440 small bowel duodenum proximal jejenum valvulae conniventes ligament of Treitz G-J tube gastrojejunal feeding tube device treatment nutrition prevents reflux plain film of the abdomen contrast X-ray Davidoff MD