
DWI
Ashley Davidoff MD
The Common Vein Copyright 2010
Introduction

Acute Infarction Right Parietal and Right temporal Lobe |
|
The diffusion weighted MRI in axial projection shows a high intensity region in the right parietal and right temporal region revealing an acute infarction poattern in these regions reflecting right middle cerebral artery territory. Note that the basal ganglia have been spared, but the insula and operculum are involved. Courtesy Ashley Davidoff MD Copyright 2010 71275c01c03 |
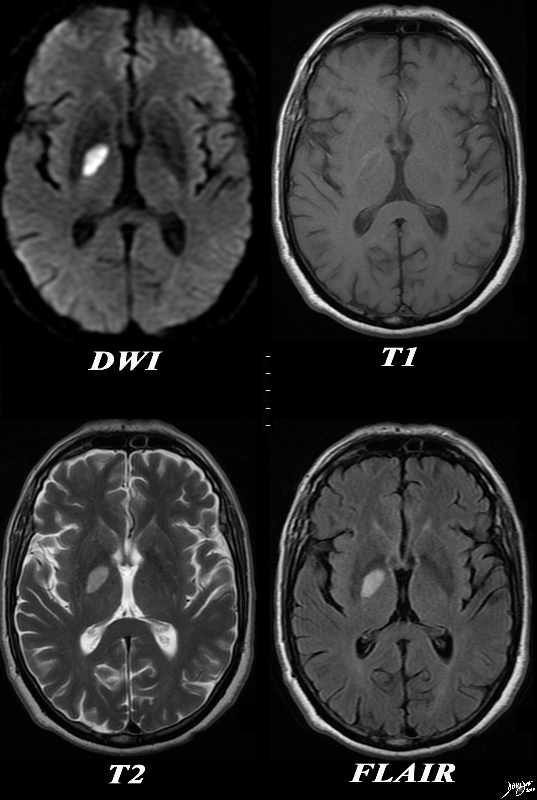
Acute Infarction of the Right Globus Pallidus |
|
The basal ganglia with an abnormality in the right globus pallidus are shown in axial projection in the MRI of a 64 year old male who presents with acute neurological deficit. In the first image a high intensity region in the right globus pallidus is shown in axial projection on DWI consistent with an acute infarction. The second image is a T1 weighted image without contrast and shows a rim of high intensity suggesting rim hemorrhage.. The third T2 weighted image shows the lesion to be bright but not as bright as CSF a finding consistent with the acute infarction. The fourth image is a FLAIR image and also shows increased intensity of the lesion. The constellation of findings is consistent with an acute infarction of the right globus pallidus with a rim of acute hemorrhage. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89087c01.8s |

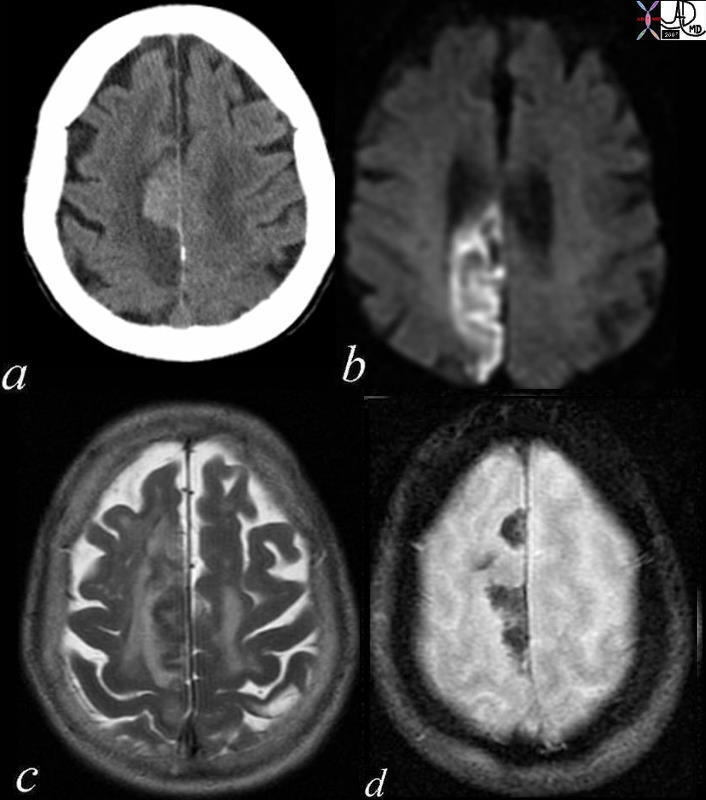
Acute Thalamastriate Infarction |
|
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s |
|
Acute Embolic Infarct High Parietal Region |
|
The axial images are from a patient with atrial fibrillation and neurological deficits. Image a is a CT scan which shows a high density lesion i the vertex of the right pariettal lobe suggesting hemorhagic change. Image b is a diffusion weighted MRI image at the level of the ventricles which shows a high intensity region in the parieto-occipital region suggesting acute infarction. Image c is a axial T2 weighted image showing edema in the white matter of the right parietal lobe. Image is aGRE image showing mixed heterogeneity with probable iron deposition suggesting subacute or chronic hemorhage. Findings are consistent with old and new multicentric infarcts of the brain likely from the heart caused by atrial fibrillation Courtesy Ashley Davidoff MD copyright 2010 71239c01 |
|
Multicentric Infarcts – Carotid Stenosis |
|
The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex. Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction. Courtesy Ashley Davidoff MD Copyright 2010 72014c01 |

Acute Hemorrhagic Infarct |
| The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci.
