
The Common Vein Copyright 2010
definition
The femur of the musculoskeletal system is characterized by being the longest and heaviest bone in the body.
It is part of the upper leg and its femoral head articulates with the acetabulum to form the hip. The distal femur articulates with the patella and the tibia to form the knee joint. It consists of bone and cartilage tissue once mature.
Its unique structural features include a head, fovea, neck, shaft, greater trochanter, lesser trochanter, intertrochanteric line, lateral condyle, medial condyle, adductor tubercle. The femur is approximately 48 cm long and 2.3 cm in diameter. The length of the femur is approximately ¼ the height of the person. Overlying the femur are the anterior, medial, and posterior thigh muscles. The sciatic nerve runs posterior to the femur. The femoral artery and nerve run anterior to the femur. As the femoral artery becomes the popliteal artery, it changes course to run into the popliteal fossa in the posterior knee.
The femoral head sits in the acetabulum as a round structure with a small indentation called the fovea. The fovea has a ligament that connects the femoral head with the acetabulum. The ligament of head or ligamentum teres contains a small arterial branch of the obturator artery known as the acetabular branch of the obturator artery. This artery does not supply sufficient blood flow to the femoral head. The articular surface of the femoral head is covered by articular cartilage.
The femoral neck is the portion of the femur that is between the femoral head and the trochanters. The diameter of the neck is less that at the femoral head. The femoral neck meets the femoral shaft at an angle of approximately 126 degrees. There is usually a degree of anterversion in the relationship of the femoral head and shaft. Anteversion refers to the head being anterior to the midline of the femoral shaft. The femoral shaft is therefore internally rotated. The adult neck-shaft angle in the frontal/coronal plane is normally 5-15 degrees.
The greater and lesser trochanters are at the junction of where the femoral neck meets the shaft. The lesser trochanter is cone-shaped and rounded on the posteromedial portion of the neck-shaft junction. The lesser trochanter is the attachment site for the iliopsoas muscle. The greater trochanter is located at the lateral, superior, and posterior portion of the neck-shaft junction. The greater trochanter is the large attachment and leverage site for abductors and thigh rotators.
The intertrochanteric line is the anterior site of the neck-shaft junction. This bony ridge also connects the greater and lesser trochanters. The iliofemoral ligament attaches here. Part of the origin of the vastus medialis is at the intertrochanteric line.
The posterior neck-shaft junction site is known as the intertrochanteric crest. The intertrochanteric crest?s quadrate tubercle is the attachment site for the quadrates femoris muscle. The quadrate tubercle is an elevatated and rounded portion along the intertrochanteric crest.
The femoral shaft is a tubular structure. It is slightly twisted with an anterior bowing/convexity. The linea aspera is a rough line on the posterior femoral shaft that serves as an attachment for the adductor?s aponeurosis. The linea aspera has medial and lateral lips. The lateral lip merges with the gluteal tuberosity. The gluteal tuberosity is the site of attachment for the gluteus maximus muscle. The medial lip of the linea aspera becomes the spiral line. The spiral line is continuous with the intertrochanteric line. Distally the linea aspera spreads into the medial and lateral supracondylar ridges.
The femoral shaft proximally contains the pectineal line which is the attachment site for the pectineus, psoas minor, and the adductor brevis.
The distal femur widens into the medial and lateral femoral epicondyles. The epicondyles are the proximal origins for the medial and lateral collateral ligaments. The medial and lateral femoral condyles are covered with articular cartilage and intracapsular as they articulate with the menisci in the knee and the tibial condyles. The medial surface of the distal femur has an elevated portion known as the adductor tubercle that is proximal to the medial epicondyle. The adductor tubercle is an attachment site for the adductor magnus?s hamstring component tendon.
In between the medial and lateral femoral condyles is the intercondylar notch. This notch serves as the attachment side to the anterior and the posterior cruciate ligaments to provide anterior-posterior stability to the knee.
The femur ossifies at different parts throughout growth. At the 7th fetal week, the body of the femur appears. The femoral head and trochanters do not appear until 11 months. The head and trochanters appear as one large physis that fuses by age 18. The greater trochanter becomes distinct at 5 years, while the lesser trochanter becomes distinct at 9 years. There is fusion of the trochanters by age 16. Distally, the femoral physis appears at birth and fuses at 19 years of age. The femur as well as all other bones, muscles, and ligaments of the body are derived of mesodermal origin in embryo.
The inclination of the proximal femur changes throughout growth. At birth it is nearly straight, but gradually decreases to reach the adult angle of about 126 degrees in the sagittal plane. This angle is less in females due to the width of the pelvis.
The function of the femur is to allow for weight bearing and to serve as attachments for muscles and ligaments to move and stabilize the joints. The proximal head articulates with the acetabulum to form the hip joint. The distal femur articulates with the patella and tibia to make the knee joint. Bipedal walking is made possible by the anatomic relationship of the knee, femur, and acetabulum. Fractures to the femur can injury the neurovascular system. The femur contains bone marrow that is responsible for making blood products including white blood cells, red blood cells, and platelets..
