SIZE AS IT RELATES TO THE LUNGS There are many aspects of lung size that are both interesting and have in addition clinical relevance. It is important to understand in general that radius and length in the tubular conducting components have relevance, and that volume and surface area in the diffusion elements have relevance. The lungs are one of the more voluminous organs in the body but in terms of weight are relatively light for their size, since they mostly are filled with air. Additionally, their size can change dramatically since the difference in volume between a deep inspiration and deep expiration can be as much as 3.5 litres.
SURFACE ANATOMY Within the thorax the lungs extend superiorly passed clavicle into the base of the neck, with a cranio-caudad length in inspiration of approximately 24 cms. Anteriorly, on a chest X-Ray they reach to the 10 rib. Posteriorly, they extend superiorly to the first thoracic vertebrae and inferiorly to the dome of the diaphragm and are seen to the level of the 6th rib on a chest X-Ray. In patients with COPD or an acute asthmatic attack the lung volumes are expanded and the lungs will be seen beyond the 6th rib posteriorly and the 10th rib anteriorly.
WEIGHT: In the living and breathing adult, the lungs weigh approximately 900 t0 1200 grams, of which nearly 40% to 50% is blood. The weight will depend on how much blood is running through the lungs. At rest it is 5L/min, but during excercise with up to 25L/min flowing through the lungs, at any one time during excercise the lungs will be that much heavier. At rest the lungs weigh about the same as the liver, which by volume comparison is about 1/3 the volume of the lungs. In the adult, the right lung weighs about 630 grams and the left weighs 570 grams. The left lung is smaller, since the heart, which is dominantly a left sided structure, occupies part of the left chest. VOLUMES: The total volume of the lungs is about 6300ml in adult men and 4200ml in adult women. At end-expiration, the gas volume is about 2.5 L, whereas at maximal inspiration it may be 6 L. Taking a rate of 10-15 breaths per minute (about 17,000 breaths per 24 hours) results in approximately 10,000 liters of air inspired per day. Of course an equal amount has to be expired per day as well, and so there is the back and forth movement of about 20,000 litres per day. Alveoli make up approximately 50% of entire lung volume. The outer 1/3 of the lung contain 50% of the alveoli. Thus alveoli are the major component of the lung and they are situated peripherally dominantly. The lung and the kidney have some similarities in that the outer third of the kidney is dominantly cortex and contains most of the key functioning and filtering aspects of the kidney whereas the tubular system is medullary and located more centrally. This is reminiscent structurally of the description of the lung. In fact the lung has also been described as having an outer cortexand an inner medulla.
SURFACE AREA There are about 20,000 acini and 300 million alveoli. The total surface area of the lung is about 80 square meters, about the size of a tennis court. In order for an efficient mechanism of gas exchange to occur, blood and air have to meet at the alveolus where the diffusion process can take place. At rest 5 litres of blood flows through the lungs per minute and up to 25 litres per minute during excercise. There are many factors that allow for the exchange to take place but the lung does its part by providing a large patent surface area by virtue of its alveolar structure, and a tubular system that delivers fresh air efficiently. DENSITY: Density of the lung as measured in g/mL or if measured by CT in Hounsefield units (HU.)The density of the lung relates to the ratio of air to soft tissue. Thus during inspiration there will be an overall increase in the volume of air in the lung and thus an overall decrease in density. This translates into a measured density of 0.30 g/mL at functional residual capacity (FRC) to 0.14 g/mL at total lung capacity – more than 50% decrease in the overall density with a deep inspiration. In addition there is a density gradient from hilum to periphery, and between upper and lower parts of the lung. In fact positional differences in density (and distribution of air)and parts of the lung between the supine, prone and upright situation, play an important role in pulmonary health of the bedridden. Upstream in the hila, (or medulla of the lung) the solid components of the conduit structures are more prominent, and the volume of alveoli is relatively diminished, whereas in the outer cortex the air filled alveoli dominate. In fact the outer 1/3 of the lung, house 50% of the alveoli. This translates into a density difference between the innermost medulla and outermost ocortex of about 10 fold. Near the hilum therefore, the measured density is 1 g/mL and peripherally it is 0.1 g/mL. There is also difference in density from top to bottom. The blood flow distribution plays an important difference in this situation. All the pulmonary vessels are more distended in the lower lung fields. This is a well known observation of the radiologists on a CXR. In fact if the vessels to the upper lobes start looking either equal to or larger than the lower vessels it is a sign of cardiac failure.