Courtesy Ashley Davidoff MD copyright 2010 46098c01.800 |
|
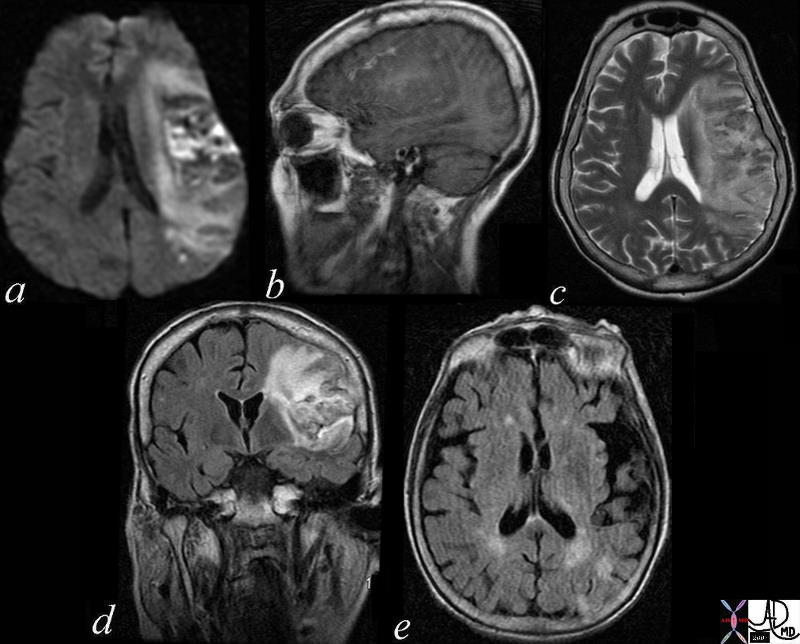
Subacute hemmorrhagic Infarct of the Parietal Lobe MRI |
|
The series of MRI images from a 70 year old male who by history suffered a stroke 1 month ago and has new onset symptoms. the series of images reveal complex changes of a subacute hemorrhagic infarct. Image a is from a DWI sequence and it shows a heterogenous increase in signal some of which represents T2 shine throughand sopme of which is bright raising the question on an acute on subacute entity. Image b is a sagittal T1 weighted image which shows areas of vague increase in density suggesting hemorrhage. Image c is a T2weighted sequence and shows some increase in water but the granular low intensity suggests hemosiderin deposit. Image d is FLAIR sequence showing increase brightness to the lesion in the left parietal lobe and image e is an axial FLAIR sequence The findings suggest extensive infarct in the left MCA territory which has mild mass effect on ventricles with petechial hemorrhage as seen on T2 and FLAIR and hyperintense T2 shine through on diffusion weighted images The punctate areas in left parietal lobe with restricted area of diffusion raises the question of a recent small infarct less bright regions on DWI suggests a subacute hemorrhagic infarct. Courtesy Ashley Davidoff MD Copyright 2010 71000c03 |
