Both endoderm and mesoderm contribute to the development of the liver, gallbladder and biliary system. In the 4th week of gestation, at the junction of the of the foregut and midgut, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diverticulum . The mesodermal tissue for the liver appears on day 22 and is called septum transversum. This mesodermal tissue contributes to the development of the heart, diaphgragm and liver.
|
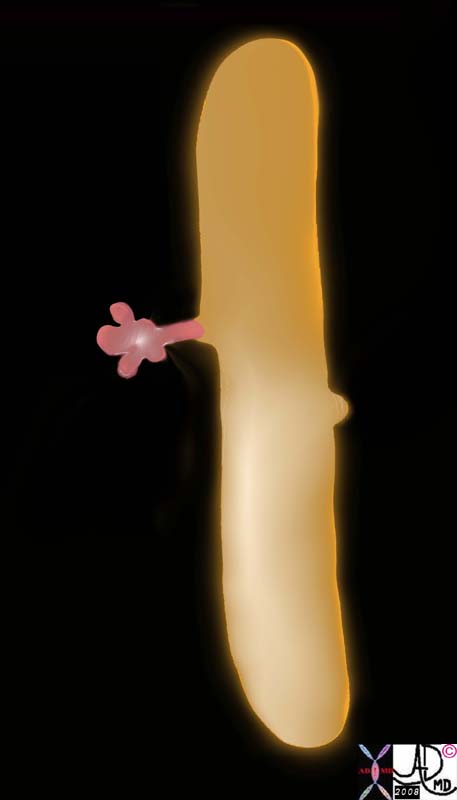 
Hepatic Diverticulum
|
|
In the 4th week of gestation, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diveticulum at the junction of the of the foregut and midgut.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a01b2.8s 82219a02a1.8s |
The hepatic diverticulum has two components; a pars hepatcia and pars cystica. The pars hepatica will evolve into the liver and bile ducts while the pars cystica will develop into the gallbladder and cystic duct. The hepatic bud is initially a solid cord but by week 8 with growth and resorbtion the tubular components are canalized.
|
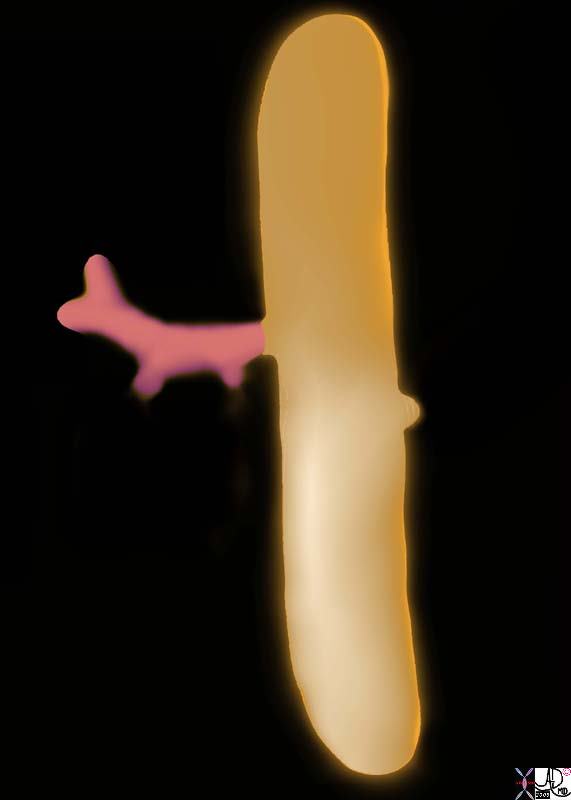
Hepatic Diverticulum
|
|
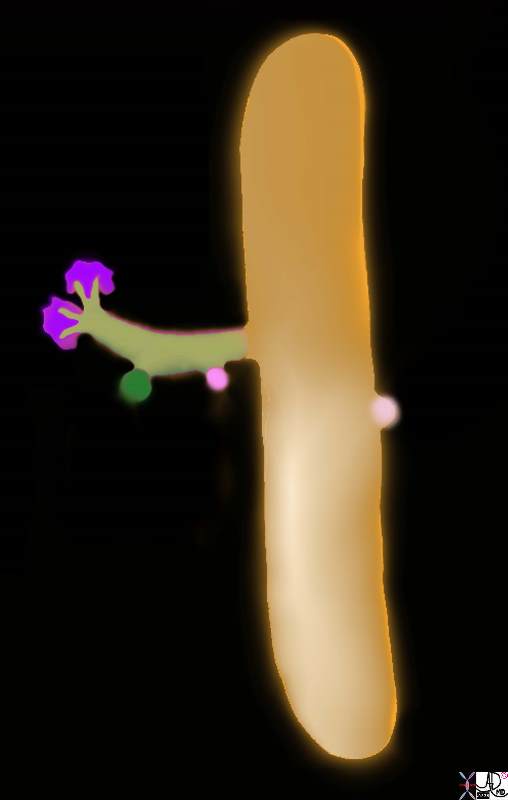
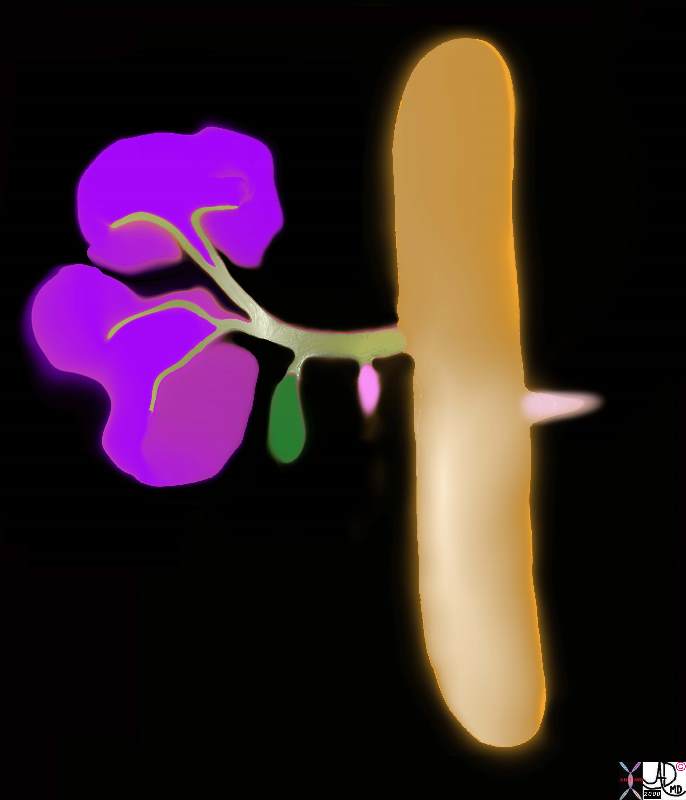
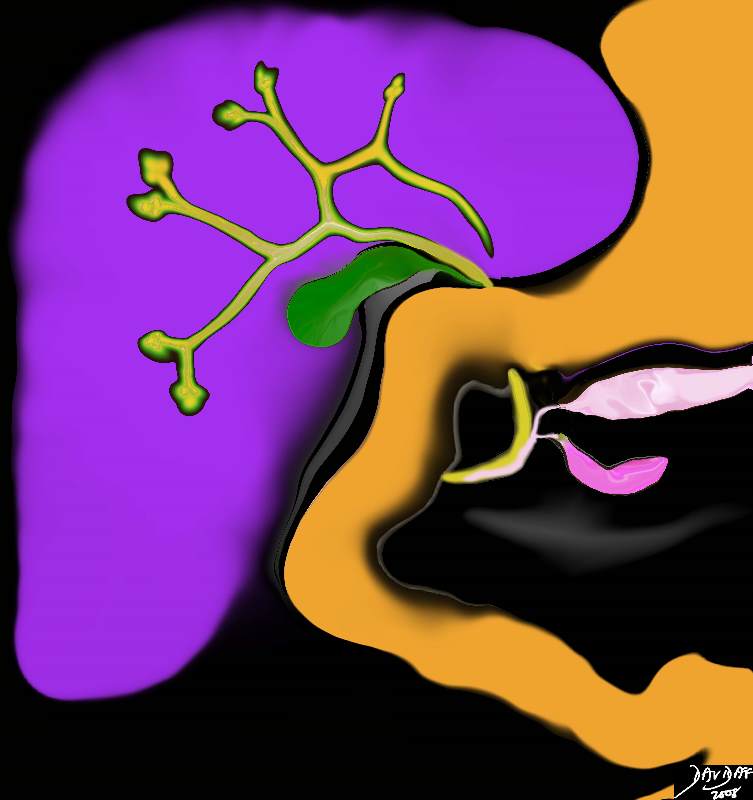
Aftter the 4th week of gestation, the primitive endoderm continues to differentiate and grow. The hepatic diverticulum is the precursor for the liver bile ducts and gallbladder. At the same time mesodermal tissue from the septum transversum (purple) is available in the right upper quadrant, and the hepatic diverticulum