SIZE AS IT RELATES TO THE TRACHEOBRONCHIAL TREE Consideration of the size of the conducting system as a tubular and transporting system is far different from the considerations given to the gas exchange system where surface area is the prime functional consideration. Length, radius, and number of divisions are the key considerations. Changes in the diameter of the the trachea can result in a significant difference in air flow and delivery. One of the major aspects of anaphylaxis is upper airway swelling – usually laryngospasm – and failure of delivery of air downstream. This is one of the causes of fatality during anaphylaxis, and return of airway patency is the first consideration in resuscitation. In fact, in any resuscitation, the “A” of the “ABC” of resuscitaion is to ensure patency of the airway first. The posterior tracheal wall is non cartilagenous and consists of a membrane. During expiration the membrane does normally move forward resulting in a narrower but insignificant narrowing. More downstream, patency of the bronchi and bronchioles is also very important. Collapse of a lung, segment, or subsegment of a lung can easily occur with foreign body inhalation, mucus, purulent impaction, or tumor growth. If there cannot be air delivery, the affected segment collapses and the all important surface area for the blood/gas exchange is lost. The respiratory system is quite forgiving and a person can function normally even with one lung removed since there are many compensatory mechanisms in place. LENGTH: In adults, the trachea ranges from 9 to 15 cm in length, terminating distally at the carina which represents the origins of the left and right mainstem bronchi. The distance from mouth to carina is about 25cms. The mainstem bronchi taken together have 40% more cross sectional area than the trachea. This increasing cross sectional area continues as we progress downstream so that resistance decreases, laminar flow evolves, and airflow is facilitated. This structural feature allows air from a single breath to reach all the alveoli virtually simeltaneously. The right bronchus is about 2.5 cm long, is wider, shorter, and more vertical in direction than the left. About 2 cm from its origin it gives off a branch to the upper lobe of the right lung. The left bronchus is nearly 5 cm long. It is therefore nearly twice the length of the right but it is smaller in diameter. The right is known as the short and fat one of the family. The left is the long and thin one. In addition to its gracile profile the left also has great athletic ability, as evidenced by its high jump over the left main stem bronchus. (hyparterial bronchus). The right does not make it over the right mainstem, and is happy in its jolly way of running under the right main stem bronchus (eparterial bronchus). The RUL bronchus is about 1cm in length. The apical bronchus is about 2cm in length. The RML bronchus is 1.2cm. The RLL basilar trunks average length measures, approximately 15 mm. LUL bronchus is short and fat and takes after its uncle on the right – it measures 9 mm in length (but 12mm in diameter). The ascending upper division bronchus on average is 1 cm in length. In situs inversus the right and left lung are reversed, so that the left lung is positioned in the right chest and the right lung in the left chest. The chest X-ray is the best and easiest way to make this diagnosis, since the air filled bronchi are easily seen. If the long and thin brother lies on the right, and the short and fat brother lies to the left, the condition of situs inversus of the lung exists. Sometimes this reflects the inversus situation in the abdomen, so the next step is to decide whether the stomach bubble is to the left or the right. The stomach bubble is almost always seen on the CXR, and if it lies to the right then situs inversus totalius exists. The CXR, more than 100 years old, is a marvelous diagnostic tool.
DIAMETER: The trachea has a maximum transverse diameter of 1.6cm, while A-P dimension is narrower, having a maximal dimension of 1.4cm. The transverse dimension of the trachea should not be less than 1.3cm in the male and 1 cm in the female, and similarly should not be more than 2.5cm in the male and 2.1cm in the female. The RUL bronchus is about 1cm in diameter, with the apical segment being 4-7mm, and the RML bronchus is about 8mms. As stated previously the LUL bronchus is short and fat and takes after its uncle on the right – it measures 12mm mm in diameter (but 9mm in length). The ascending upper division bronchus is approximately 7 mm in diameter. An acinus averages 0.75 mm in diameter. General diamters of the downstream airways include lobular and segmental bronchi (5-8mm), subsegmental bronchi and bronchiole (1.5-3mm), lobular bronchiole (1mm), terminal bronchiole (.7mm) and acinar bronchiole (.5mm). (Webb, Muller, Naidich.)
