Introduction
The principles of disease in the gallbladder are the principles that govern disease elsewhere in the body but the diseases manifest with a distinctness and uniqueness in the gallbladder because of its unique structure and function.
The universal equation that defines the interactions between objects with positive or negative outcome follows;
Things interact with other things in a given environment at a moment in time resulting in a change. This change may be either good or bad – positive or negative.
When the change is bad – disorder results and the biological equivalent of disorder is disease.
There are about 12 basic disorders of disease that affect the body and the categories defined apply to the gallbladder as well. Certain categories of disease affect the gallbladder more than others because of the specific interactions, that the gallbladder is subject to.
The information below is provided to give you a broad view of the diseases that affect the gallbladder.

Red Hot Gallbladder
|
|
The red, hot, and distended gallbladder is the most common manifestation of gallbladder disease. It is most commonly caused by stones impacted in the neck or cystic duct but is also caused by prolonged cholestasis which is complicated by acalculous cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008 |
1 Inflammation
Common examples include acute cholecystis, acalculous cholecytitis, and chronic cholecytitis.
2 Infection
Common examples include HIV cholangiopathies eg cryptosporidium
3 Neoplasm amd other growth abnormalities
Benign polyps and gallbladder cancer are well lknown but relatively uncommon.
4 Mechanical
Obstruction of the gallbladder by stones in the neck, cystic duct and bile duct are common disorders. Pancreatic carcinoma is also a common cause of bile duct and gallbladder obstruction
5 Trauma
Trauma to the gallbladder is uncommon due to its protected position.
6 Metabolic
Cholelithiasis is sometimes a manifestation of metabolic disorder.
7 Circulatory
Circulatory disease is uncommon, though the end result of acute a svere distension and inflammation may be caused by ischemic necrosis of the wall.
8 Immune
Immune disease of the gallbladder is uncommon
9 Iatrogenic
Iatrogenic disease is uncommon, but bile duct injury during laparoscopic surgery does occur, and capacious cystic duct remnants withstone impaction are known but rare entities.
10 Inherited
Inherited disease of the gall bladder is rare
11 Idiopathic
Idiopathic disease is rare
12 Functional
Cholestasis due to inactivity and prolonged fasting is very common in the ICU setting. The hyperplastic disorders include adenomyomatosis and cholesterolosis are thought to be of functional origin and are fairly common
Introduction
The categories of disease have been introduced in the section on “Disease”. “Principles” serves to advance the categories in a general way before we delve into the specific diseases of the gallbladder.
Inflammation
Inflammation is the body’s response to an injurious or noxious agent. The causative noxious agent may be one of many aggressive factors in the environment including, infectious, chemical, electrical, ionizing radiation, thermal, traumatic, or a foreign body such as a splinter. The result is a relatively non specific response by the body with the process called inflammation.
Structurally the changes reflect two initial pathophysiological events; a vascular response and a cellular response. The vascular response results in an increase in blood flow to the region resulting in both an increase in fluid and an increase in leukocytes to the interstitial space at the site of injury. This causes warmth, redness, heat, and swelling.
The increased fluid in the region dilutes the noxious agent and the infiltration of leukocystes serves as a direct atttempt at destroying the invasive agent.
The damage caused by both the invasive agent and to variable extent the inflammatory response requires repair which is also instituted by the inflammatory response. Initially this consists of fibrin deposition with subsequent evolution of a longer lasting fibrotic change.
The changes of acute inflammation described by Celsus almost 2000 years ago still apply today. These include swelling, (tumor), redness (rubor), pain (dolor), and heat (calor).
The affected structure has diminished functional capacity. Virchow in 1870, added the functional incapacity of inflammed structures to Celsus’s principles .
The diagnosis of inflammation is often made clinically by utilizing the principles of Celsus and Virchow, with the patient presenting with fever, malaise, swelling and pain with relevant loss of functional capacity. Elevated white cell count and sedimentation rate are routinely found in inflammatory conditions, and imaging reflects swelling hyperemia, increased metabolic activity, and exudations.
Treatment depends on the cause but a variety of anti-inflammatory drugs are available to suppress the inflammatory response.
The inflammatory diseases of the gallbladder include acute cholecystitis, acalculous cholecytitis, and the chronic form is called chronic cholecystitis.
 Acute Cholecystitis Acute Cholecystitis |
| In this artistic rendition, a small stone has become impacted in the neck of the gallbladder, resulting in obstruction . The prolonged stasis has resulted in inflammation and infection with exudation – acute cholecystitis. The red color of the wall infers an inflammatory response.
04766b08.8s gallbladder stones cholelithiasis acute cholecystitis distended enlarged bile ducts Davidoff art copyright 2008 |
Infection
An infection is the unfavorable acute, subacute or chronic invasion (space occupation) and growth of a foreign organism in a host. The pathogenic and causative organisms include, viruses bacteria, fungi and parasities. As the invading organism grows and colonizes they utilize space and resources of the host as well as inducing an inflammatory response
The result is therefore very similar to the inflammatory changes described above.
Structurally the changes reflect two initial pathophysiological events; a vascular response and a cellular response. The vascular response results in an increase in blood flow to the region resulting in both an increase in fluid and an increase in leukocytes to the interstitial space at the site of injury. This causes warmth redness heat and swelling
The increased fluid in the region dilutes the noxious agent and the infiltration of leukocystes serves as a direct atttempt at destroying the invasive agent.
The damage caused by both the invasive agent and to variable extent the inflammatory response requires repair which is also instituted by the inflammatory response. Initially this consists of fibrin deposition with subsequent evolution of a longer lasting fibrotic change.
The debris that results from the interaction of the host with the organism may liquify to form pus and an abscess, characteristic of a bacterial infection.