grows into the mesederm. The pars cystica (green) will become the gallbladder and the the ventral portion of the pancreas (dark pink) is part of the endodermal outgrowth. On the medial side of the foregut the dorsal portion of the pancreas (light pink) evolves.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a02b1.8s 82219a02b3.8s |
Complex interactions between the mesoderm and the epithelial cells of the endoderm take place, but a harmonious marriage between the two systems has to take place in order for the appropriate connections between duct, parenchyma, connective tissue and vessels to evolve.
|

Hepatic Diverticulum
|
| Continued volume growth and and interaction between endoderm and mesoderm result in the enlargement of the evolving liver, gallbladder, pancreas and stomach and duodenum.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219b08.8s |
Additionally a series of growth patterns change the position of the organs. As the stomach grows it rotates to the left. The duodenum grows down and to the right and also rotates to the right. The combination of these three events brings the distal common bile duct, and ventral pancreas to the medial and left side of the duodenum. The distal common bile duct as a result of the rotations courses behind the duodenum, and the biliary pancreatic confluens connects to the middle of the descending duodenum on its medial aspect.
The CBD and Ampulla on the Medial Duodenum
|
| In the 5th week, the duodenum has grown down and to the right, as well as rotated 90 degrees to the right. The stomach rotates to the left. These events bring the pancreatic duct and the CBD to the posterior and medial aspect of the duodenum resulting in the positioning of the ampulla in the mid and medial portion of the descending duodenum.
82219b12.8s liver gallbladder pancreas foregut midgut bile duct cystic duct common bile duct stomach embryology septum transversum mesoderm endoderm 5th week stomach rotated to left duodenum growth |
At the sixth week the extrahepatic biliary system becomes reorganized and recanalizes. At the 7th week the cystic duct recanalizes while the gallbladder recanalizes at a slightly later date.
In a histological study (Haffajee) embryos of 10-13weeks age, demonstrated thickened walls, and contained “crumbly” debris. At 14 weeks bile staining was observed, and the mucosa appeared mature. At 20 weeks bile with mature consistency and color was present.
Thus the gallbladder arises from the foregut, with precursors that are common to the liver and pancreas. it shares primitive tissue with the heart, diaphragm and gastrointestinal tract. It is initially a solid bud, undergoes cavitation, returns to solid form, only to recanalize again, maturing by 10-13 weeks. By 20 weeks mature bile, indicating a mature liver is found in the formed gallbladder.
Applied Biology
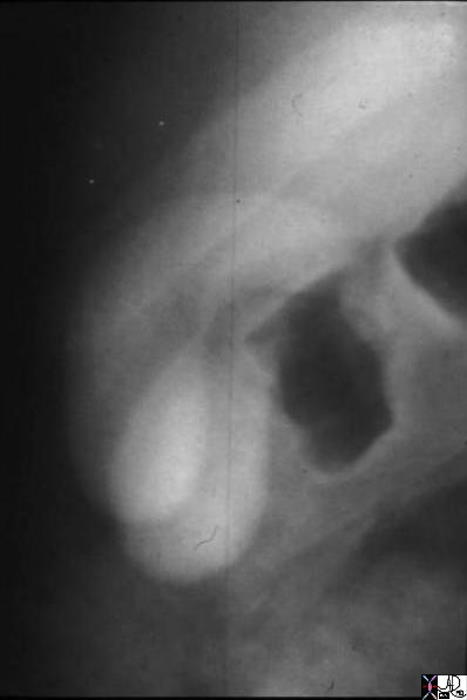
Sometimes the pars cystica, the precursor for the gallbladder, divides in two rather than remaining one entity, forming a duplicated gallbladder usually with one cystic duct. This results in a duplicated gallbladder.