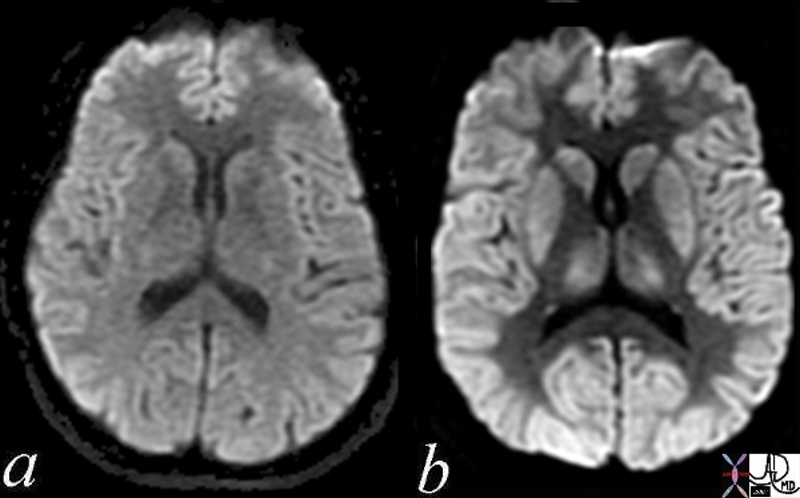
Normal (a) and Acute Global Ischemia (b) |
|
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Brownian motion of the affected area and the image can be manipulated to present this as a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a) Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 49433c02.800 |
|
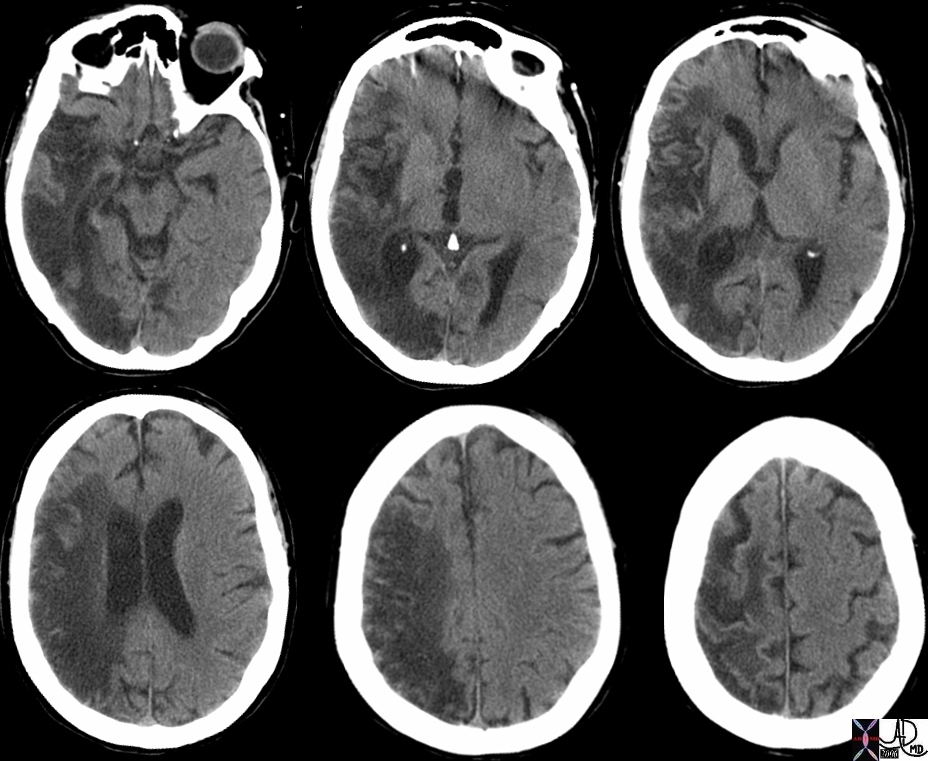
Chronic Parietal Infarction – CT scan |
|
The CT scan shows the effects of an extensive right middle cerebral infarct and involves the right parietal lobe, temporal lobe, and occipital lobe. The right lateral ventricle is enlarged because of the loss of brain tissue as a result of the infarction. This process is called encephalomalacia (brain softening) and the changes are called ex vacuo changes because the loss of tissue results in gain of space resulting in the shift of the ventricle into the space. Courtesy Ashley Davidoff MD copyright 2010 46031c |
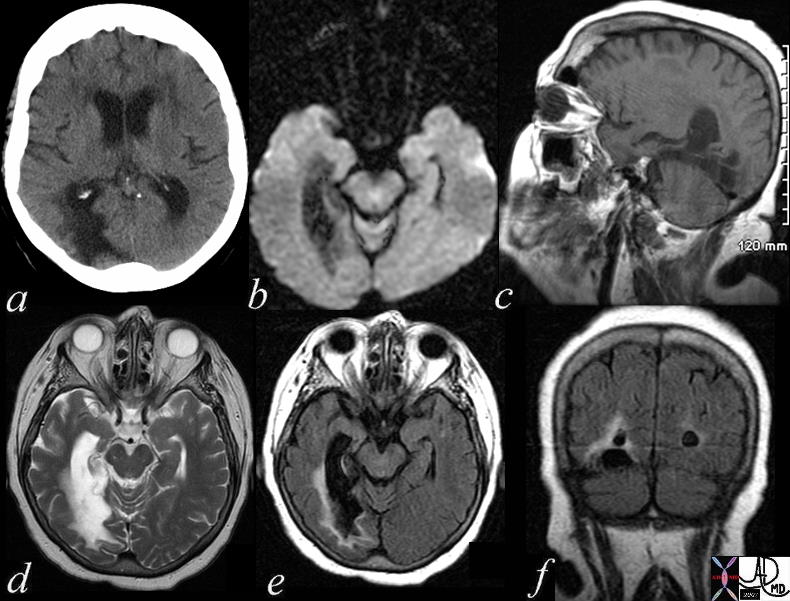
Chronic Infarction |
|
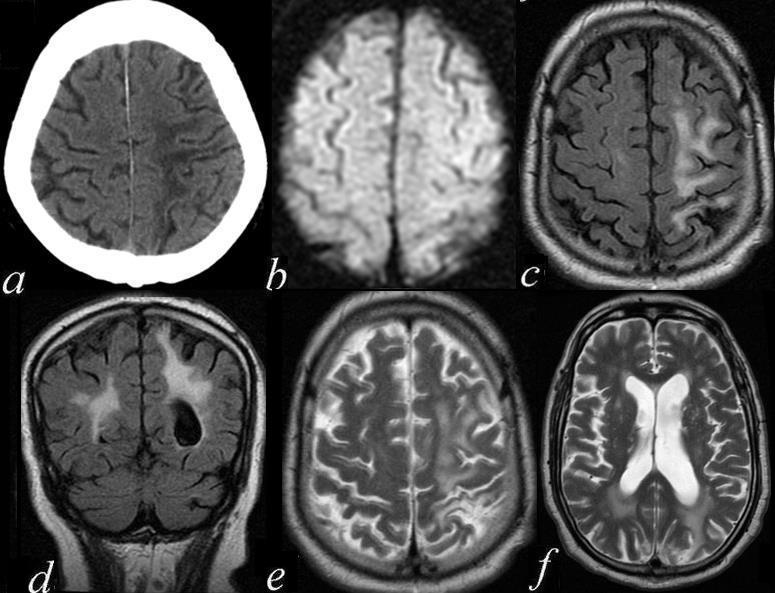
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800 |
 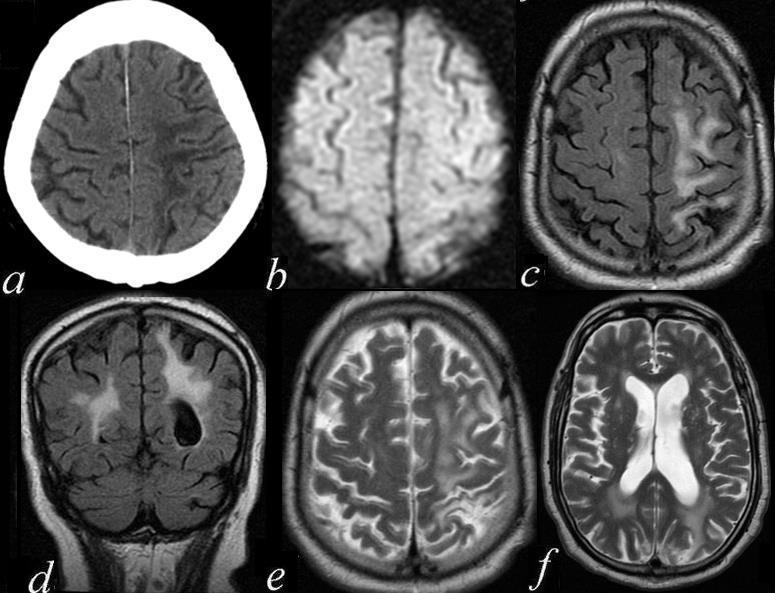
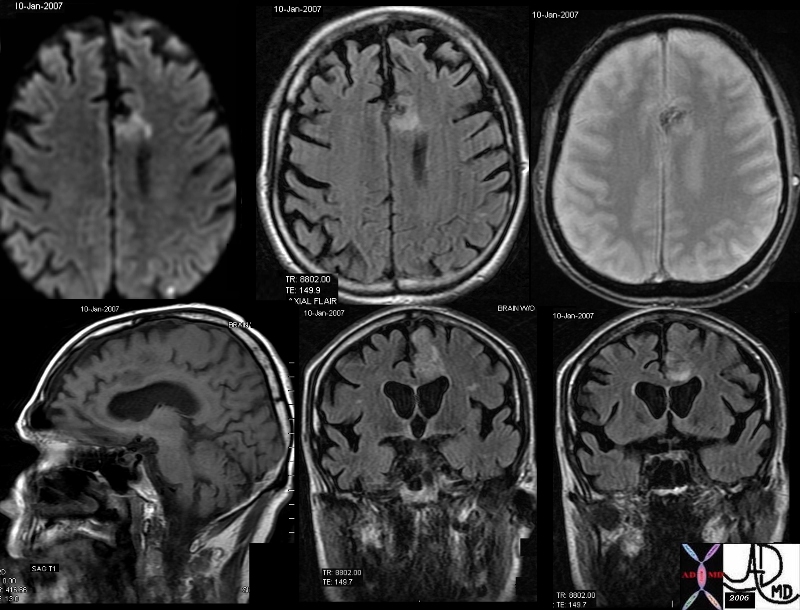
Chronic Parietal Infarction with Encephalomalacia |
|
The series of axial and coronal images are from a 74 year old man with mental status changes. Image a is an axial CT scan showing a region of white matter hypodensity over the high parietal region. Image b is a DWI image that shows no abnormality in the region thus excluding an acute infarct. Image c is a FLAIR sequence in the axial plane and image d is a FLAIR seqience in the coronal plane suggesting increase water in the white matter of the high left parietal region confirmed by the T2 weighted sequence of e. The last axial image is a T2 weighted sequence through the ventricles showing that the left lateral ventricle is larger than the right. These findings suggest a chronic left MCA infarct with gliosis, encephalomalacia and ex vacuo changes. 71411c01.801 Courtesy Ashley Davidoff MD 71411c01.800 |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Parietal Infarction with Encephalomalacia
The series of axial and coronal images are from a 74 year old man with mental status changes. Image a is an axial CT scan showing a region of white matter hypodensity over the high parietal region. Image b is a DWI image that shows no abnormality in the region thus excluding an acute infarct. Image c is a FLAIR sequence in the axial plane and image d is a FLAIR seqience in the coronal plane suggesting increase water in the white matter of the high left parietal region confirmed by the T2 weighted sequence of e. The last axial image is a T2 weighted sequence through the ventricles showing that the left lateral ventricle is larger than the right.