Functionally the affected structure has diminished functional capacity.
The diagnosis is often made clinically by utilizing the principles of Celsus and Virchow, with the patient presenting with fever, malaise, swelling and pain with relevant loss of functional capacity. Elevated white cell count and sedimentation rate are routinely found in inflammatory conditions, and imaging reflects swelling, hyperemia, increased metabolic activity, and exudation. The presence of small amounts of air within a an extraluminal fluid collection is highly specific for infection. If the organism is isolated and cultured. sensitivity to appropriate therapy can be instituted.
Treatment depends on the cause, but a variety of anti-inflammatory drugs are available to suppress the inflammatory response, while antibacterial and antifungal agents are more specific. Antiviral agents are not routinely available. Abscesses need to be drained. Immunization against certain invading agents is available and infections such as smallpox which has been eradicated, and polio which has almost been eradictated.
HIV cholangiopathy and cryptosporidium infections of the biliary system in the HIV population are relatively common. Empyema and emphysematous cholecystitis are well known entities but are relatively uncommon.
 Emphysematous Cholecystitis and Pancreatitis Emphysematous Cholecystitis and Pancreatitis |
| The CT scan through the gallbladder is from a 61 year old female who presented with abdominal pain, acute inferior myocardial infarction, and with a background history of type II diabetes. The presence of of air in the lumen (air fluid level) and the curvilinear air in the posterior wall of the gallbladder is consistent with the diagnosis of emphysematous cholecystits – caused by gas producing gram negative organisms. This patients course was complicated by acute pancreatitis. The pancreas is edematous and illdefined midline structure anterior to the aorta and left kidney.
31093 Courtesy Ashley Davidoff MD code pancreas fx induration dx acute pancreatitis code gall bladder wall fx air dx emphysematous cholecystitis size |
Growth Abnormalities
Growth abnormalities infer a group of diseases where the growth of tissue does not conform to the expected normal pattern and where size, shape, position and character of the cells or organ become aberrant. The causes and manifestations are multiple and diverse including congenital growth abnormalities (aplasia, dysplasia, hypoplasia) acquired abnormaliites such as atrophy, hypertrophy and hyperplasia. Neoplasia and particulalrly malignant neoplasia present as one of the most challenging diseases to the medical community and to the community at large. The benign form of neoplasia infers a benign slow course with little if any loss of functional capacity. Malignant neoplasia implies a more virulent pattern with space occupation, potential for the disease to spread to other parts of the body with resulting significant functional impairment, commonly culminating in death.
The structural changes are pathologically distinct under the micrscope, but in general result in a change in size shape position or character of the tissues.
The functional changes depend on the organ involved, and the type of growth abnormality. Atresia of the mitral valve for example is life threatening, while atresia of the kidney has no ill effect. Benign neoplasm of the lung has no ill effect while a malignant neoplasm is life threatening.
The diagnosis of the growth disorders are accomplished through a combination of clinical, imaging and most importantly pathological examination.
Treatment depends on the type of disease but often requires surgery
Congenital Growth Abnormality
A congenital disorder is a disease or disorder that is present at birth. it can be caused by many factors including genetic or chromosomal aberrations, or errors in morphogenesis.
Structural results include, aplasia, hypoplasia, dysplasia, hyperplasia, agenesis, dysgenesis, teratogenesis, arteriovenous malformations, and situs abnormalities.
Functional resultsdepends on the extent and severity of the defect and ranges from minimal or no impairment to incompatibility with life.
Diagnosis is sometimes through a combination of clinical presentation, chromosomal assessment, serum testing, and medical imaging.
Treatment is based on the defect and may be medical or surgical.
The gallbladder is subject to a number of congenital defects. The most important and clinically most relevant is biliary atresia where a spectrum of hypoplastic changes occur predominantly in the biliary tree but which can affect the gallbladder to some extent. Agenesis, duplication, situs inversus and situs ambiguus are other known anomalies. variations in the shape, cystic duct length and cystic duct insertions are all normal anatomical variants.
Duplicated Gallbladder
|
|
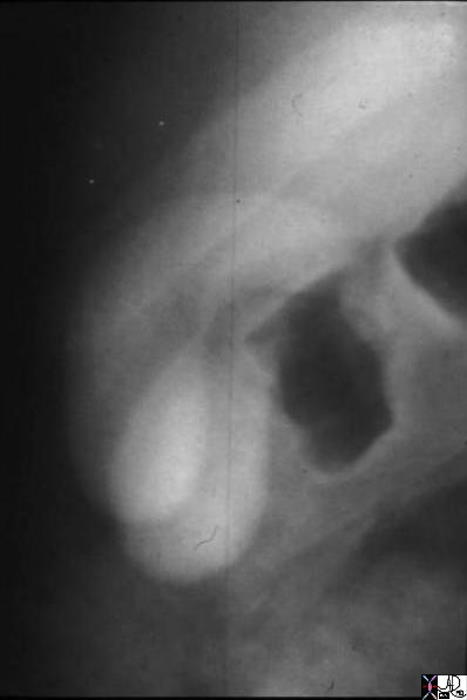
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD |
Neoplasm
British oncologist Willis has come closest with his definition of neoplasm by describing the entitiy as “… an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change.”
Benign neoplasm
Benign neoplasm is a “new growth” that consists of non aggressive, slow growth of parenchymal matrix or stromal components of a tissue, usually of unknown cause and resulting in space occupation without metastasis. benign tumors do not usually recur after removal, are usually non functioning, and do not usually cause functional impairment.
In the gallbladder benign polyps do occur, are most commonly of a non neoplastic nature eg cholesterol polyps or inflammatory polyps consisting of granulation tissue. Adenomatous polyps are rare.

