Definition
Athersclerosis is a degenerative disorder of the vascular wall characterised by a fibrofatty deposition (plaque) in the inner liningof the artery.
Cause: It occurs as a normal course of aging, but it is accelerated by genetic, dietary and behavioral factors.
Result: The accumulation of plaque in the wall causes narrowing of the lumen of the arteries progressively restricting flow. In addition, the normal smooth and glistening lining of the arteries are replaced by a rough irregular inner wall that is a factor that predisposes to thrombosis, sometimes an acute life threatening event if the arteries of the heart or brain are affected.
Diagnosis: The clinical presentation depends on the organ involved and the degree of narrowing. In the heart for example simple narrowing results in chest pain called angina. When total acute obstruction occurs with thrombosis of the artery, severe unremitting chest pain occurs, and myocardial infarction ensues.Each organ has varied manifestations of clinical presentation, all relating to reduced perfusion of the end organ due to narrowing. Imaging plays an essential role in diagnosis. Ultrasound can directly view the lumen and wall of accesible vessels, while CTscan and MRI are advancing to be the mainstay of diagnosis for the deeper arteries. Angiography was the gold standard of the past, is still used and is invaluable in selected circumstances, particulalrly if therapeutic intervention is needed.
Treatment is usually directed at maintaining flow to the end organs. Medical therapy is often directed at the smooth muscle components of the vessel wall in order to dilate the vesels. Minimally invasive methods use angioplasty and stents to expand the narrowing directly, while surgery often employs bypass methods.
Atherosclerosis |
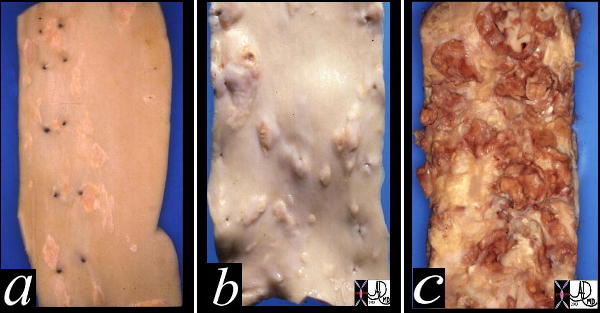
| This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro |
Principles
Structure

Normal Arterial Wall – Histology |
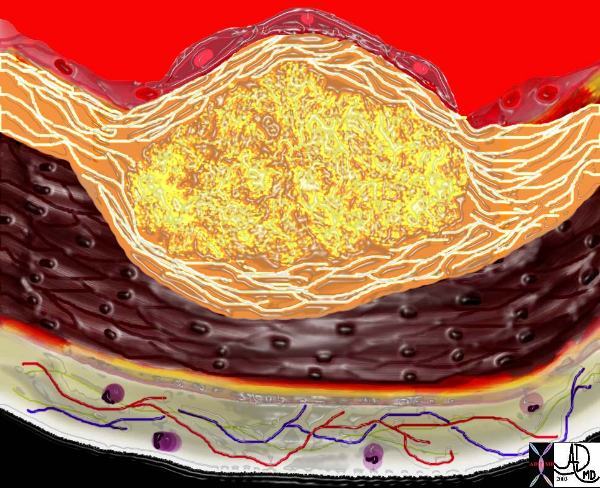
| This image shows the lumen (red) single layer of the inner lining called the endothelium (pink) the muscular wall of a medium sized artery (maroon) and the yellow outer lining called the adventitia. There arelipoprotein molecules normally in the lumen. (yellow)The next step in atherogenesis is the accumulation of these lipoprotein molecules in the intima. Courtesy Ashley Davidoff MD. 33789 code heart artery wall histology normal drawing pathogenesis atherosclerosis atheroma |