These findings suggest a chronic left MCA infarct with gliosis, encephalomalacia and ex vacuo changes.
71411c01.801 Courtesy Ashley Davidoff MD 71411c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Parietal Infarction with Encephalomalacia
The series of axial and coronal images are from a 74 year old man with mental status changes. Image a is an axial CT scan showing a region of white matter hypodensity over the high parietal region. Image b is a DWI image that shows no abnormality in the region thus excluding an acute infarct. Image c is a FLAIR sequence in the axial plane and image d is a FLAIR seqience in the coronal plane suggesting increase water in the white matter of the high left parietal region confirmed by the T2 weighted sequence of e. The last axial image is a T2 weighted sequence through the ventricles showing that the left lateral ventricle is larger than the right.
These findings suggest a chronic left MCA infarct with gliosis, encephalomalacia and ex vacuo changes.
71411c01.801 Courtesy Ashley Davidoff MD 71411c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The series of axial and coronal images are from a 74 year old man with mental status changes. Image a is an axial CT scan showing a region of white matter hypodensity over the high parietal region. Image b is a DWI image that shows no abnormality in the region thus excluding an acute infarct. Image c is a FLAIR sequence in the axial plane and image d is a FLAIR seqience in the coronal plane suggesting increase water in the white matter of the high left parietal region confirmed by the T2 weighted sequence of e. The last axial image is a T2 weighted sequence through the ventricles showing that the left lateral ventricle is larger than the right.
These findings suggest a chronic left MCA infarct with gliosis, encephalomalacia and ex vacuo changes.
71411c01.801 Courtesy Ashley Davidoff MD 71411c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The series of axial and coronal images are from a 74 year old man with mental status changes. Image a is an axial CT scan showing a region of white matter hypodensity over the high parietal region. Image b is a DWI image that shows no abnormality in the region thus excluding an acute infarct. Image c is a FLAIR sequence in the axial plane and image d is a FLAIR seqience in the coronal plane suggesting increase water in the white matter of the high left parietal region confirmed by the T2 weighted sequence of e. The last axial image is a T2 weighted sequence through the ventricles showing that the left lateral ventricle is larger than the right.
These findings suggest a chronic left MCA infarct with gliosis, encephalomalacia and ex vacuo changes.
71411c01.801 Courtesy Ashley Davidoff MD 71411c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Parietal Infarction with Encephalomalacia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Parietal Infarction with Encephalomalacia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Infarction
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Infarction
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The patient is a 74 year old female with a history of ataxia, incontinence, and memory loss. The MRI shows features of a chronic infarction in the right posterior cerebral artery territory affecting the posteromedial aspect of right temporal lobe and medial and inferior aspect of the right occipital lobe. There is evidence of gliosis with volume loss, atrophy, and encephalomalacia resulting in ex vacuo changes with dilatation of temporal and occipital horns of the lateral ventricles. Image a is a CTscan showing encephalomalacia in the right posterior temporal region and ex vacuo change with ventricular dilatation. Image b is a DWI scan showing no acute changes. Image c is a T1 weighted sagittal view showing no acute hemorrhage. Image d is a T2 weighted study showing compound high intensity changes in the region of the occipital horn but the distinction between disease and dilated ventricle cannot be made because of blooming and isointensity of the ventrciles and the diseases cerebral tissue. Image e is a FLAIR image that turns the CSF black and enables the identification of the high intensity abnormal brain tissue that is smaller than expected after reviewing the T2 weighted image. This case reveals the importance of the FLAIR image. Image f is a coronal FLAIR sequence also showing that the actual dimension of diseased tissue is relatively small. The findings are consistent with an old chronic infarction.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71419c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Infarction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Infarction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Parietal Infarction – CT scan
The CT scan shows the effects of an extensive right middle cerebral infarct and involves the right parietal lobe, temporal lobe, and occipital lobe. The right lateral ventricle is enlarged because of the loss of brain tissue as a result of the infarction. This process is called encephalomalacia (brain softening) and the changes are called ex vacuo changes because the loss of tissue results in gain of space resulting in the shift of the ventricle into the space.
Courtesy Ashley Davidoff MD copyright 2010 46031c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Parietal Infarction – CT scan
The CT scan shows the effects of an extensive right middle cerebral infarct and involves the right parietal lobe, temporal lobe, and occipital lobe. The right lateral ventricle is enlarged because of the loss of brain tissue as a result of the infarction. This process is called encephalomalacia (brain softening) and the changes are called ex vacuo changes because the loss of tissue results in gain of space resulting in the shift of the ventricle into the space.
Courtesy Ashley Davidoff MD copyright 2010 46031c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT scan shows the effects of an extensive right middle cerebral infarct and involves the right parietal lobe, temporal lobe, and occipital lobe. The right lateral ventricle is enlarged because of the loss of brain tissue as a result of the infarction. This process is called encephalomalacia (brain softening) and the changes are called ex vacuo changes because the loss of tissue results in gain of space resulting in the shift of the ventricle into the space.