Gallbladder Polyp surrounded by fluid – 3mms
|
|
The 3 mms non shadowing nodule seen on the right and anterior porion of the body of the gallbladder is defineed as a polyp rather than a stone because it is attached to the wall. The patient is in the supine position and so mobile stones should fall to the bottom of the gallbladder. In this instance it is adherent to, or attached to the wall and hence a polyp is likely.
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD |
Malignant Neoplasm
Malignant neoplasm is a “new growth” that consists of aggressive, relatively rapid and uncontrolled growth of parenchymal cells or stromal components of a tissue, usually of unknown cause and resulting in space occupation metastasis, and a tendency to recur after removal.
Structually malignant tissue is a biological unit unto itself and has size shape position and a specific character. It grows in size over time, occupies space as a squatter, has no regard for structural borders, and has no consideration for the biological unit at large.
Depending on their nature and location they will eventually limit the function of the host organ. They can be functional, but rarely are.
Diagnosis is most commonly made by direct pathological examination, while serum tumor markers and PET scanning have brought new facets to the diagnosis and staging of malignant tumors.
Treatment options include surgery, chemotherapy, radiation therapy. More recently cryotherapy, radiofrequency ablation, and chemoembolization therapy have broadened treatment options.
Growth of a Malignancy in a Tubular Organ
|
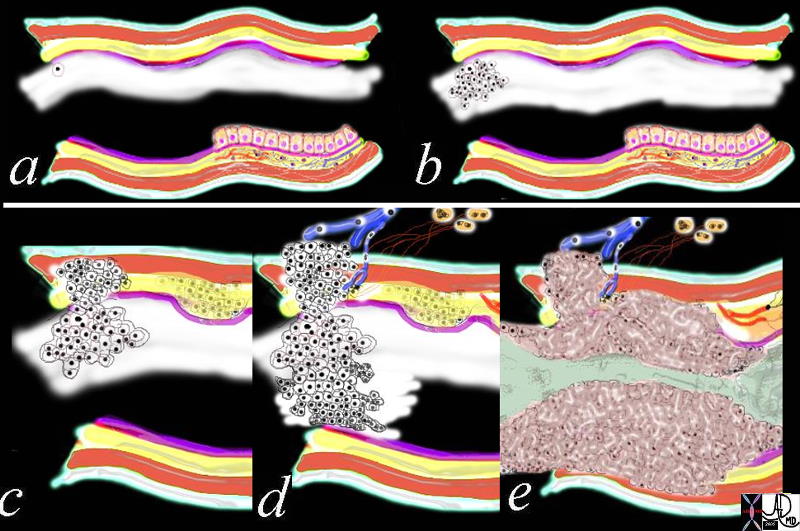
| The diagram above represents a carcinoma starting as one rebellious cell seen in (a) as a white cell with a black nucleus breaks away from the normal mucosa. It multiplies over time and eventually forms a clump of cells which go onto to form a nodule (b) As the nodule grows it invades the layers of the wall and once it breaks through the muscularis layer (red) a new and concerning era for the tumor is reached. As it continues to grow it will invade the outer layer of the wall, the regional nodes and also the blood vessels. Once it reaches this stage then it can spread systemically. (d) Locally, the tumor grows and takes up space in the lumen of the host structure eventually obstructing flow and limiting function.(e)
32354c01.800 tube colon trachea bronchus small bowel bile duct epithelium neoplasm benign malignant malignancy epithelial cell multiply multiplication growth mucosa submucosa muscularis serosa adventitia vein lymph node circumferential metastasixe metastasis metastases narrowing stenosis obstruction complication cancer uncontrolled growth Davidoff drawing Davidoff art Davidoff tube Davidoff MD |
Gallbladder cancer is a particularly difficult therapeutic challenge because presentation is late and direct spread to the liver is early through the lymphatics and veins in the gallbladder fossa.
Direct Invasion into the Liver and Bile Duct Obstruction
|
|
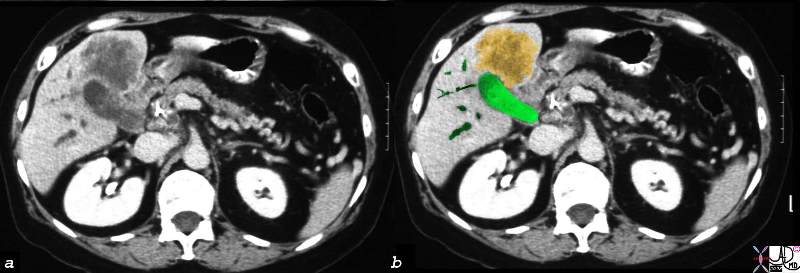
Gallbladder cancer spreads early into the liver through the gallbladder fosssa. In this CTscan through the gallbladder (green) the cancer (orange) has spread into the liver and has caused bile duct obstruction (dark green tubular structures in b)
16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008
|
Mechanical Disorders – Obstruction
A mechanical disorder is defined as a disease where a finite structural change causes disease. Entities such as obstructions, torsions, herniations, ruptures are examples of mechanical disease.
In tubular systems that have pliable walls such as in the gastrointestinal tract the structural changes of obstruction will be upstream dilatation and downstream decompression.
Functionally mechanical disorders commonly result in failed delivery of a product.
Complications of structural disease may have circulatory consequences. Thus a torsion or a herniation may cause infarction
Clinical presentations of mechanical disrders are usually acute and dramatic. Acute obstruction of the gastrointestinal tract, biliary tract, or genitourinary tract results in significant pain.
Diagnosis is made via a combination of clinical examination and imaging. Obstruction of the gastrointestinal tract results in abdominal distension and vomitting and would be clinically apparent, whereas ureteric pain from stone disease is not as distinctly clinically manifest and is best diagnosed by imaging techniques.