Atheromatous plaque is an accumulation of fatty and fibrous elements within the intima of the arterial wall. The multifactorial causes of atherosclerosis include age, sex, genetics, lifestyle and dietary factors. among many other unfolding factors. The recognizable “phases” of atherosclerosis include ; 1) breach of the endothelium (33792d) 2) migration of lipoproteins from the lumen into the intima. (33792d) 3) Formation of a lipoprotein-proteoglycan complex that traps the lipoprotein in the intima (33792e) 4) Migration of leukocytes from the lumen into the intima. (33792g) 5) Transformation of the monocytes into macrophages and phagocytosis of the fat complexes to form fat laden foamy macrophages. (33792h) 6) Migration of smooth muscle cells from the media into the intima and transformation into fibrocytes. A fibrous capsule around the fatty complex is formed. (33792i, 33801b) 7) Cell death and destruction with associated formation of dystrophic calcification. 8) Growth of the atheromatous complex with impingement on the lumen. (33801b) 9) Potential of the complex to rupture. (33801d) The progressive impingement on the lumen causes reduction of blood flow, usually manifesting clinically with angina when the lumen is reduced by 70% of its original size. Acute rupture of a plaque predisposes to superadded thrombosis and occlusion of the lumen. Acute myocardial infarction and death are complications of this event. The initial phase of endothelial injury has multifactorial contributing factors including hypertension, hemodynamic factors, hyperlipidemia, homocysteine, smoking, toxins, immune reactions, and viral disease. The result is a breach in the intima and migration of lipoproteins into the subendothelial layer. The lipoproteins and proteoglycans form a complex compound that traps the fat complex in the subepithelial layer. The next phase heralds the migration of leukocytes and platelets into the subendothelial layer. The monocytes, phagocytose the lipoprotein-proteoglycan complex forming the lipid laden foamy histiocytes. These macrophages can apparently repllicate. At this stage the macroscopic appearance is the well known “fatty streak”. The next phase of atherosclerosis occurs following smooth muscle proliferation and migration from the media into the evolving plaque. Smooth muscle also undergoes apoptosis and death. The vascular smooth muscle produces the extracellular matrix has major contribution to the atheromatous lesion. Interstitial collagens (types I and III) and proteoglycans such and elastin fibers also accumulate in atherosclerotic plaques. Accumlation of cholesterol and cholesterol esters occur. Smooth muscle migrates from the media into the intima and transform into fibrous elements both within the lesion as well superficial to the lesion forming a fibrous plaque.The monocytes and macrophages ingest the fat and foamy fat laden macrophages result. An inflammatory reaction evolves. Continued accumulation of