Duplicated Gallbladder
|
|
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD |
Duplicated Gallbladder
|
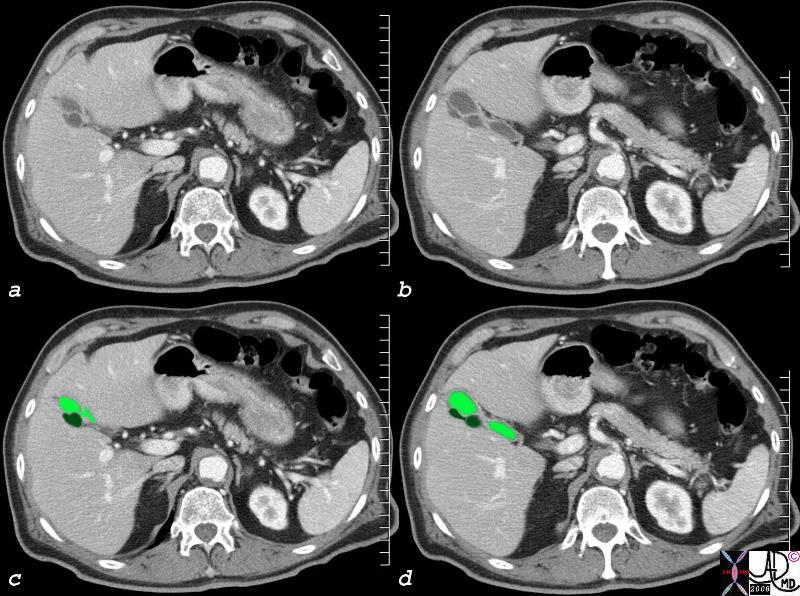
| The CTscan in axial section also shows two gallbladders – a duplicated sytem. It is slightly harder to appreciate the two fundi and bodies. It is impossible to appreciate the cystic duct. The dark green represents the posterior and seemingly smaller gallbladder while the light green reveals the larger anterior gallbladder.
82231c01.8s gallbladder duplicated congenital duplication CTscan Courtesy Ashley Davidoff MD copyright 2008 |
A range of underdevelopment can occur varying from hypoplasia to aplasia. Biliary atresia is a known association with infantile polycystic disease. In biliary atresia the intrahepatic ducts, extrahepatic ducts, and gallbladder are variably involved.
Hypoplastic and Hypoplastic Gallbladder
|
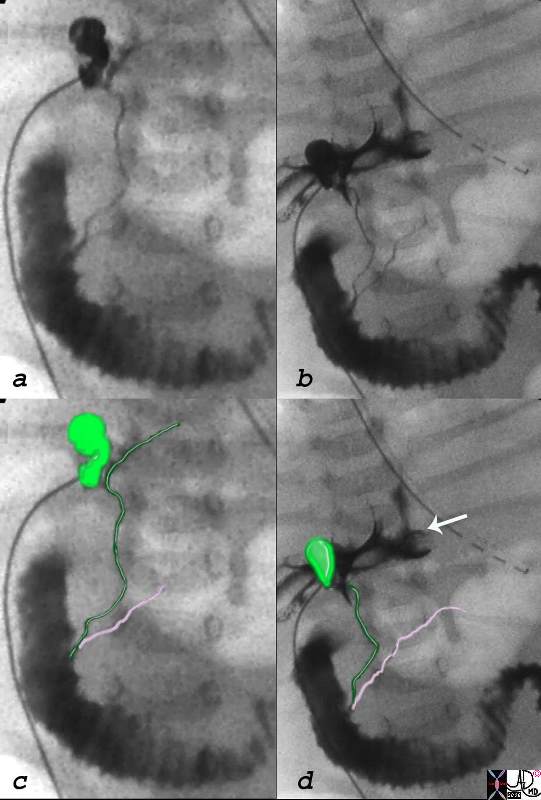
| This percutaneous cholecystogram was performed on a neonate with profound jaundice. A catheter enters the gallbladder directly (seen to the left of images (a,b,c,d) and injection shows filling of a small gallbladder (light green in c,d) and part of the left duct and all the CBD (dark green) and pancreatic duct. (pink) In an attempt to fill the right side and intrahepatic radicles, the persistant injection resulted in overflow of contrast into the subhepatic space (arrow, d) since the intrahepatic system was too small or non existant to accomodarte the contrast. The absence of filling of the intrahepatic radicles is reminiscent of a form biliary atresia. The gallbladder in this case is small and hypoplastic.