NUMBER OF DIVISIONS: The number of branches from hilum to periphery is variable with the shortest path to a terminal bronchiole being about 7 divisions and total length of 7 to 8 cm., and the longest pathway having about 25 branch divisions with total length of more than 22 cm. The main pulmonary artery (MPA) is usually about 3-4 cm in diameter being very similar to the aorta and twice the size of the trachea. The branch pulmonary arteries are each about the same size as the trachea, and thus the RPA and LPA are quite a bit larger than their counterparts the right and left mainstem bronchi. However, at the segmental level there is a catch up, so that the bronchi and arteries are equal in size. These comparative sizes are very important in the imaging world and size evaluation is very useful in the diagnosis of tracheomalacia, COPD (big trachea), tracheal narrowing, bronchiectasis, aortic aneurysm, pulmonary congestion, and pulmonary hypertension – all common medical conditions that have characteristic changes in size that are evaluated by comparing the sizes of the airways to the vessels. It should be noted that in dependant positions the artery may normally appear slightly larger than its counterpart.
THICKNESS Thickness of the downstream airways include lobular and segmental bronchi (1.5mm), subsegmental bronchi and bronchiole (.2-.3mm), lobular bronchiole (.15mm), terminal bronchiole (.1mm), and acinar bronchiole (.05mm). (Webb, Muller, Naidich.)
ANGLES: The left main stem bronchus leaves the trachea at a 135 degree angle. The right mainstem bronchus is more vertically oriented, with a 155 degree angle of origin. This carinal angle should be about 55 degrees and should not be more than 90 degrees. In patients with subcarinal disease including pathological lymph nodes (lyphoma and metastatic lung carcinoma), left atrial enlargement (mitral stenosis, regurgitaion and left heart failure), and large hiatus hernia, the carinal angle maty be widened. The carinal angle is therefore a very important landmark in the evaluation of the chest X-Ray.
DIVISIONS: Each lobe has 19 bronchopulmonary segments. There are approximately 23 airway divisions to the level of the alveoli.
NUMBERS: The lobule has 3-5 terminal bronchioles and their distal structures. 20,000 acini and 300 million alveoli. (compare 100 billion neurons in the brain.)
AREA: Cross-sectional area of the airways trachea 2.5 cm2 alveoli 11,800 cm2 There are about 20,000 acini and 300 million alveoli. The total surface area of the lung is about 80 square meters, about the size of a tennis court. TIME Gas exchange takes 0.25 seconds or 1/3 of the total transit time of a red cell. The entire blood volume of the body passes through the lungs each minute in the resting state, that is 5 liters per minute. All material which accumulates in the lungs is removed in about 24 hours.
FREQUENCIES Cilia beat at 1,000 to 1,500 cycles per minute resulting in cephalad movement of the mucus blanket at 0.5-1 mm/min in small airways and 5-20 mm/min in the trachea and main bronchi.
RELATIVE SIZE OF TISSUE COMPONENTS: About 10% of the lung is occupied by solid tissue, whereas the remainder is filled with air and blood. The right crura is thicker than the left. In the clinical realm, there are certain diseases that make the lungs abnormally large and those that reduce the size of the lungs or segments of the lungs. In the COPD group, including emphysema, there is air trapping so that what goes in does not come out because of the structural changes in the lung, resulting in hyperinflation and large lungs. Atelectasis and chronic interstitial lung diseases cause reduction in size of segmental lobar and lung in the group of diseases labelled chronic obstructive airway disease. In an acute astmatic attack there is air trapping making the lungs larger in volume than normal. The diappragmats get pushed down and become flattened. There are conditions where one lung and its blood vessels become
Size of the Lung
The Common Vein copyright 2008
Introduction
Size of the Lung
The lungs are one of the more voluminous organs in the body but in terms of weight are relatively light for their size, since they mostly are filled with air. Additionally, their size can change dramatically since the difference in volume between a deep inspiration and deep expiration can be as much as 3.5 liters.
Surface anatomy
Within the thorax the lungs extend superiorly passed clavicle into the base of the neck, with a craniocaudal length in inspiration of approximately 24 cms. Posteriorly, on a chest X-Ray they reach to the 10 rib. Cranially they extend to the first thoracic vertebrae and inferiorly to the dome of the diaphragm and costophrenic sulci more inferiorly.
In patients with COPD or an acute asthmatic attack the lung volumes are expanded and the lungs will be seen beyond the 6th rib anteriorly and the 10th rib posteriorly.