Common diseases include arthritis, fracture, tumor, bursitis, osteomyelitis, Legg-Calve Perthes Disease, Slipped Capital Femoral Epiphysis (SCFE), osteochondritis dessicans, femoral anteversion/retroversion, coxa valga/vara, rickets, stress fractures, osteochondral defects, patellofemoral syndrome and chondromalacia patella.
Osteomyelitis is an infection of the bone usually due to bacteria.
Tumors can either be primary or from metastasis. A few primary tumors that can occur in the femur include leukemia, lymphoma, neuroblastoma, osteoblastoma, osteosarcoma, osteoid osteoma, enchondroma, and Ewing?s Sarcoma.
Legg-Calve-Perthes Disease (LCP) is a form of osteonecrosis/avascular necrosis that occurs at the femoral head. There is inadequate blood supply to the bone resulting in cell death. Patients between age 3 to 12 with a limp may have LCP. X-rays will show destruction and fragmentation of the femoral head early in the disease process, then healing later on. It can be a cause of chronic hip pain as the healed femoral head may not articulate well with the acetabulum.
Slipped Capital Femoral Epiphysis (SCFE) is a condition where there is displacement of the bones on each side of the growth plate in the proximal femur. Patients are typically adolescent boys that are obese. They present with hip, groin, or knee pain and a limp.
Increased femoral anteversion can result in an intoeing gait. Increased anterversion is when the neck-shaft angle is greater than 15 degrees. Femoral retroversion occurs when the neck-shaft angle is less than 5 degrees.
Coxa valga and coxa vara refer to the angle of the femoral neck and shaft in the sagittal plane. Coxa valga is an angle greater than 135 degrees, while coxa vara occurs when the angle is less than 120 degrees.
Rickets and other calcium depleting conditions can cause the femoral shaft to increase in convexity or bow.
Commonly used diagnostic procedures include clinical history, physical exam, x-ray, MRI, bone scan, and CT scan. Prenatal ultrasound often focuses on the size of the femur to determine the approximate age of the developing fetus.
It is usually treated with internal or external surgical fixation or non-operative approaches for fractures and slipped capital femoral epiphysis. Bursitis is treated with physical therapy, NSAIDs and steroid injections. Tumors can be treated with surgery, chemotherapy, and radiation. Rickets is treated with replacing vitamin D. Stress fractures are treated with rest, physical therapy, and dietary modification. Arthritis is treated initially with physical therapy, NSAIDs, steroid injections, and braces. Arthritis can also be surgically treated with arthroscopic debridement or hip and knee replacements. Osteochondral defects can be treated with microfracture surgery, allografts, or autologous cartilage transplantation.
The unique characteristics of the femur include its:
– largest bone in the body
– situated between the hip and the knee
– right and left femurs are mirror images of each other
– outer hard cortical bone
– softer inner cancellous bone
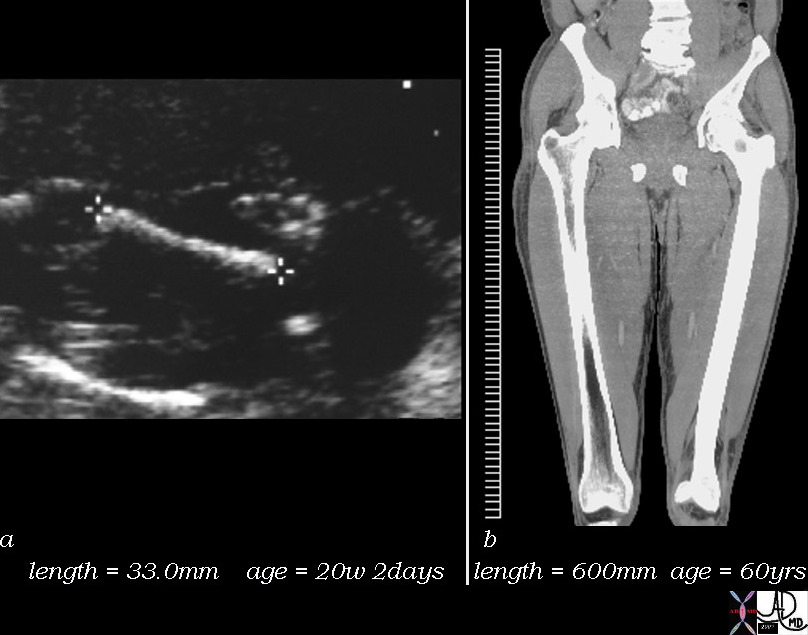
Femur – From Fetus to Adulthood |
| 48395c01 bone femur femoral length fetus adult age aaging time growth normal Davidoff MD |

Osteochondroma From the Knee I Flee |
| 75967.800 bone femur knee diaphysis osteochondroma from the knee I flee plain film plain X-ray Courtesy Ashley Davidoff MD |
References
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless? Textbook of Orthopaedics: Anatomy of the Femur (http://www.wheelessonline.com/ortho/anatomy_of_femur)