Treatment often requires surgery or a mechanical intervention and removal or repair of the structural deformity.
Acute cholecytitis is primarily a mechanical disease because it is caused by a stone in the cystic duct or neck of the gallbladder. With prolonged obstruction, secondary inflammation occurs and the mechanical disorder transforms and is complicated by an inflamatory disorder.

Choledocholithiasis
|
|
The MRCP performed using T2 weighted FSE technique shows a CBD stone (orange) associated with dilatation of the CBD, cystic duct and the gallbladder.
17083c02.3k.8s 82 female presents with obstructive jaundice gallbladder duct enlarged distended distension dilated dilatation choledocholithiasis stone obstruction obstructive jaundice MRI T2 weighted Courtesy Ashley Davidoff MD copyright 2008 |
Trauma
Traumatic injury is a form of mechanical injury where the inciting aggressive force is from the external environment. The cause is either via blunt or penetrating mechanism and it results in tearing, shearing, or fracture of the tissues.
Structurally the injuries range from mild swelling or bruising to extensive tearing and even rupture of the organs.
Functionally impairment varies from minimal to mortal consequences.
The diagnosis is based mostly on the history, and the extent of injury is evaluated from a clinical and imaging standpoint.
Treatment depends on the extent and location of injury but surgery is the most common form, with medical treatment used for supportive measures.
Trauma to the gallbladder is relatively uncommon because of the position of the gallbladder and its protection by the liver.

Gallbladder Laceration from Trauma
|
| The 32 year old male suffered from a motor vehicle accident and presented with right upper quadrant pain. The gallbladder shows disruption of the mucosal enhancement (arrow in a) and is thick walled (pink) These findings are consistent with a a laceratio and possible rupture of the gallbladder.
16216c01.8s 32 male s/p trauma MVA gallbladder hyperemic mucosa thickened wall disrupted mucosa decompresssed lumen CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Metabolic Disease
Metabolic disease is the aberration of the biochemical mileu of the body caused by aberrant absorbtion, aberrant control mechanisms such as endocrinolgical disease, or aberrant excretion of chemicals or water from the organs or the body.
Structurally the biochemical changes more commonly than not do not have structural change at a macroscopic level, but endocrinological diseases such as Grave’s disease, gigantism, and Cushing’s disease do have characteristic and distinct structural manifestations.
Functionally the effects are far reaching and variable depending on which of the many complex chemicals is involved.
The diagnosis is made usually by evaluation of the body fluids.
Treatment is based on the cause of disease.
The gallbladder sometimes is the harbinger of gallstones caused by abnormal cholesterol metabolism or by excessive aberrant metabolism that causes pigmented stones.

Low Density Cholesterol stone
|
| The CTscan through the gallbladder shows a relatively large (approximately 1cms) low density stone with minimal rim calcificationlying dependantly in the body of the gallbladder. This finding is reminiscent of a cholesterol stone.
25566.8s gallbladder stone low density filling defect cholelithiasis cholesterol Cpourtesy Ashley DAvidoff MD copyright 2008 |
Circulatory Disease
Circulatory disease is an aberrance of any part of the structures of the circulation but usually inferring disease of the arteries or veins. Causes for diseasese include thrombosis, embolisation, aneurysmal disease, arteriovenous malformation, congestion, ischemia, or infarction.
The structural changes are manifest in the vessel involved and sometimes at the end organ level as well.
The functional changes vary between minimal effects such as in varicocties, to life threatening situations such as in coronary thrombosis, or ruptured aneurysm.
Diagnosis is a combination of clinical evaluation and imaging manifestations. Angiography used to be the mainstay of diagnosis of circulatory disease, but CTscans and MRI are evolving as major tools since they are able to evaluate both the vessels and the end organ to better effect.
Treatment is based on the disease, but newer techniques in the minimally invasive sphere have become imporant including thrombolyis, vessel stenting and angioplasty.
The gallbladder has an endarterial blood supply so that the fundus is the most vulnerable part. When the gallbladder becomes distended, pressure on the vessel wall can result in ischemic necrosis with rupture of the wall usually at the fundus.
Scleroderma Pulmonary Hypertension and Right Heart Failure
|
|
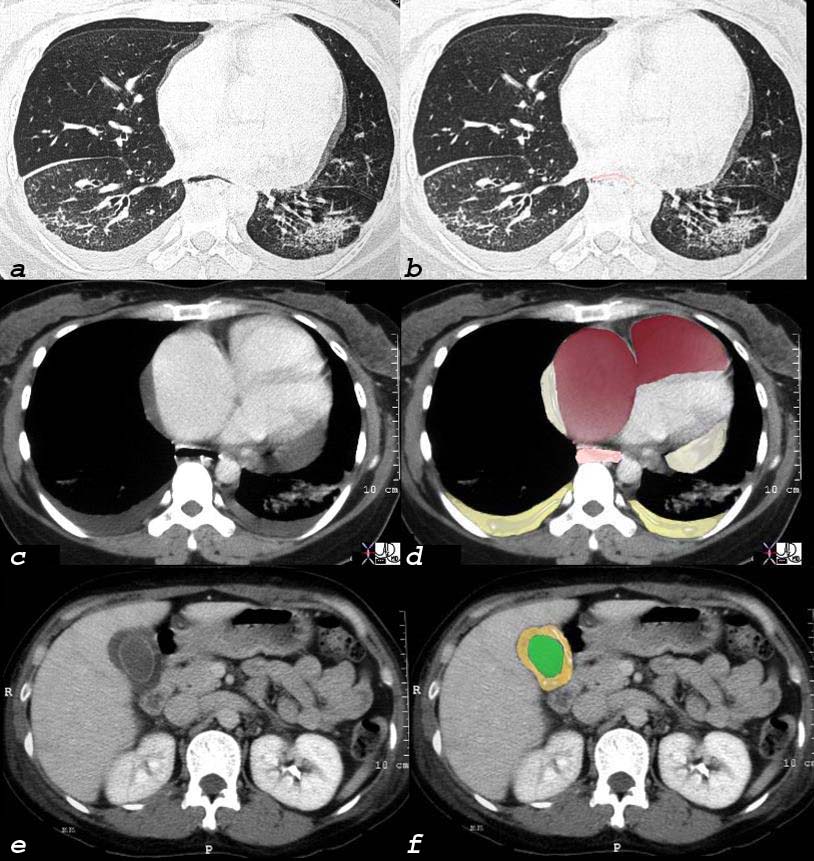
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema. This is a issue of congestion of the hepatic venous syustem causing congestion of the gallbladder drainage and subsequent result of gallbladder wall edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD |
Iatrogenic disease
Iatrogenic disease is disorder induced by physicians and includes causes such as negative effects of drugs, errors in surgery, hospital acquired infections, and medication errors.