Weight
In the living and breathing adult, the lungs weigh approximately 900 to 1200 grams, of which nearly 40% to 50% is blood. The weight will depend on how much blood is running through the lungs. At rest it is 5L/min, but during exercise with up to 25L/min flowing through the lungs, at any one time during exercise the lungs will be that much heavier.
At rest the lungs together weigh about the same as the liver, which is 1/3 the volume of the lungs.
In the adult, the right lung weighs about 630 grams and the left weighs 570 grams. The left lung is smaller, since the heart, which is dominantly a left sided structure, occupies part of the left chest.
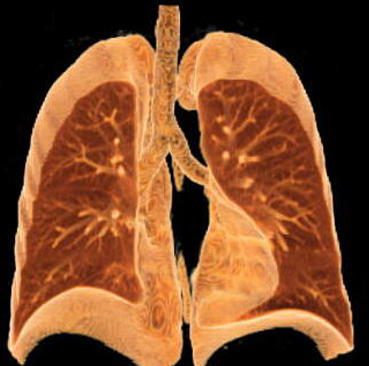
Volume of lung displaced by heart |
| A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right. Courtesy of: Doug Brown RT (R) and Ashley Davidoff MD. 32623 |
Volumes
The total volume of the lungs is about 6300ml in adult men and 4200ml in adult women. At end-expiration, the volume of air within the lungs is about 2.5 L, whereas at maximal inspiration it may be 6 L. Taking a rate of 10-15 breaths per minute (about 17,000 breaths per 24 hours) results in approximately 10,000 liters of air inspired per day. Of course an equal amount has to be expired per day as well, and so there is the back and forth movement of about 20,000 liters per day.
Alveoli make up approximately 50% of entire lung volume. The outer 1/3 of the lung contains 50% of the alveoli. Thus alveoli are the major component of the lung and they are situated dominantly in the periphery while the tubular transport systems are located centrally by the hilum . The lung and the kidney have structural similarities in that the outer third of the kidney called the cortex, contains most of the key functioning and filtering aspects of the kidney whereas the inner and more central medulla houses the tubular system. The similarity is such that some refer to the lung as having an outer cortex and an inner medulla.
Surface area
There are about 20,000 acini and 300 million alveoli in the normal lung. During inspiration the radius of the alveolus doubles from about 0.05 mm to 0.1 mm. The total surface area of the lung is about 80 square meters, about the size of a tennis court. The extent and volume of air that is moved across the alveoli is simply stunning.
As we have already seen about 5-10 liters of air is moved through the tracheobronchial tree per minute at rest. During exercise up to 100 liters of air can be moved through the airways per minute and about 3 liters of oxygen and 3 liters of carbon dioxide moved across the membrane. There are many factors that allow for the exchange to take place but the lung does its part by providing a large patent surface area by virtue of its alveolar structure.
Each organ system that requires a large working surface area for optimal function has adapted and evolved different structural tricks to accommodate need.. For example the small bowel has primary mucosal folds called called valvulae conniventes increase the surface area by about 3 times. The valvulae themselves have microscopic folds called villi which further increase the working surface by about 10 fold. Each villus has has about 1000 microvilli which increase the surface area by about another 20 fold. Overall the surface area of the 14-20 foot tube also has a surface area of a tennis court.
The kidneys also have devised a mechanism to increase surface area of their side by side epithelial surfaces that act as a filtering mechanism. On the one side, the capillaries bringing blood increase their surface area by convoluting into a ball, while on the other side the receiving membrane of the urinary system becomes a semispherical cup called Bowman?s capsule. The larger the surface area of this membrane, the more effective and efficient the function.
The lungs create the same increased space by bubbling, or ballooning out in the form of the alveoli. The gastrointestinal tract and kidney have more time to do their work. The lungs need all the time they can get since most of the exchange is done during inspiration and even more effectively between inspiration and expiration. The air that is inspired must present itself to the functional surface at large almost immediately, and the exchange has to take place before expiration starts when the air is whisked away to prepare for the next load.
Applied Anatomy
In the clinical realm, there are certain diseases that make the lungs abnormally large and those that reduce the size of the lungs or segments of the lungs.
The lungs will usually take up the available space in the chest so that if one part of the lung is collapsed or surgically removed then the remaining lung will take up the space. Similarly, if one lung is blocked or becomes smaller, then the other becomes hyperinflated resulting in shape and size changes t accommodate the deficiency.