lipid, macrophages, foamy cells, extracellular matrix result in a fibrofatty complex that grows in size over time. As it enlarges it bulges and thins the intima and eventually erodes the surface. As the disease progresses, cell death within the plaque results, and dystrophic calcification follows. ****** needs revision The American Heart Association classification divides atherosclerotic lesions into six types; foam cells ( fatty dots) – Type I fatty streaks, – Type II atheromas, – Type III fibroatheromas, – Type IV complicated lesions (Stary)

The circulating lipoproteins enter a breached endothelium (2) and enter the subendothelial layer of supporting connective tissue within which are linear starands of proteoglycan. (3). At this stage the media (4) is quiescent. Courtesy Ashley Davidoff MD 33792d code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
atheroma drawing
  The Aging ArteryAn Observation by da Vinci The Aging ArteryAn Observation by da Vinci |
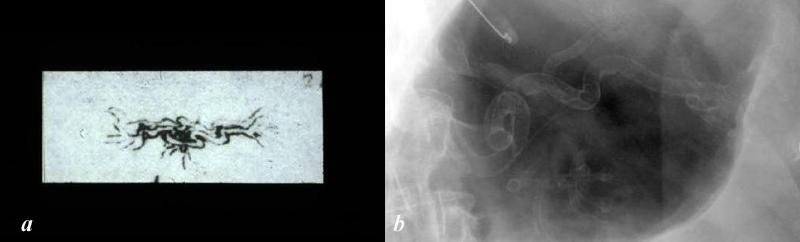
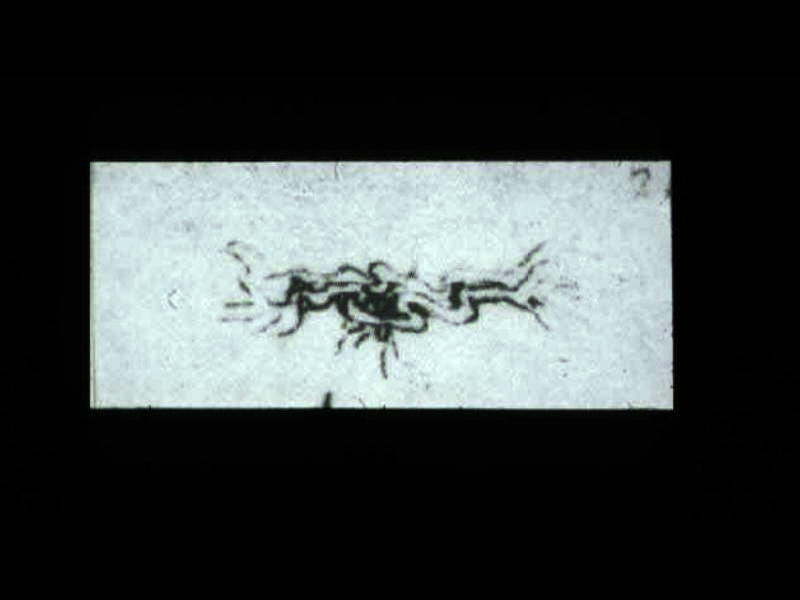
| The drawing of the ?meseraic vessels? ? presumably the celiac axis is by Leonardo da Vinci. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuous state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow. The translation of da Vinci?s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis historical da Vinci) Image b is a magnified view of the left upper quadrant showing a calcified serpiginous splenic artery much like the atherosclerotic vessel described by da Vinci.Courtesy Ashley Davidoff MD 13045b da Vinci diagram 113318c.8L |
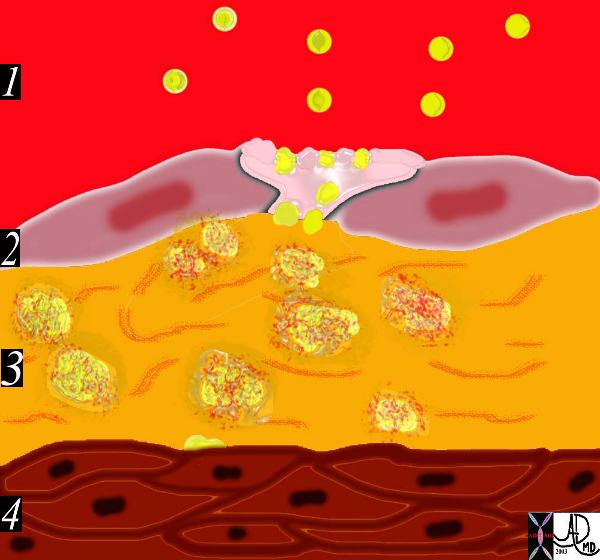
This diagram shows the yellow spheroidal lipoproteins traverse the injured epithelium (2) from the lumen (red) and binding to the linear shaped proteoglycan molecules in the intimal layer. (3) In essence the lipoprotein is ?captured?, because it has been altered structurally and is unable to return to the circulation. Courtesy Ashley Davidoff MD. 33792e code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
 The diagram shows an evolving atheromatous plaque with inflammatory cells, monocytes, and lymphocytes infiltrating the intima which contains the lipoprotein- proteoglycan complex, extracellular lipid , and cholesterol crystals. 33792g Courtesy Ashley Davidoff MD. code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
The diagram shows an evolving atheromatous plaque with inflammatory cells, monocytes, and lymphocytes infiltrating the intima which contains the lipoprotein- proteoglycan complex, extracellular lipid , and cholesterol crystals. 33792g Courtesy Ashley Davidoff MD. code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