The resulting disorders are varied and the structural, functional results and diagnostic and therapeutic challenges are equally varied.
Laparoscopic surgery on the gallbladdder by inexperienced surgeons may result in bile duct injury which complicates recovery and requires further surgery to repair the ducts.
Immune disease
Immune disease incorporates aberrant allergic immune response to noxious agents in the environment including microorganisms, pollen or dust, as well as the autoimmune diseases where the aberrant immune system fails to recognize host tissue.
The cause for these responses is in general not known, and the structural result ranges from muscle spasm, to anaphylaxis, to acute and chronic inflammation.
Functionally the range of disorders includes bronchospasm, edema, hypotension in the anaphylaxis/allergic group, to chronic debilitaion and multisystem dysfunction in the autoimmune group.
Treatment is medical and is in general antiinflammatory in nature.
The gallbladder is not usually involved in immune disease.
Idiopathic Disease
Idiopathic disease is a disease of unknown cause
Functional Disorders
Functional disorders are diseases that arise from aberrant function that does not have an obvious structural basis.
The hyperplastic cholecystoses are a range of diseases that appear to have a functional basis possibly related to hypercontractile disorders of the gallbladder.

Strawberry Gallbladder
|
|
The dramatic pathology image shows an opened gallbladder stippled with yellow fatty deposits of cholesterol, in a background of a hyperemic red mucosa, that is characteristic of the strawberry gallbladder. Strawberry gallbladder is on of the entities that belong in the group of diseases of the gallbladder called the hyperplastic cholecystoses which appear to be related to a hypercontractile state.
hyperemic 04777.800 gallbladder strawberry gallbladder hyperemic mucosa yellow cholesterolosis hyperplastic cholecystoses cholecytosis Davidoff MD hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis cholesterolosis |
References
Diseases of the Gallbladder
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Strawberry Gallbladder
The dramatic pathology image shows an opened gallbladder stippled with yellow fatty deposits of cholesterol, in a background of a hyperemic red mucosa, that is characteristic of the strawberry gallbladder. Strawberry gallbladder is on of the entities that belong in the group of diseases of the gallbladder called the hyperplastic cholecystoses which appear to be related to a hypercontractile state.
hyperemic 04777.800 gallbladder strawberry gallbladder hyperemic mucosa yellow cholesterolosis hyperplastic cholecystoses cholecytosis Davidoff MD hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis cholesterolosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Strawberry Gallbladder
The dramatic pathology image shows an opened gallbladder stippled with yellow fatty deposits of cholesterol, in a background of a hyperemic red mucosa, that is characteristic of the strawberry gallbladder. Strawberry gallbladder is on of the entities that belong in the group of diseases of the gallbladder called the hyperplastic cholecystoses which appear to be related to a hypercontractile state.
hyperemic 04777.800 gallbladder strawberry gallbladder hyperemic mucosa yellow cholesterolosis hyperplastic cholecystoses cholecytosis Davidoff MD hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis cholesterolosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The dramatic pathology image shows an opened gallbladder stippled with yellow fatty deposits of cholesterol, in a background of a hyperemic red mucosa, that is characteristic of the strawberry gallbladder. Strawberry gallbladder is on of the entities that belong in the group of diseases of the gallbladder called the hyperplastic cholecystoses which appear to be related to a hypercontractile state.
hyperemic 04777.800 gallbladder strawberry gallbladder hyperemic mucosa yellow cholesterolosis hyperplastic cholecystoses cholecytosis Davidoff MD hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis cholesterolosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The dramatic pathology image shows an opened gallbladder stippled with yellow fatty deposits of cholesterol, in a background of a hyperemic red mucosa, that is characteristic of the strawberry gallbladder. Strawberry gallbladder is on of the entities that belong in the group of diseases of the gallbladder called the hyperplastic cholecystoses which appear to be related to a hypercontractile state.
hyperemic 04777.800 gallbladder strawberry gallbladder hyperemic mucosa yellow cholesterolosis hyperplastic cholecystoses cholecytosis Davidoff MD hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis cholesterolosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Strawberry Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Strawberry Gallbladder
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema. This is a issue of congestion of the hepatic venous syustem causing congestion of the gallbladder drainage and subsequent result of gallbladder wall edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema. This is a issue of congestion of the hepatic venous syustem causing congestion of the gallbladder drainage and subsequent result of gallbladder wall edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema. This is a issue of congestion of the hepatic venous syustem causing congestion of the gallbladder drainage and subsequent result of gallbladder wall edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 32 year old female has scleroderma and her disease is characterized by interstitial basal lung disease (a,b) with normal anterior lung fields and fibrotic posterior lung fields, enlargement of right heart structures (maroon in d), pericardial effusion (light yellow in d), pleural effusions (dark yellow in d) and an edematous wall (orange, in f) of the gallbladder (lumen is green). As a result of her lung disease she developed pulmonary hypertension, right heart failure and tricuspid regurgitation and this lead to the gallbladder edema. This is a issue of congestion of the hepatic venous syustem causing congestion of the gallbladder drainage and subsequent result of gallbladder wall edema.
and 30464c08 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium gallbladder esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure pulmonary hypertension cor pulmonale dx scleroderma CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Scleroderma Pulmonary Hypertension and Right Heart Failure
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Low Density Cholesterol stone
The CTscan through the gallbladder shows a relatively large (approximately 1cms) low density stone with minimal rim calcificationlying dependantly in the body of the gallbladder. This finding is reminiscent of a cholesterol stone.