Courtesy Ashley Davidoff MD copyright 2010 46031c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT scan shows the effects of an extensive right middle cerebral infarct and involves the right parietal lobe, temporal lobe, and occipital lobe. The right lateral ventricle is enlarged because of the loss of brain tissue as a result of the infarction. This process is called encephalomalacia (brain softening) and the changes are called ex vacuo changes because the loss of tissue results in gain of space resulting in the shift of the ventricle into the space.
Courtesy Ashley Davidoff MD copyright 2010 46031c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Parietal Infarction – CT scan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Parietal Infarction – CT scan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal (a) and Acute Global Ischemia (b)
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Brownian motion of the affected area and the image can be manipulated to present this as a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 49433c02.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal (a) and Acute Global Ischemia (b)
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Brownian motion of the affected area and the image can be manipulated to present this as a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 49433c02.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Brownian motion of the affected area and the image can be manipulated to present this as a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 49433c02.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Brownian motion of the affected area and the image can be manipulated to present this as a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 49433c02.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal (a) and Acute Global Ischemia (b)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal (a) and Acute Global Ischemia (b)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Subacute hemmorrhagic Infarct of the Parietal Lobe MRI
The series of MRI images from a 70 year old male who by history suffered a stroke 1 month ago and has new onset symptoms. the series of images reveal complex changes of a subacute hemorrhagic infarct. Image a is from a DWI sequence and it shows a heterogenous increase in signal some of which represents T2 shine throughand sopme of which is bright raising the question on an acute on subacute entity. Image b is a sagittal T1 weighted image which shows areas of vague increase in density suggesting hemorrhage. Image c is a T2weighted sequence and shows some increase in water but the granular low intensity suggests hemosiderin deposit. Image d is FLAIR sequence showing increase brightness to the lesion in the left parietal lobe and image e is an axial FLAIR sequence The findings suggest extensive infarct in the left MCA territory which has mild mass effect on ventricles with petechial hemorrhage as seen on T2 and FLAIR and hyperintense T2 shine through on diffusion weighted images The punctate areas in left parietal lobe with restricted area of diffusion raises the question of a recent small infarct less bright regions on DWI suggests a subacute hemorrhagic infarct.
Courtesy Ashley Davidoff MD Copyright 2010 71000c03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Subacute hemmorrhagic Infarct of the Parietal Lobe MRI
The series of MRI images from a 70 year old male who by history suffered a stroke 1 month ago and has new onset symptoms. the series of images reveal complex changes of a subacute hemorrhagic infarct. Image a is from a DWI sequence and it shows a heterogenous increase in signal some of which represents T2 shine throughand sopme of which is bright raising the question on an acute on subacute entity. Image b is a sagittal T1 weighted image which shows areas of vague increase in density suggesting hemorrhage. Image c is a T2weighted sequence and shows some increase in water but the granular low intensity suggests hemosiderin deposit. Image d is FLAIR sequence showing increase brightness to the lesion in the left parietal lobe and image e is an axial FLAIR sequence The findings suggest extensive infarct in the left MCA territory which has mild mass effect on ventricles with petechial hemorrhage as seen on T2 and FLAIR and hyperintense T2 shine through on diffusion weighted images The punctate areas in left parietal lobe with restricted area of diffusion raises the question of a recent small infarct less bright regions on DWI suggests a subacute hemorrhagic infarct.
Courtesy Ashley Davidoff MD Copyright 2010 71000c03
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The series of MRI images from a 70 year old male who by history suffered a stroke 1 month ago and has new onset symptoms. the series of images reveal complex changes of a subacute hemorrhagic infarct. Image a is from a DWI sequence and it shows a heterogenous increase in signal some of which represents T2 shine throughand sopme of which is bright raising the question on an acute on subacute entity. Image b is a sagittal T1 weighted image which shows areas of vague increase in density suggesting hemorrhage. Image c is a T2weighted sequence and shows some increase in water but the granular low intensity suggests hemosiderin deposit. Image d is FLAIR sequence showing increase brightness to the lesion in the left parietal lobe and image e is an axial FLAIR sequence The findings suggest extensive infarct in the left MCA territory which has mild mass effect on ventricles with petechial hemorrhage as seen on T2 and FLAIR and hyperintense T2 shine through on diffusion weighted images The punctate areas in left parietal lobe with restricted area of diffusion raises the question of a recent small infarct less bright regions on DWI suggests a subacute hemorrhagic infarct.
Courtesy Ashley Davidoff MD Copyright 2010 71000c03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The series of MRI images from a 70 year old male who by history suffered a stroke 1 month ago and has new onset symptoms. the series of images reveal complex changes of a subacute hemorrhagic infarct. Image a is from a DWI sequence and it shows a heterogenous increase in signal some of which represents T2 shine throughand sopme of which is bright raising the question on an acute on subacute entity. Image b is a sagittal T1 weighted image which shows areas of vague increase in density suggesting hemorrhage. Image c is a T2weighted sequence and shows some increase in water but the granular low intensity suggests hemosiderin deposit. Image d is FLAIR sequence showing increase brightness to the lesion in the left parietal lobe and image e is an axial FLAIR sequence The findings suggest extensive infarct in the left MCA territory which has mild mass effect on ventricles with petechial hemorrhage as seen on T2 and FLAIR and hyperintense T2 shine through on diffusion weighted images The punctate areas in left parietal lobe with restricted area of diffusion raises the question of a recent small infarct less bright regions on DWI suggests a subacute hemorrhagic infarct.