 This drawing shows migration of the monocytes into the intima. These monocytes transform into macrophages in the intima and phagocytose the lipid products to become lipid laden foamy cells. The macroscopic correlate at this stage is the fatty streak. Courtesy Ashley Davidoff MD 33792h . code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
This drawing shows migration of the monocytes into the intima. These monocytes transform into macrophages in the intima and phagocytose the lipid products to become lipid laden foamy cells. The macroscopic correlate at this stage is the fatty streak. Courtesy Ashley Davidoff MD 33792h . code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing

This diagram shows the reaction of the smooth muscle cells (b) to the formation of foam cells (a) in the subendothelial layer of the intima. The smooth muscle cells migrate from the muscular layer (4) into the intima. Here they undergo dedifferentiation into fibrocytes. 33792i Courtesy Ashley Davidoff MD. code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing

The diagram shows the atherosclerotic lesion in the subepithelial layer of the intima which at first bulges toward the media or muscular layer. 33801a Courtesy Ashley Davidoff MD. code heart artery intima endothelium histopathology pathogenesis atherosclerosis atheroma drawing
The diagram shows the atherosclerotic lesion in the subepithelial layer of the intima which is bulging both toward the media and toward the lumen. There is a central core of fat and necrotic debris, surrounded by fibrous elements which give the plaque its hardness to the feel. The accumulation of fibrous tissue heralds an advanced atherosclerotic lesion. 33801b Courtesy Ashley Davidoff MD. code heart artery atherosclerosis
Davidoff MD. code heart artery

Mild Coronary Atherosclerosis
|
| 74888 heart cardiac artery ramus medianus coronary artery circumflex coronary artery LAD left anterior descending coronary artery mild atherosclerosis calcific plaques CTscan volume rendering 3D Courtesy Ashley Davidoff MD |
|
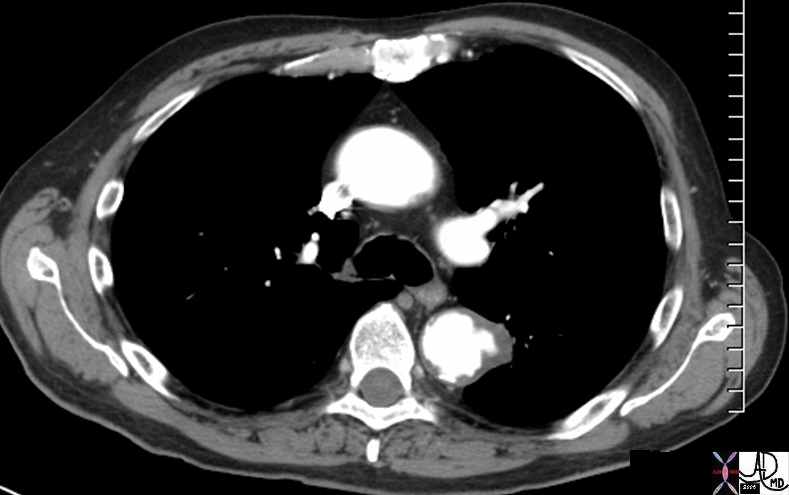
Penetrating Ulcer |
| 48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD |
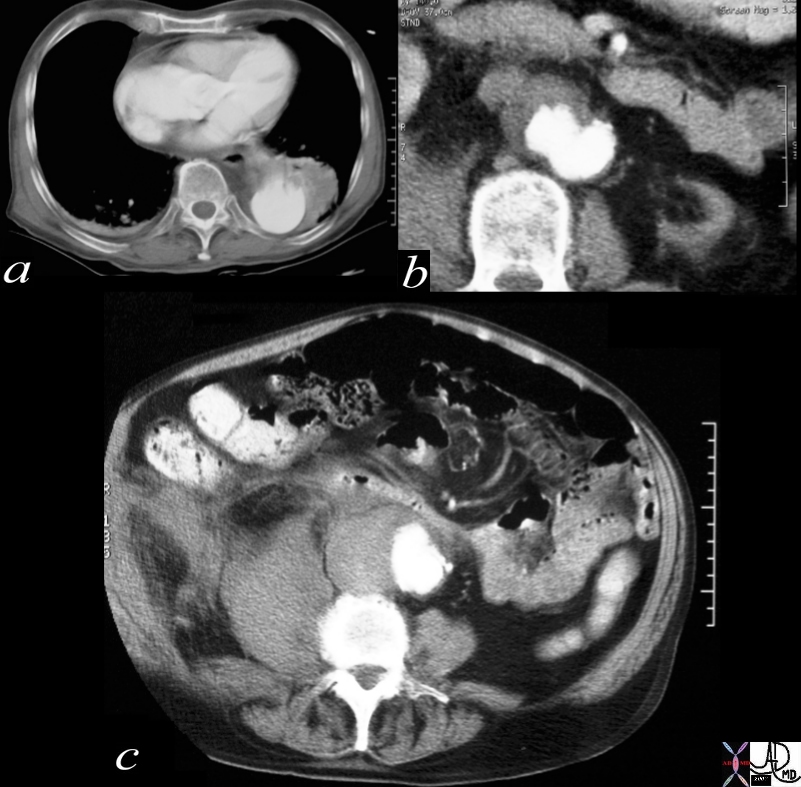
Penetrating Ulcer with Rupture
|
| 17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD |

Devastating Effects of Diabetes – aberrant glucose metabolism |
|
This image reveals the devastating manifestations of aberrant glucose metabolism as a result of insulin insufficiency, with consequent effects on the small vessels throughout the body. In this instance the diabetic arteriopathy is characterised by calcific atherosclerotic diease seen as calcification of the digital artery in b with subsequent ischemia to the foot. The poor nutrition has resulted in infection and ulceration of skin and bone, with poor healing and a need to amputate irrecovarable tissues.