In the COPD group, including emphysema, there is air trapping so that what goes in does not come out because of the structural changes in the lung, resulting in hyperinflation and large lungs. In an acute asthmatic attack there is air trapping making the lungs larger in volume than normal. The diaphragm gets pushed down and becomes flattened. Atelectasis is also part of the disease because thickened mucus, plugs the smaller airways and therefore air cannot get in and subsegmental and collapse occurs. Less commonly the mucus may block the airways at segmental and lobar level with significant consequences to an already compromised system. The diaphragm on the same side of the collapse becomes elevated to the degree that depends on the size of the collapse. The larger the collapse the greater the volume loss in the lungs, the greater the space that needs to be filled in, and hence the greater the elevation of the diaphragm. The concept of filling in space is also witnessed when a patient has had resection of part of the lung. The space usually is filled in by the remaining segments of the ipsilateral lung, but if there is insufficient ipsilateral lung to do the job, (fill in the space) it may be filled in by contralateral lung.
 Large volume lungs Large volume lungs |
| In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon?s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest. Courtesy Ashley Davidoff MD 41987c |
 Large volume lungs Large volume lungs |
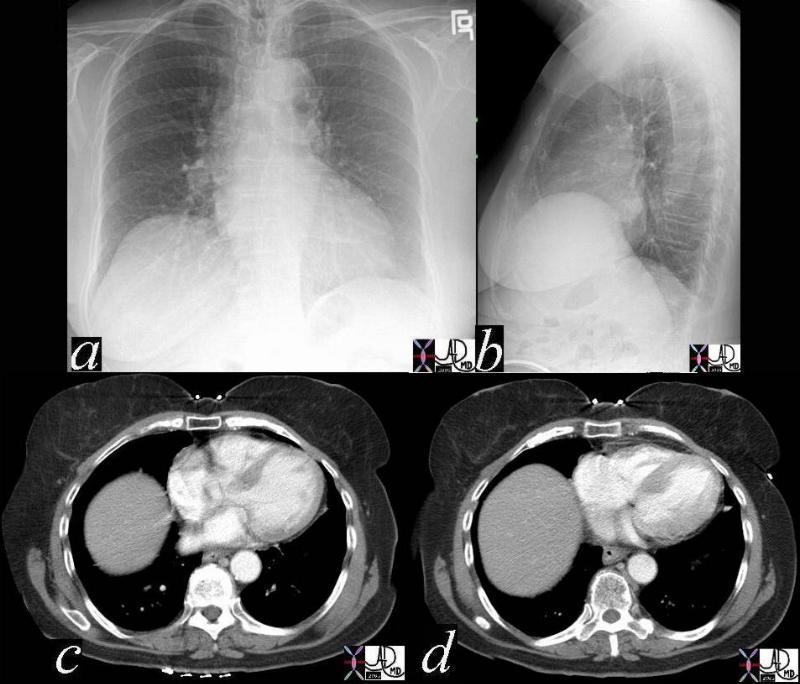
| In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, this has no clinical effect if the lungs are otherwise healthy. Courtesy Ashley Davidoff MD 41981c |
 Large volume lungs Large volume lungs |
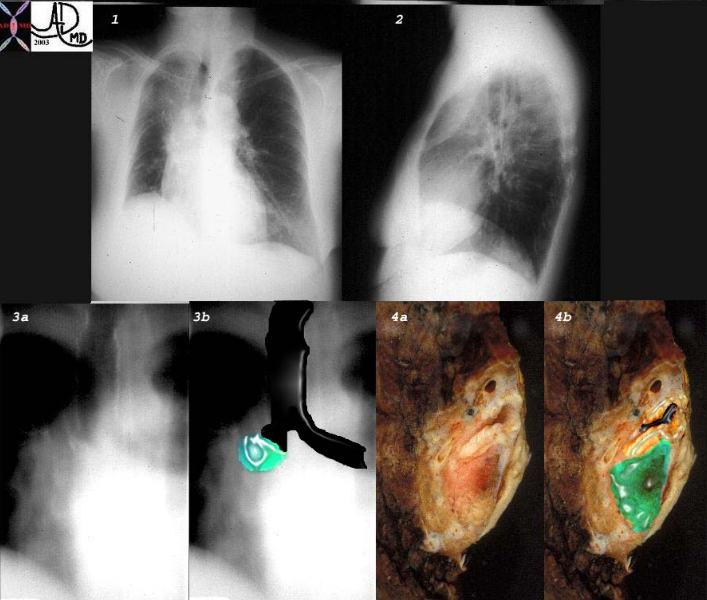
| This combination of images shows the manifestations of a malignant mass in the hilum causing obstruction of the right mainstem bronchus. There is an elevation of the right hilum on the CXR, and elevation of the right hemidiaphragm associated with collapse of the anterior segment of the RUL seen as a vague density in the PA CXR and an anterior pie shaped density of the lateral. The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus (the implied tumor overlaid in green). Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing the right mainstem from below and distorting and obstructing it. With the volume loss the right hemidiaphragm moves up to take up the void left by the volume loss of the lung.