28814c02.8s gallbladder small absent hypoplastic intrahepatic bile ducts liver biliary atresia congenital cholangiogram Courtesy Ashley Davidoff MD copyright 2008 |
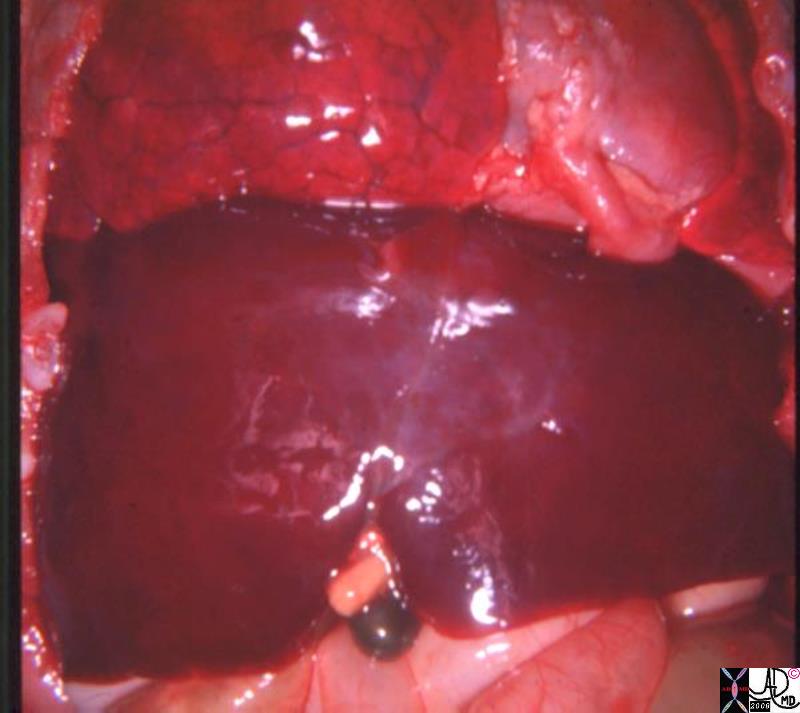
The positioning of the gallbladder is related to the positioning of the liver. In situs inversus of the abdominal organs, the gallbladder is left sided. If there is situs ambiguus, there are usually two large lobes of the liver, reminiscent of two right lobes, with one one on the right and one on the leftside. The ambiguity of the liver also affects the gallbladder and the confounded gallbladder is centrally placed. This entity occurs in the asplenia syndrome.
Central Gallbladder
Situs Ambiguus
|
| In this post mortem specimen of the unfortunate child with asplenia syndrome the gallbladder is noted in the middle of the body. (dark green) This ambiguus position of the gallbladder is coupled in this image with an ambiguus liver that appears to have two large right lobes. The whole entity is combined with other ambiguus anomalies such as bilateral right atria, or bilateral IVC’s for example. Many of these anomalies are incompatible with life.
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008 |
References
Brookes Clinical Embryology: A Color Atlas and Text By Murray Brookes, Anthony Zietman Published by CRC Press, 1998
Meilstrup JW Imaging Atlas of the Normal Gallbladder and Its Variants By Jon W. Meilstrup Published by CRC Press, 1994
Suchy Liver Disease in Children By Frederick J. Suchy, Ronald J. Sokol, William F. Balistreri Published by Lippincott Williams & Wilkins, 2000 **
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Central Gallbladder
Situs Ambiguus
In this post mortem specimen of the unfortunate child with asplenia syndrome the gallbladder is noted in the middle of the body. (dark green) This ambiguus position of the gallbladder is coupled in this image with an ambiguus liver that appears to have two large right lobes. The whole entity is combined with other ambiguus anomalies such as bilateral right atria, or bilateral IVC’s for example. Many of these anomalies are incompatible with life.