48471c01 foot phalanx phalanges toes digital artery bone fx amputation calcified calcification of arteries dx diabetic arteriopathy chronic ischemia complicated by ulceration infection osteomyelitis treated with amputation diabetes mellitus metabolic disorder plain X-Ray of the foot Courtesy Ashley Davidoff MD |
Serpiginous Splenic Artery – Da Vinci |
| This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the dessicated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Serpiginous Splenic Artery – Da Vinci
This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the dessicated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Serpiginous Splenic Artery – Da Vinci
This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the dessicated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the dessicated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the dessicated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Serpiginous Splenic Artery – Da Vinci
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Serpiginous Splenic Artery – Da Vinci
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Devastating Effects of Diabetes – aberrant glucose metabolism
This image reveals the devastating manifestations of aberrant glucose metabolism as a result of insulin insufficiency, with consequent effects on the small vessels throughout the body. In this instance the diabetic arteriopathy is characterised by calcific atherosclerotic diease seen as calcification of the digital artery in b with subsequent ischemia to the foot. The poor nutrition has resulted in infection and ulceration of skin and bone, with poor healing and a need to amputate irrecovarable tissues.
48471c01 foot phalanx phalanges toes digital artery bone fx amputation calcified calcification of arteries dx diabetic arteriopathy chronic ischemia complicated by ulceration infection osteomyelitis treated with amputation diabetes mellitus metabolic disorder plain X-Ray of the foot Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Devastating Effects of Diabetes – aberrant glucose metabolism
This image reveals the devastating manifestations of aberrant glucose metabolism as a result of insulin insufficiency, with consequent effects on the small vessels throughout the body. In this instance the diabetic arteriopathy is characterised by calcific atherosclerotic diease seen as calcification of the digital artery in b with subsequent ischemia to the foot. The poor nutrition has resulted in infection and ulceration of skin and bone, with poor healing and a need to amputate irrecovarable tissues.