25566.8s gallbladder stone low density filling defect cholelithiasis cholesterol Cpourtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Low Density Cholesterol stone
The CTscan through the gallbladder shows a relatively large (approximately 1cms) low density stone with minimal rim calcificationlying dependantly in the body of the gallbladder. This finding is reminiscent of a cholesterol stone.
25566.8s gallbladder stone low density filling defect cholelithiasis cholesterol Cpourtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CTscan through the gallbladder shows a relatively large (approximately 1cms) low density stone with minimal rim calcificationlying dependantly in the body of the gallbladder. This finding is reminiscent of a cholesterol stone.
25566.8s gallbladder stone low density filling defect cholelithiasis cholesterol Cpourtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CTscan through the gallbladder shows a relatively large (approximately 1cms) low density stone with minimal rim calcificationlying dependantly in the body of the gallbladder. This finding is reminiscent of a cholesterol stone.
25566.8s gallbladder stone low density filling defect cholelithiasis cholesterol Cpourtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Low Density Cholesterol stone
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Low Density Cholesterol stone
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Gallbladder Laceration from Trauma
The 32 year old male suffered from a motor vehicle accident and presented with right upper quadrant pain. The gallbladder shows disruption of the mucosal enhancement (arrow in a) and is thick walled (pink) These findings are consistent with a a laceratio and possible rupture of the gallbladder.
16216c01.8s 32 male s/p trauma MVA gallbladder hyperemic mucosa thickened wall disrupted mucosa decompresssed lumen CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Gallbladder Laceration from Trauma
The 32 year old male suffered from a motor vehicle accident and presented with right upper quadrant pain. The gallbladder shows disruption of the mucosal enhancement (arrow in a) and is thick walled (pink) These findings are consistent with a a laceratio and possible rupture of the gallbladder.
16216c01.8s 32 male s/p trauma MVA gallbladder hyperemic mucosa thickened wall disrupted mucosa decompresssed lumen CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The 32 year old male suffered from a motor vehicle accident and presented with right upper quadrant pain. The gallbladder shows disruption of the mucosal enhancement (arrow in a) and is thick walled (pink) These findings are consistent with a a laceratio and possible rupture of the gallbladder.
16216c01.8s 32 male s/p trauma MVA gallbladder hyperemic mucosa thickened wall disrupted mucosa decompresssed lumen CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The 32 year old male suffered from a motor vehicle accident and presented with right upper quadrant pain. The gallbladder shows disruption of the mucosal enhancement (arrow in a) and is thick walled (pink) These findings are consistent with a a laceratio and possible rupture of the gallbladder.
16216c01.8s 32 male s/p trauma MVA gallbladder hyperemic mucosa thickened wall disrupted mucosa decompresssed lumen CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Gallbladder Laceration from Trauma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Gallbladder Laceration from Trauma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Choledocholithiasis
The MRCP performed using T2 weighted FSE technique shows a CBD stone (orange) associated with dilatation of the CBD, cystic duct and the gallbladder.
17083c02.3k.8s 82 female presents with obstructive jaundice gallbladder duct enlarged distended distension dilated dilatation choledocholithiasis stone obstruction obstructive jaundice MRI T2 weighted Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Choledocholithiasis
The MRCP performed using T2 weighted FSE technique shows a CBD stone (orange) associated with dilatation of the CBD, cystic duct and the gallbladder.
17083c02.3k.8s 82 female presents with obstructive jaundice gallbladder duct enlarged distended distension dilated dilatation choledocholithiasis stone obstruction obstructive jaundice MRI T2 weighted Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The MRCP performed using T2 weighted FSE technique shows a CBD stone (orange) associated with dilatation of the CBD, cystic duct and the gallbladder.
17083c02.3k.8s 82 female presents with obstructive jaundice gallbladder duct enlarged distended distension dilated dilatation choledocholithiasis stone obstruction obstructive jaundice MRI T2 weighted Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The MRCP performed using T2 weighted FSE technique shows a CBD stone (orange) associated with dilatation of the CBD, cystic duct and the gallbladder.