Courtesy Ashley Davidoff MD Copyright 2010 71000c03
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Subacute hemmorrhagic Infarct of the Parietal Lobe MRI
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Subacute hemmorrhagic Infarct of the Parietal Lobe MRI
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Hemorrhagic Infarct
The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci.
Courtesy Ashley Davidoff MD copyright 2010 46098c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Hemorrhagic Infarct
The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci.
Courtesy Ashley Davidoff MD copyright 2010 46098c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci.
Courtesy Ashley Davidoff MD copyright 2010 46098c01.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci.
Courtesy Ashley Davidoff MD copyright 2010 46098c01.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Hemorrhagic Infarct
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Hemorrhagic Infarct
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Multicentric Infarcts – Carotid Stenosis
The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex.
Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction.
Courtesy Ashley Davidoff MD Copyright 2010 72014c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Multicentric Infarcts – Carotid Stenosis
The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex.
Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction.
Courtesy Ashley Davidoff MD Copyright 2010 72014c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex.
Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction.
Courtesy Ashley Davidoff MD Copyright 2010 72014c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The images reveal multicentric acute infarcts in the left cerebral hemisphere involving the internal capsule and left parietal lobe cortex.
Image a is the DWI sequence and the high intensity foci are diagnostic of acute infarction. Image b is a T2 weighted image that reflects increase water in the high intensity regions. Image c is an axial FLAIR and d a coronal FLAIR sequence both sensitive to the regions of infarct and characerized by high intensity foci in the regions of acute infarction.
Courtesy Ashley Davidoff MD Copyright 2010 72014c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Multicentric Infarcts – Carotid Stenosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Multicentric Infarcts – Carotid Stenosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Embolic Infarct High Parietal Region
The axial images are from a patient with atrial fibrillation and neurological deficits.
Image a is a CT scan which shows a high density lesion i the vertex of the right pariettal lobe suggesting hemorhagic change.
Image b is a diffusion weighted MRI image at the level of the ventricles which shows a high intensity region in the parieto-occipital region suggesting acute infarction.
Image c is a axial T2 weighted image showing edema in the white matter of the right parietal lobe.
Image is aGRE image showing mixed heterogeneity with probable iron deposition suggesting subacute or chronic hemorhage.
Findings are consistent with old and new multicentric infarcts of the brain likely from the heart caused by atrial fibrillation
Courtesy Ashley Davidoff MD copyright 2010 71239c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Embolic Infarct High Parietal Region
The axial images are from a patient with atrial fibrillation and neurological deficits.
Image a is a CT scan which shows a high density lesion i the vertex of the right pariettal lobe suggesting hemorhagic change.
Image b is a diffusion weighted MRI image at the level of the ventricles which shows a high intensity region in the parieto-occipital region suggesting acute infarction.
Image c is a axial T2 weighted image showing edema in the white matter of the right parietal lobe.
Image is aGRE image showing mixed heterogeneity with probable iron deposition suggesting subacute or chronic hemorhage.
Findings are consistent with old and new multicentric infarcts of the brain likely from the heart caused by atrial fibrillation
Courtesy Ashley Davidoff MD copyright 2010 71239c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 7
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The axial images are from a patient with atrial fibrillation and neurological deficits.
Image a is a CT scan which shows a high density lesion i the vertex of the right pariettal lobe suggesting hemorhagic change.
Image b is a diffusion weighted MRI image at the level of the ventricles which shows a high intensity region in the parieto-occipital region suggesting acute infarction.
Image c is a axial T2 weighted image showing edema in the white matter of the right parietal lobe.
Image is aGRE image showing mixed heterogeneity with probable iron deposition suggesting subacute or chronic hemorhage.
Findings are consistent with old and new multicentric infarcts of the brain likely from the heart caused by atrial fibrillation
Courtesy Ashley Davidoff MD copyright 2010 71239c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The axial images are from a patient with atrial fibrillation and neurological deficits.
Image a is a CT scan which shows a high density lesion i the vertex of the right pariettal lobe suggesting hemorhagic change.
Image b is a diffusion weighted MRI image at the level of the ventricles which shows a high intensity region in the parieto-occipital region suggesting acute infarction.
Image c is a axial T2 weighted image showing edema in the white matter of the right parietal lobe.
Image is aGRE image showing mixed heterogeneity with probable iron deposition suggesting subacute or chronic hemorhage.