48471c01 foot phalanx phalanges toes digital artery bone fx amputation calcified calcification of arteries dx diabetic arteriopathy chronic ischemia complicated by ulceration infection osteomyelitis treated with amputation diabetes mellitus metabolic disorder plain X-Ray of the foot Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This image reveals the devastating manifestations of aberrant glucose metabolism as a result of insulin insufficiency, with consequent effects on the small vessels throughout the body. In this instance the diabetic arteriopathy is characterised by calcific atherosclerotic diease seen as calcification of the digital artery in b with subsequent ischemia to the foot. The poor nutrition has resulted in infection and ulceration of skin and bone, with poor healing and a need to amputate irrecovarable tissues.
48471c01 foot phalanx phalanges toes digital artery bone fx amputation calcified calcification of arteries dx diabetic arteriopathy chronic ischemia complicated by ulceration infection osteomyelitis treated with amputation diabetes mellitus metabolic disorder plain X-Ray of the foot Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This image reveals the devastating manifestations of aberrant glucose metabolism as a result of insulin insufficiency, with consequent effects on the small vessels throughout the body. In this instance the diabetic arteriopathy is characterised by calcific atherosclerotic diease seen as calcification of the digital artery in b with subsequent ischemia to the foot. The poor nutrition has resulted in infection and ulceration of skin and bone, with poor healing and a need to amputate irrecovarable tissues.
48471c01 foot phalanx phalanges toes digital artery bone fx amputation calcified calcification of arteries dx diabetic arteriopathy chronic ischemia complicated by ulceration infection osteomyelitis treated with amputation diabetes mellitus metabolic disorder plain X-Ray of the foot Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Devastating Effects of Diabetes – aberrant glucose metabolism
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Devastating Effects of Diabetes – aberrant glucose metabolism
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Penetrating Ulcer with Rupture
17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Penetrating Ulcer with Rupture
17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Penetrating Ulcer with Rupture
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Penetrating Ulcer with Rupture
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Penetrating Ulcer
48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Penetrating Ulcer
48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Penetrating Ulcer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Penetrating Ulcer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Mild Coronary Atherosclerosis
74888 heart cardiac artery ramus medianus coronary artery circumflex coronary artery LAD left anterior descending coronary artery mild atherosclerosis calcific plaques CTscan volume rendering 3D Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Mild Coronary Atherosclerosis
74888 heart cardiac artery ramus medianus coronary artery circumflex coronary artery LAD left anterior descending coronary artery mild atherosclerosis calcific plaques CTscan volume rendering 3D Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 74888 heart cardiac artery ramus medianus coronary artery circumflex coronary artery LAD left anterior descending coronary artery mild atherosclerosis calcific plaques CTscan volume rendering 3D Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 74888 heart cardiac artery ramus medianus coronary artery circumflex coronary artery LAD left anterior descending coronary artery mild atherosclerosis calcific plaques CTscan volume rendering 3D Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Mild Coronary Atherosclerosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Mild Coronary Atherosclerosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Aging ArteryAn Observation by da Vinci