17083c02.3k.8s 82 female presents with obstructive jaundice gallbladder duct enlarged distended distension dilated dilatation choledocholithiasis stone obstruction obstructive jaundice MRI T2 weighted Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Choledocholithiasis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Choledocholithiasis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Direct Invasion into the Liver and Bile Duct Obstruction
Gallbladder cancer spreads early into the liver through the gallbladder fosssa. In this CTscan through the gallbladder (green) the cancer (orange) has spread into the liver and has caused bile duct obstruction (dark green tubular structures in b)
16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Direct Invasion into the Liver and Bile Duct Obstruction
Gallbladder cancer spreads early into the liver through the gallbladder fosssa. In this CTscan through the gallbladder (green) the cancer (orange) has spread into the liver and has caused bile duct obstruction (dark green tubular structures in b)
16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Gallbladder cancer spreads early into the liver through the gallbladder fosssa. In this CTscan through the gallbladder (green) the cancer (orange) has spread into the liver and has caused bile duct obstruction (dark green tubular structures in b)
16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Gallbladder cancer spreads early into the liver through the gallbladder fosssa. In this CTscan through the gallbladder (green) the cancer (orange) has spread into the liver and has caused bile duct obstruction (dark green tubular structures in b)
16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Direct Invasion into the Liver and Bile Duct Obstruction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Direct Invasion into the Liver and Bile Duct Obstruction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Growth of a Malignancy in a Tubular Organ
The diagram above represents a carcinoma starting as one rebellious cell seen in (a) as a white cell with a black nucleus breaks away from the normal mucosa. It multiplies over time and eventually forms a clump of cells which go onto to form a nodule (b) As the nodule grows it invades the layers of the wall and once it breaks through the muscularis layer (red) a new and concerning era for the tumor is reached. As it continues to grow it will invade the outer layer of the wall, the regional nodes and also the blood vessels. Once it reaches this stage then it can spread systemically. (d) Locally, the tumor grows and takes up space in the lumen of the host structure eventually obstructing flow and limiting function.(e)
32354c01.800 tube colon trachea bronchus small bowel bile duct epithelium neoplasm benign malignant malignancy epithelial cell multiply multiplication growth mucosa submucosa muscularis serosa adventitia vein lymph node circumferential metastasixe metastasis metastases narrowing stenosis obstruction complication cancer uncontrolled growth Davidoff drawing Davidoff art Davidoff tube Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Growth of a Malignancy in a Tubular Organ
The diagram above represents a carcinoma starting as one rebellious cell seen in (a) as a white cell with a black nucleus breaks away from the normal mucosa. It multiplies over time and eventually forms a clump of cells which go onto to form a nodule (b) As the nodule grows it invades the layers of the wall and once it breaks through the muscularis layer (red) a new and concerning era for the tumor is reached. As it continues to grow it will invade the outer layer of the wall, the regional nodes and also the blood vessels. Once it reaches this stage then it can spread systemically. (d) Locally, the tumor grows and takes up space in the lumen of the host structure eventually obstructing flow and limiting function.(e)
32354c01.800 tube colon trachea bronchus small bowel bile duct epithelium neoplasm benign malignant malignancy epithelial cell multiply multiplication growth mucosa submucosa muscularis serosa adventitia vein lymph node circumferential metastasixe metastasis metastases narrowing stenosis obstruction complication cancer uncontrolled growth Davidoff drawing Davidoff art Davidoff tube Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The diagram above represents a carcinoma starting as one rebellious cell seen in (a) as a white cell with a black nucleus breaks away from the normal mucosa. It multiplies over time and eventually forms a clump of cells which go onto to form a nodule (b) As the nodule grows it invades the layers of the wall and once it breaks through the muscularis layer (red) a new and concerning era for the tumor is reached. As it continues to grow it will invade the outer layer of the wall, the regional nodes and also the blood vessels. Once it reaches this stage then it can spread systemically. (d) Locally, the tumor grows and takes up space in the lumen of the host structure eventually obstructing flow and limiting function.(e)
32354c01.800 tube colon trachea bronchus small bowel bile duct epithelium neoplasm benign malignant malignancy epithelial cell multiply multiplication growth mucosa submucosa muscularis serosa adventitia vein lymph node circumferential metastasixe metastasis metastases narrowing stenosis obstruction complication cancer uncontrolled growth Davidoff drawing Davidoff art Davidoff tube Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The diagram above represents a carcinoma starting as one rebellious cell seen in (a) as a white cell with a black nucleus breaks away from the normal mucosa. It multiplies over time and eventually forms a clump of cells which go onto to form a nodule (b) As the nodule grows it invades the layers of the wall and once it breaks through the muscularis layer (red) a new and concerning era for the tumor is reached. As it continues to grow it will invade the outer layer of the wall, the regional nodes and also the blood vessels. Once it reaches this stage then it can spread systemically. (d) Locally, the tumor grows and takes up space in the lumen of the host structure eventually obstructing flow and limiting function.(e)
32354c01.800 tube colon trachea bronchus small bowel bile duct epithelium neoplasm benign malignant malignancy epithelial cell multiply multiplication growth mucosa submucosa muscularis serosa adventitia vein lymph node circumferential metastasixe metastasis metastases narrowing stenosis obstruction complication cancer uncontrolled growth Davidoff drawing Davidoff art Davidoff tube Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Growth of a Malignancy in a Tubular Organ
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Growth of a Malignancy in a Tubular Organ
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Gallbladder Polyp surrounded by fluid – 3mms
The 3 mms non shadowing nodule seen on the right and anterior porion of the body of the gallbladder is defineed as a polyp rather than a stone because it is attached to the wall. The patient is in the supine position and so mobile stones should fall to the bottom of the gallbladder. In this instance it is adherent to, or attached to the wall and hence a polyp is likely.
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Gallbladder Polyp surrounded by fluid – 3mms
The 3 mms non shadowing nodule seen on the right and anterior porion of the body of the gallbladder is defineed as a polyp rather than a stone because it is attached to the wall. The patient is in the supine position and so mobile stones should fall to the bottom of the gallbladder. In this instance it is adherent to, or attached to the wall and hence a polyp is likely.
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The 3 mms non shadowing nodule seen on the right and anterior porion of the body of the gallbladder is defineed as a polyp rather than a stone because it is attached to the wall. The patient is in the supine position and so mobile stones should fall to the bottom of the gallbladder. In this instance it is adherent to, or attached to the wall and hence a polyp is likely.
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The 3 mms non shadowing nodule seen on the right and anterior porion of the body of the gallbladder is defineed as a polyp rather than a stone because it is attached to the wall. The patient is in the supine position and so mobile stones should fall to the bottom of the gallbladder. In this instance it is adherent to, or attached to the wall and hence a polyp is likely.