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Central Gallbladder
Situs Ambiguus
In this post mortem specimen of the unfortunate child with asplenia syndrome the gallbladder is noted in the middle of the body. (dark green) This ambiguus position of the gallbladder is coupled in this image with an ambiguus liver that appears to have two large right lobes. The whole entity is combined with other ambiguus anomalies such as bilateral right atria, or bilateral IVC’s for example. Many of these anomalies are incompatible with life.
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this post mortem specimen of the unfortunate child with asplenia syndrome the gallbladder is noted in the middle of the body. (dark green) This ambiguus position of the gallbladder is coupled in this image with an ambiguus liver that appears to have two large right lobes. The whole entity is combined with other ambiguus anomalies such as bilateral right atria, or bilateral IVC’s for example. Many of these anomalies are incompatible with life.
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this post mortem specimen of the unfortunate child with asplenia syndrome the gallbladder is noted in the middle of the body. (dark green) This ambiguus position of the gallbladder is coupled in this image with an ambiguus liver that appears to have two large right lobes. The whole entity is combined with other ambiguus anomalies such as bilateral right atria, or bilateral IVC’s for example. Many of these anomalies are incompatible with life.
82222.8s liver gallbladder bilateral right lobe asplenia syndrome Ivemark syndrome central gallbladder situs ambiguus congenital position gross pathology Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Central Gallbladder
Situs Ambiguus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Central Gallbladder
Situs Ambiguus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hypoplastic and Hypoplastic Gallbladder
This percutaneous cholecystogram was performed on a neonate with profound jaundice. A catheter enters the gallbladder directly (seen to the left of images (a,b,c,d) and injection shows filling of a small gallbladder (light green in c,d) and part of the left duct and all the CBD (dark green) and pancreatic duct. (pink) In an attempt to fill the right side and intrahepatic radicles, the persistant injection resulted in overflow of contrast into the subhepatic space (arrow, d) since the intrahepatic system was too small or non existant to accomodarte the contrast. The absence of filling of the intrahepatic radicles is reminiscent of a form biliary atresia. The gallbladder in this case is small and hypoplastic.
28814c02.8s gallbladder small absent hypoplastic intrahepatic bile ducts liver biliary atresia congenital cholangiogram Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hypoplastic and Hypoplastic Gallbladder
This percutaneous cholecystogram was performed on a neonate with profound jaundice. A catheter enters the gallbladder directly (seen to the left of images (a,b,c,d) and injection shows filling of a small gallbladder (light green in c,d) and part of the left duct and all the CBD (dark green) and pancreatic duct. (pink) In an attempt to fill the right side and intrahepatic radicles, the persistant injection resulted in overflow of contrast into the subhepatic space (arrow, d) since the intrahepatic system was too small or non existant to accomodarte the contrast. The absence of filling of the intrahepatic radicles is reminiscent of a form biliary atresia. The gallbladder in this case is small and hypoplastic.
28814c02.8s gallbladder small absent hypoplastic intrahepatic bile ducts liver biliary atresia congenital cholangiogram Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This percutaneous cholecystogram was performed on a neonate with profound jaundice. A catheter enters the gallbladder directly (seen to the left of images (a,b,c,d) and injection shows filling of a small gallbladder (light green in c,d) and part of the left duct and all the CBD (dark green) and pancreatic duct. (pink) In an attempt to fill the right side and intrahepatic radicles, the persistant injection resulted in overflow of contrast into the subhepatic space (arrow, d) since the intrahepatic system was too small or non existant to accomodarte the contrast. The absence of filling of the intrahepatic radicles is reminiscent of a form biliary atresia. The gallbladder in this case is small and hypoplastic.