Findings are consistent with old and new multicentric infarcts of the brain likely from the heart caused by atrial fibrillation
Courtesy Ashley Davidoff MD copyright 2010 71239c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Embolic Infarct High Parietal Region
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Embolic Infarct High Parietal Region
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Thalamastriate Infarction
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Thalamastriate Infarction
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT and MRI images are from an 82 year old make with acute neurological deficit. An acute infarction is shown that involves territory within and beyond the basal ganglia. In the CTscan two low density regions are seen medial to the Sylvian fissure and medial to the insular cortex, likely involving the putamen and the part of the right caudate nucleus as well as some white matter in right middle cerebra;l territory. In the second image a high intensity region in the putamen and part of the caudate nucleus is shown together with an area that does not involve the basal ganglia more posteriorly, likely part of the white matter of the right parietal lobe shown in an axial projection on DWI consistent with an acute infarction. The third image is an axial FLAIR sequence and shows the area of parenchymal edema with presumed central necrosis, while the image at low right shows the periventricular disease to better advantage. The constellation of findings is consistent with an acute infarction with distribution of the lenticulostriate vessels arising from the right middle cerebral territory
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89367c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Thalamastriate Infarction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Thalamastriate Infarction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Infarction of the Right Globus Pallidus
The basal ganglia with an abnormality in the right globus pallidus are shown in axial projection in the MRI of a 64 year old male who presents with acute neurological deficit. In the first image a high intensity region in the right globus pallidus is shown in axial projection on DWI consistent with an acute infarction. The second image is a T1 weighted image without contrast and shows a rim of high intensity suggesting rim hemorrhage.. The third T2 weighted image shows the lesion to be bright but not as bright as CSF a finding consistent with the acute infarction. The fourth image is a FLAIR image and also shows increased intensity of the lesion. The constellation of findings is consistent with an acute infarction of the right globus pallidus with a rim of acute hemorrhage.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89087c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Infarction of the Right Globus Pallidus
The basal ganglia with an abnormality in the right globus pallidus are shown in axial projection in the MRI of a 64 year old male who presents with acute neurological deficit. In the first image a high intensity region in the right globus pallidus is shown in axial projection on DWI consistent with an acute infarction. The second image is a T1 weighted image without contrast and shows a rim of high intensity suggesting rim hemorrhage.. The third T2 weighted image shows the lesion to be bright but not as bright as CSF a finding consistent with the acute infarction. The fourth image is a FLAIR image and also shows increased intensity of the lesion. The constellation of findings is consistent with an acute infarction of the right globus pallidus with a rim of acute hemorrhage.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89087c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The basal ganglia with an abnormality in the right globus pallidus are shown in axial projection in the MRI of a 64 year old male who presents with acute neurological deficit. In the first image a high intensity region in the right globus pallidus is shown in axial projection on DWI consistent with an acute infarction. The second image is a T1 weighted image without contrast and shows a rim of high intensity suggesting rim hemorrhage.. The third T2 weighted image shows the lesion to be bright but not as bright as CSF a finding consistent with the acute infarction. The fourth image is a FLAIR image and also shows increased intensity of the lesion. The constellation of findings is consistent with an acute infarction of the right globus pallidus with a rim of acute hemorrhage.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89087c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The basal ganglia with an abnormality in the right globus pallidus are shown in axial projection in the MRI of a 64 year old male who presents with acute neurological deficit. In the first image a high intensity region in the right globus pallidus is shown in axial projection on DWI consistent with an acute infarction. The second image is a T1 weighted image without contrast and shows a rim of high intensity suggesting rim hemorrhage.. The third T2 weighted image shows the lesion to be bright but not as bright as CSF a finding consistent with the acute infarction. The fourth image is a FLAIR image and also shows increased intensity of the lesion. The constellation of findings is consistent with an acute infarction of the right globus pallidus with a rim of acute hemorrhage.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 89087c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Infarction of the Right Globus Pallidus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Infarction of the Right Globus Pallidus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Infarction Right Parietal and Right temporal Lobe
The diffusion weighted MRI in axial projection shows a high intensity region in the right parietal and right temporal region revealing an acute infarction poattern in these regions reflecting right middle cerebral artery territory. Note that the basal ganglia have been spared, but the insula and operculum are involved.
Courtesy Ashley Davidoff MD Copyright 2010 71275c01c03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Infarction Right Parietal and Right temporal Lobe
The diffusion weighted MRI in axial projection shows a high intensity region in the right parietal and right temporal region revealing an acute infarction poattern in these regions reflecting right middle cerebral artery territory. Note that the basal ganglia have been spared, but the insula and operculum are involved.
Courtesy Ashley Davidoff MD Copyright 2010 71275c01c03
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The diffusion weighted MRI in axial projection shows a high intensity region in the right parietal and right temporal region revealing an acute infarction poattern in these regions reflecting right middle cerebral artery territory. Note that the basal ganglia have been spared, but the insula and operculum are involved.
Courtesy Ashley Davidoff MD Copyright 2010 71275c01c03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The diffusion weighted MRI in axial projection shows a high intensity region in the right parietal and right temporal region revealing an acute infarction poattern in these regions reflecting right middle cerebral artery territory. Note that the basal ganglia have been spared, but the insula and operculum are involved.
Courtesy Ashley Davidoff MD Copyright 2010 71275c01c03
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Infarction Right Parietal and Right temporal Lobe
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Infarction Right Parietal and Right temporal Lobe
)