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Gallbladder Polyp surrounded by fluid – 3mms
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Gallbladder Polyp surrounded by fluid – 3mms
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Duplicated Gallbladder
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The oral cholecystogram shows two gallbladders lying side by side. This duplex system consists of two fundi and two bodies. The cystic duct is not appreciated in this example, but it is commonly a single entity.
04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Duplicated Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Duplicated Gallbladder
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Emphysematous Cholecystitis and Pancreatitis
The CT scan through the gallbladder is from a 61 year old female who presented with abdominal pain, acute inferior myocardial infarction, and with a background history of type II diabetes. The presence of of air in the lumen (air fluid level) and the curvilinear air in the posterior wall of the gallbladder is consistent with the diagnosis of emphysematous cholecystits – caused by gas producing gram negative organisms. This patients course was complicated by acute pancreatitis. The pancreas is edematous and illdefined midline structure anterior to the aorta and left kidney.
31093 Courtesy Ashley Davidoff MD code pancreas fx induration dx acute pancreatitis code gall bladder wall fx air dx emphysematous cholecystitis size
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Emphysematous Cholecystitis and Pancreatitis
The CT scan through the gallbladder is from a 61 year old female who presented with abdominal pain, acute inferior myocardial infarction, and with a background history of type II diabetes. The presence of of air in the lumen (air fluid level) and the curvilinear air in the posterior wall of the gallbladder is consistent with the diagnosis of emphysematous cholecystits – caused by gas producing gram negative organisms. This patients course was complicated by acute pancreatitis. The pancreas is edematous and illdefined midline structure anterior to the aorta and left kidney.
31093 Courtesy Ashley Davidoff MD code pancreas fx induration dx acute pancreatitis code gall bladder wall fx air dx emphysematous cholecystitis size
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The CT scan through the gallbladder is from a 61 year old female who presented with abdominal pain, acute inferior myocardial infarction, and with a background history of type II diabetes. The presence of of air in the lumen (air fluid level) and the curvilinear air in the posterior wall of the gallbladder is consistent with the diagnosis of emphysematous cholecystits – caused by gas producing gram negative organisms. This patients course was complicated by acute pancreatitis. The pancreas is edematous and illdefined midline structure anterior to the aorta and left kidney.
31093 Courtesy Ashley Davidoff MD code pancreas fx induration dx acute pancreatitis code gall bladder wall fx air dx emphysematous cholecystitis size
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The CT scan through the gallbladder is from a 61 year old female who presented with abdominal pain, acute inferior myocardial infarction, and with a background history of type II diabetes. The presence of of air in the lumen (air fluid level) and the curvilinear air in the posterior wall of the gallbladder is consistent with the diagnosis of emphysematous cholecystits – caused by gas producing gram negative organisms. This patients course was complicated by acute pancreatitis. The pancreas is edematous and illdefined midline structure anterior to the aorta and left kidney.
31093 Courtesy Ashley Davidoff MD code pancreas fx induration dx acute pancreatitis code gall bladder wall fx air dx emphysematous cholecystitis size
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Emphysematous Cholecystitis and Pancreatitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Emphysematous Cholecystitis and Pancreatitis
)
https://beta.thecommonvein.net/wp-content/uploads/2023/05/31093.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Acute Cholecystitis
In this artistic rendition, a small stone has become impacted in the neck of the gallbladder, resulting in obstruction . The prolonged stasis has resulted in inflammation and infection with exudation – acute cholecystitis. The red color of the wall infers an inflammatory response.
04766b08.8s gallbladder stones cholelithiasis acute cholecystitis distended enlarged bile ducts Davidoff art copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Cholecystitis
In this artistic rendition, a small stone has become impacted in the neck of the gallbladder, resulting in obstruction . The prolonged stasis has resulted in inflammation and infection with exudation – acute cholecystitis. The red color of the wall infers an inflammatory response.
04766b08.8s gallbladder stones cholelithiasis acute cholecystitis distended enlarged bile ducts Davidoff art copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this artistic rendition, a small stone has become impacted in the neck of the gallbladder, resulting in obstruction . The prolonged stasis has resulted in inflammation and infection with exudation – acute cholecystitis. The red color of the wall infers an inflammatory response.
04766b08.8s gallbladder stones cholelithiasis acute cholecystitis distended enlarged bile ducts Davidoff art copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this artistic rendition, a small stone has become impacted in the neck of the gallbladder, resulting in obstruction . The prolonged stasis has resulted in inflammation and infection with exudation – acute cholecystitis. The red color of the wall infers an inflammatory response.
04766b08.8s gallbladder stones cholelithiasis acute cholecystitis distended enlarged bile ducts Davidoff art copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute Cholecystitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute Cholecystitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Red Hot Gallbladder
The red, hot, and distended gallbladder is the most common manifestation of gallbladder disease. It is most commonly caused by stones impacted in the neck or cystic duct but is also caused by prolonged cholestasis which is complicated by acalculous cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Red Hot Gallbladder
The red, hot, and distended gallbladder is the most common manifestation of gallbladder disease. It is most commonly caused by stones impacted in the neck or cystic duct but is also caused by prolonged cholestasis which is complicated by acalculous cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The red, hot, and distended gallbladder is the most common manifestation of gallbladder disease. It is most commonly caused by stones impacted in the neck or cystic duct but is also caused by prolonged cholestasis which is complicated by acalculous cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The red, hot, and distended gallbladder is the most common manifestation of gallbladder disease. It is most commonly caused by stones impacted in the neck or cystic duct but is also caused by prolonged cholestasis which is complicated by acalculous cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Red Hot Gallbladder
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Red Hot Gallbladder
)