28814c02.8s gallbladder small absent hypoplastic intrahepatic bile ducts liver biliary atresia congenital cholangiogram Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This percutaneous cholecystogram was performed on a neonate with profound jaundice. A catheter enters the gallbladder directly (seen to the left of images (a,b,c,d) and injection shows filling of a small gallbladder (light green in c,d) and part of the left duct and all the CBD (dark green) and pancreatic duct. (pink) In an attempt to fill the right side and intrahepatic radicles, the persistant injection resulted in overflow of contrast into the subhepatic space (arrow, d) since the intrahepatic system was too small or non existant to accomodarte the contrast. The absence of filling of the intrahepatic radicles is reminiscent of a form biliary atresia. The gallbladder in this case is small and hypoplastic.
28814c02.8s gallbladder small absent hypoplastic intrahepatic bile ducts liver biliary atresia congenital cholangiogram Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hypoplastic and Hypoplastic Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hypoplastic and Hypoplastic Gallbladder
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Duplicated Gallbladder
The CTscan in axial section also shows two gallbladders – a duplicated sytem. It is slightly harder to appreciate the two fundi and bodies. It is impossible to appreciate the cystic duct. The dark green represents the posterior and seemingly smaller gallbladder while the light green reveals the larger anterior gallbladder.
82231c01.8s gallbladder duplicated congenital duplication CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
The CTscan in axial section also shows two gallbladders – a duplicated sytem. It is slightly harder to appreciate the two fundi and bodies. It is impossible to appreciate the cystic duct. The dark green represents the posterior and seemingly smaller gallbladder while the light green reveals the larger anterior gallbladder.
82231c01.8s gallbladder duplicated congenital duplication CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CTscan in axial section also shows two gallbladders – a duplicated sytem. It is slightly harder to appreciate the two fundi and bodies. It is impossible to appreciate the cystic duct. The dark green represents the posterior and seemingly smaller gallbladder while the light green reveals the larger anterior gallbladder.
82231c01.8s gallbladder duplicated congenital duplication CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CTscan in axial section also shows two gallbladders – a duplicated sytem. It is slightly harder to appreciate the two fundi and bodies. It is impossible to appreciate the cystic duct. The dark green represents the posterior and seemingly smaller gallbladder while the light green reveals the larger anterior gallbladder.
82231c01.8s gallbladder duplicated congenital duplication CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Duplicated Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Duplicated Gallbladder
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Duplicated Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The CBD and Ampulla on the Medial Duodenum
In the 5th week, the duodenum has grown down and to the right, as well as rotated 90 degrees to the right. The stomach rotates to the left. These events bring the pancreatic duct and the CBD to the posterior and medial aspect of the duodenum resulting in the positioning of the ampulla in the mid and medial portion of the descending duodenum.
82219b12.8s liver gallbladder pancreas foregut midgut bile duct cystic duct common bile duct stomach embryology septum transversum mesoderm endoderm 5th week stomach rotated to left duodenum growth
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The CBD and Ampulla on the Medial Duodenum
In the 5th week, the duodenum has grown down and to the right, as well as rotated 90 degrees to the right. The stomach rotates to the left. These events bring the pancreatic duct and the CBD to the posterior and medial aspect of the duodenum resulting in the positioning of the ampulla in the mid and medial portion of the descending duodenum.
82219b12.8s liver gallbladder pancreas foregut midgut bile duct cystic duct common bile duct stomach embryology septum transversum mesoderm endoderm 5th week stomach rotated to left duodenum growth
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In the 5th week, the duodenum has grown down and to the right, as well as rotated 90 degrees to the right. The stomach rotates to the left. These events bring the pancreatic duct and the CBD to the posterior and medial aspect of the duodenum resulting in the positioning of the ampulla in the mid and medial portion of the descending duodenum.
82219b12.8s liver gallbladder pancreas foregut midgut bile duct cystic duct common bile duct stomach embryology septum transversum mesoderm endoderm 5th week stomach rotated to left duodenum growth
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In the 5th week, the duodenum has grown down and to the right, as well as rotated 90 degrees to the right. The stomach rotates to the left. These events bring the pancreatic duct and the CBD to the posterior and medial aspect of the duodenum resulting in the positioning of the ampulla in the mid and medial portion of the descending duodenum.