The drawing of the ?meseraic vessels? ? presumably the celiac axis is by Leonardo da Vinci. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuous state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow. The translation of da Vinci?s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis historical da Vinci) Image b is a magnified view of the left upper quadrant showing a calcified serpiginous splenic artery much like the atherosclerotic vessel described by da Vinci.Courtesy Ashley Davidoff MD 13045b da Vinci diagram 113318c.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Aging ArteryAn Observation by da Vinci
The drawing of the ?meseraic vessels? ? presumably the celiac axis is by Leonardo da Vinci. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuous state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow. The translation of da Vinci?s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis historical da Vinci) Image b is a magnified view of the left upper quadrant showing a calcified serpiginous splenic artery much like the atherosclerotic vessel described by da Vinci.Courtesy Ashley Davidoff MD 13045b da Vinci diagram 113318c.8L
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The drawing of the ?meseraic vessels? ? presumably the celiac axis is by Leonardo da Vinci. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuous state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow. The translation of da Vinci?s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis historical da Vinci) Image b is a magnified view of the left upper quadrant showing a calcified serpiginous splenic artery much like the atherosclerotic vessel described by da Vinci.Courtesy Ashley Davidoff MD 13045b da Vinci diagram 113318c.8L
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The drawing of the ?meseraic vessels? ? presumably the celiac axis is by Leonardo da Vinci. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuous state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow. The translation of da Vinci?s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis historical da Vinci) Image b is a magnified view of the left upper quadrant showing a calcified serpiginous splenic artery much like the atherosclerotic vessel described by da Vinci.Courtesy Ashley Davidoff MD 13045b da Vinci diagram 113318c.8L
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The Aging ArteryAn Observation by da Vinci
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The Aging ArteryAn Observation by da Vinci
)
https://beta.thecommonvein.net/wp-content/uploads/2024/02/113318c.8L.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/09/13045b.jpg
http://www.thecommonvein.net/shaypz/wp-content/uploads/2014/09/113318c.8L.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Arterial Wall – Histology
This image shows the lumen (red) single layer of the inner lining called the endothelium (pink) the muscular wall of a medium sized artery (maroon) and the yellow outer lining called the adventitia. There arelipoprotein molecules normally in the lumen. (yellow)The next step in atherogenesis is the accumulation of these lipoprotein molecules in the intima. Courtesy Ashley Davidoff MD. 33789 code heart artery wall histology normal drawing pathogenesis atherosclerosis atheroma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Arterial Wall – Histology