32292cw Courtesy Ashley Davidoff MD |
 Normal vs Atelectasis Normal vs Atelectasis |
| 74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Normal vs Atelectasis
74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal vs Atelectasis
74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Normal vs Atelectasis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Normal vs Atelectasis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large volume lungs
This combination of images shows the manifestations of a malignant mass in the hilum causing obstruction of the right mainstem bronchus. There is an elevation of the right hilum on the CXR, and elevation of the right hemidiaphragm associated with collapse of the anterior segment of the RUL seen as a vague density in the PA CXR and an anterior pie shaped density of the lateral. The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus (the implied tumor overlaid in green). Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing the right mainstem from below and distorting and obstructing it. With the volume loss the right hemidiaphragm moves up to take up the void left by the volume loss of the lung.
32292cw Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large volume lungs
This combination of images shows the manifestations of a malignant mass in the hilum causing obstruction of the right mainstem bronchus. There is an elevation of the right hilum on the CXR, and elevation of the right hemidiaphragm associated with collapse of the anterior segment of the RUL seen as a vague density in the PA CXR and an anterior pie shaped density of the lateral. The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus (the implied tumor overlaid in green). Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing the right mainstem from below and distorting and obstructing it. With the volume loss the right hemidiaphragm moves up to take up the void left by the volume loss of the lung.
32292cw Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This combination of images shows the manifestations of a malignant mass in the hilum causing obstruction of the right mainstem bronchus. There is an elevation of the right hilum on the CXR, and elevation of the right hemidiaphragm associated with collapse of the anterior segment of the RUL seen as a vague density in the PA CXR and an anterior pie shaped density of the lateral. The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus (the implied tumor overlaid in green). Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing the right mainstem from below and distorting and obstructing it. With the volume loss the right hemidiaphragm moves up to take up the void left by the volume loss of the lung.
32292cw Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This combination of images shows the manifestations of a malignant mass in the hilum causing obstruction of the right mainstem bronchus. There is an elevation of the right hilum on the CXR, and elevation of the right hemidiaphragm associated with collapse of the anterior segment of the RUL seen as a vague density in the PA CXR and an anterior pie shaped density of the lateral. The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus (the implied tumor overlaid in green). Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing the right mainstem from below and distorting and obstructing it. With the volume loss the right hemidiaphragm moves up to take up the void left by the volume loss of the lung.
32292cw Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Large volume lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Large volume lungs
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large volume lungs
In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, this has no clinical effect if the lungs are otherwise healthy. Courtesy Ashley Davidoff MD 41981c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large volume lungs
In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, this has no clinical effect if the lungs are otherwise healthy. Courtesy Ashley Davidoff MD 41981c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, this has no clinical effect if the lungs are otherwise healthy. Courtesy Ashley Davidoff MD 41981c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, this has no clinical effect if the lungs are otherwise healthy. Courtesy Ashley Davidoff MD 41981c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Large volume lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Large volume lungs
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large volume lungs
In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon?s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest. Courtesy Ashley Davidoff MD 41987c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large volume lungs
In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon?s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest. Courtesy Ashley Davidoff MD 41987c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon?s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest. Courtesy Ashley Davidoff MD 41987c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon?s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest. Courtesy Ashley Davidoff MD 41987c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Large volume lungs
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Large volume lungs
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Volume of lung displaced by heart
A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right. Courtesy of: Doug Brown RT (R) and Ashley Davidoff MD. 32623
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Volume of lung displaced by heart
A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right. Courtesy of: Doug Brown RT (R) and Ashley Davidoff MD. 32623
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right. Courtesy of: Doug Brown RT (R) and Ashley Davidoff MD. 32623
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right. Courtesy of: Doug Brown RT (R) and Ashley Davidoff MD. 32623
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Volume of lung displaced by heart
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Volume of lung displaced by heart
)