82219b12.8s liver gallbladder pancreas foregut midgut bile duct cystic duct common bile duct stomach embryology septum transversum mesoderm endoderm 5th week stomach rotated to left duodenum growth
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CBD and Ampulla on the Medial Duodenum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CBD and Ampulla on the Medial Duodenum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/06/82219b12.8s.jpg
http://thecommonvein.net/media/82219b14.8s.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hepatic Diverticulum
Continued volume growth and and interaction between endoderm and mesoderm result in the enlargement of the evolving liver, gallbladder, pancreas and stomach and duodenum.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219b08.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
Continued volume growth and and interaction between endoderm and mesoderm result in the enlargement of the evolving liver, gallbladder, pancreas and stomach and duodenum.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219b08.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Continued volume growth and and interaction between endoderm and mesoderm result in the enlargement of the evolving liver, gallbladder, pancreas and stomach and duodenum.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219b08.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Continued volume growth and and interaction between endoderm and mesoderm result in the enlargement of the evolving liver, gallbladder, pancreas and stomach and duodenum.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219b08.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hepatic Diverticulum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hepatic Diverticulum
Aftter the 4th week of gestation, the primitive endoderm continues to differentiate and grow. The hepatic diverticulum is the precursor for the liver bile ducts and gallbladder. At the same time mesodermal tissue from the septum transversum (purple) is available in the right upper quadrant, and the hepatic diverticulum grows into the mesederm. The pars cystica (green) will become the gallbladder and the the ventral portion of the pancreas (dark pink) is part of the endodermal outgrowth. On the medial side of the foregut the dorsal portion of the pancreas (light pink) evolves.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a02b1.8s 82219a02b3.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
Aftter the 4th week of gestation, the primitive endoderm continues to differentiate and grow. The hepatic diverticulum is the precursor for the liver bile ducts and gallbladder. At the same time mesodermal tissue from the septum transversum (purple) is available in the right upper quadrant, and the hepatic diverticulum grows into the mesederm. The pars cystica (green) will become the gallbladder and the the ventral portion of the pancreas (dark pink) is part of the endodermal outgrowth. On the medial side of the foregut the dorsal portion of the pancreas (light pink) evolves.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a02b1.8s 82219a02b3.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Aftter the 4th week of gestation, the primitive endoderm continues to differentiate and grow. The hepatic diverticulum is the precursor for the liver bile ducts and gallbladder. At the same time mesodermal tissue from the septum transversum (purple) is available in the right upper quadrant, and the hepatic diverticulum grows into the mesederm. The pars cystica (green) will become the gallbladder and the the ventral portion of the pancreas (dark pink) is part of the endodermal outgrowth. On the medial side of the foregut the dorsal portion of the pancreas (light pink) evolves.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a02b1.8s 82219a02b3.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Aftter the 4th week of gestation, the primitive endoderm continues to differentiate and grow. The hepatic diverticulum is the precursor for the liver bile ducts and gallbladder. At the same time mesodermal tissue from the septum transversum (purple) is available in the right upper quadrant, and the hepatic diverticulum grows into the mesederm. The pars cystica (green) will become the gallbladder and the the ventral portion of the pancreas (dark pink) is part of the endodermal outgrowth. On the medial side of the foregut the dorsal portion of the pancreas (light pink) evolves.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a02b1.8s 82219a02b3.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hepatic Diverticulum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hepatic Diverticulum
In the 4th week of gestation, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diveticulum at the junction of the of the foregut and midgut.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a01b2.8s 82219a02a1.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
In the 4th week of gestation, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diveticulum at the junction of the of the foregut and midgut.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a01b2.8s 82219a02a1.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
In the 4th week of gestation, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diveticulum at the junction of the of the foregut and midgut.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a01b2.8s 82219a02a1.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
In the 4th week of gestation, the primitive endoderm gives rise to a foregut diverticulum called the hepatic diveticulum at the junction of the of the foregut and midgut.
liver bile ducts pars cystica gallbladder and cystic duct. endodermal bud solid cord growth and resorbtion gallbladder embryology normal Davidoff art copyright 2008
82219a01b2.8s 82219a02a1.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hepatic Diverticulum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hepatic Diverticulum
)