This image shows the lumen (red) single layer of the inner lining called the endothelium (pink) the muscular wall of a medium sized artery (maroon) and the yellow outer lining called the adventitia. There arelipoprotein molecules normally in the lumen. (yellow)The next step in atherogenesis is the accumulation of these lipoprotein molecules in the intima. Courtesy Ashley Davidoff MD. 33789 code heart artery wall histology normal drawing pathogenesis atherosclerosis atheroma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This image shows the lumen (red) single layer of the inner lining called the endothelium (pink) the muscular wall of a medium sized artery (maroon) and the yellow outer lining called the adventitia. There arelipoprotein molecules normally in the lumen. (yellow)The next step in atherogenesis is the accumulation of these lipoprotein molecules in the intima. Courtesy Ashley Davidoff MD. 33789 code heart artery wall histology normal drawing pathogenesis atherosclerosis atheroma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This image shows the lumen (red) single layer of the inner lining called the endothelium (pink) the muscular wall of a medium sized artery (maroon) and the yellow outer lining called the adventitia. There arelipoprotein molecules normally in the lumen. (yellow)The next step in atherogenesis is the accumulation of these lipoprotein molecules in the intima. Courtesy Ashley Davidoff MD. 33789 code heart artery wall histology normal drawing pathogenesis atherosclerosis atheroma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Arterial Wall – Histology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Arterial Wall – Histology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
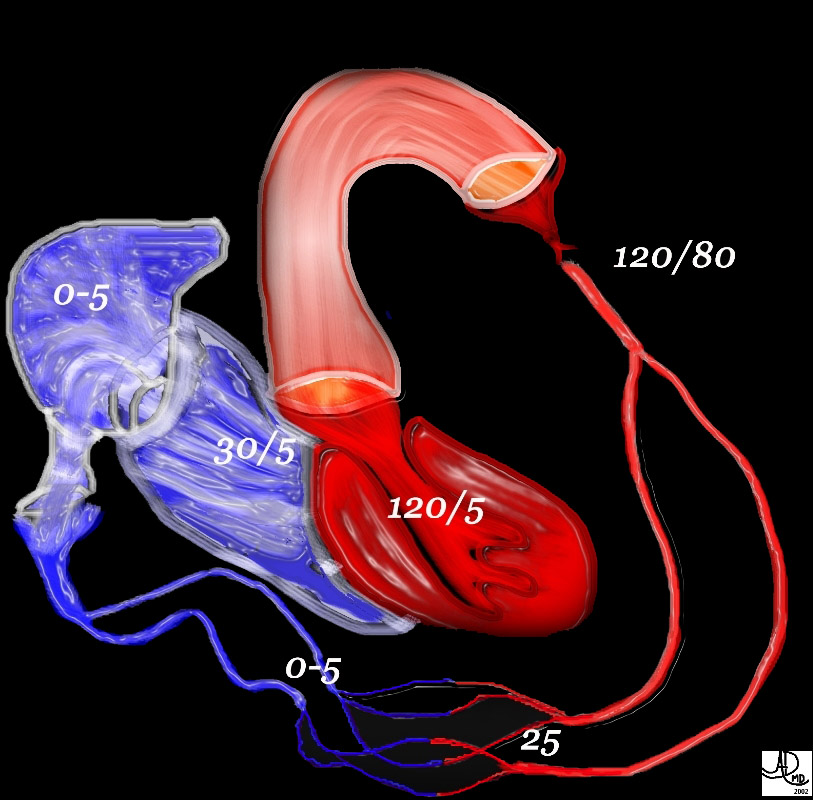
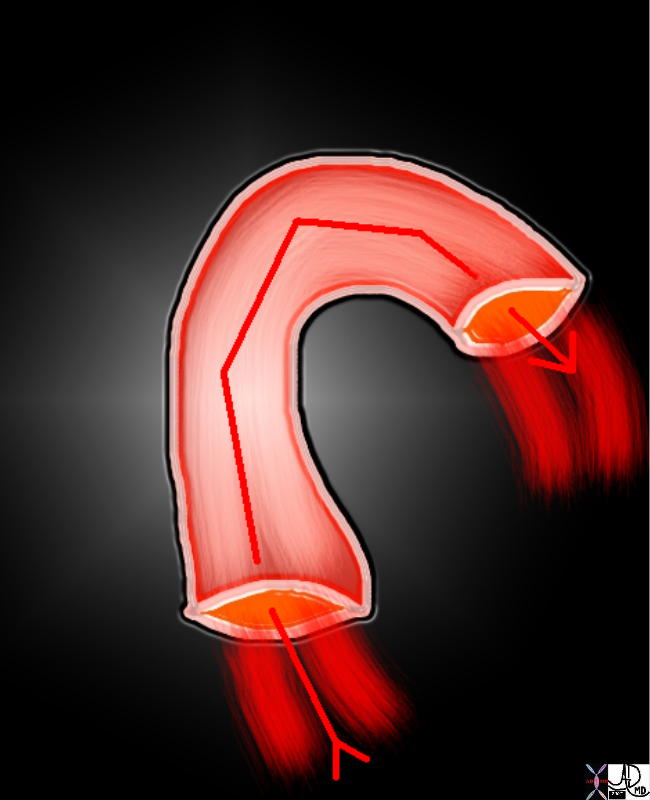
A Simple Tube
72845.800 aorta flow principles structure laminar flow turbulent flow normal Davidoff Art Courtesy Ashley Davidoff MD 72835.800 72839 72831.800 72845.800 49483b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
A Simple Tube
72845.800 aorta flow principles structure laminar flow turbulent flow normal Davidoff Art Courtesy Ashley Davidoff MD 72835.800 72839 72831.800 72845.800 49483b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 72845.800 aorta flow principles structure laminar flow turbulent flow normal Davidoff Art Courtesy Ashley Davidoff MD 72835.800 72839 72831.800 72845.800 49483b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72845.800 aorta flow principles structure laminar flow turbulent flow normal Davidoff Art Courtesy Ashley Davidoff MD 72835.800 72839 72831.800 72845.800 49483b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
A Simple Tube
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A Simple Tube
)
https://beta.thecommonvein.net/wp-content/uploads/2023/09/72835.800.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/09/72845.800.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/09/72831.800.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/09/49483b01.jpg https://beta.thecommonvein.net/wp-content/uploads/2023/09/72839.jpg
http://thecommonvein.net/media/72845.800.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Atherosclerosis
This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Atherosclerosis
This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Atherosclerosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Atherosclerosis
)