
Size of the Colon
The Common Vein Copyright 2008
Introduction
The SIZE Length: = Transverse: = Antero-posterior: = Weight = Volume = “It is about 1.5 meters long, being one-fifth of the whole extent of the intestinal canal. Its caliber is largest at its commencement at the cecum, and gradually diminishes as far as the rectum, where there is a dilatation of considerable size just above the anal canal. It differs from the small intestine in its greater caliber”
| Description of the Colon
The Common Vein Coyright 2007
Size The overall length of the colon is 150cms (about 5 feet), and is about 1/5 the length of the small bowel. On average itsdiameter is about 5cms. which is about twice the diameter of the small bowel. It is widest regions are located in the cecum, sigmoid and rectum, while its narrowest diamter is found in the descending colon which when empty simulates the size of the small bowel. The size varies significantly based on functional state and contents.
Shape The colon has a tubular, saccular shape caused by the presence of the haustral markings, semilunar folds or plica semilunares which are ridges that raise the mucosa so that the mucosa is not completely flat. The pleating effect is caused by the presence of the taenia coli which as mentioned are longitudinal mucle bands that run the length of the colon, and which are shorter thann the colon and hence the pleating effect and the sacculkar haustra. When the taenia contract they become even shorter and the haustrra become more apparent. The colon is characterized by the absence of villi on the mucosal surface, but the presence of mucosal infoldings called crypts of Lieberkuhn. The fatty excrescences called the appendices epiploica on the outer surface are unique and characteristic. Position The colon occupies the entire abdominal cavity and lies within the intraperitoneal, retroperitoneal, and the extraperitoneal spaces. It frames the abdominal cavity with the ascending and descending components being the lateral borders and the transverse a superior border. The transverse colon when redundant however coan drop down into thw pelvis while the sigm,oid when it is redundant can reach the upper abdomen. The most cranial aspect is usually at the splenic flexure and the most caudal aspect at the rectum. The ascending colon and descending colon are relatively posterior while the transverse colon is anterior. The ascending colon and descending colon have a vertical axis and the transverse colon has a relatively horizontal axis. Character The mucosa should be pink while the adventitia and serosa are usually paler. To the feel it is muscular, membranous, and distensible.
Relations Overall the mostimportant and relevant relations of the colon are to the mesenteric attachments, urinary bladder and stomach. The rectal relations include the sacrum, and coccyx which lie posteriorly, while anteriorly in the male the fundus of the bladder, the ureters, ductus deferentia, seminal vesicles and prostate lie. In the female the cul de sac lies anteriorly followed by the lower uterine segment cervix and vagina.
Applied AnatomyWhen is the colon too large?
There is a significant difference in clinical implications between an enlarged colon that is an acute presentation and one in which it is chronic. The colon can accomodate large volumes of stool if this is a slow chronic process whereas if it is acute, the blood flow can be compromised, which may be complicated by ischemia and infarction with subsequent rupture. Spillage of stool into the abdominal cavity is tantamount to bacterial warfare and is an extermely serious and often fatal entity. The acute entities include large bowel obstruction, cecal and sigmoid volvulus, and Ogilvie’s syndrome which is a colonic ileus, and toxic megacolon. These will be discussed in further detail in the sections below. The chronic forms of megacolon and megarectum are seen in institutionalised patients and quadriplegic patients and other patients who have neurologic deficit to the colon. Hirshsprungs disease is a congenital absence of nerves ina segment of the bowel wall which results in a functional obstruction. The actual measurements that define an enlarged colon have to used with caution since there is such variability in size between tpatients. As a general rule the following sizes are concerning; a cecum that is larger than 12cms, an ascending colon larger than 8cms, and a rectosigmoid that is greater than 6.5cms.
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting. |

DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
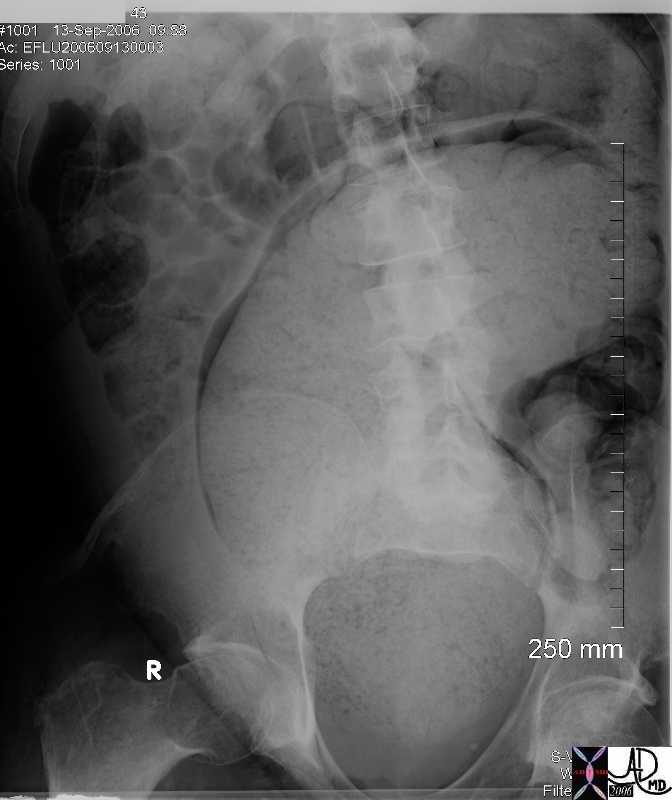
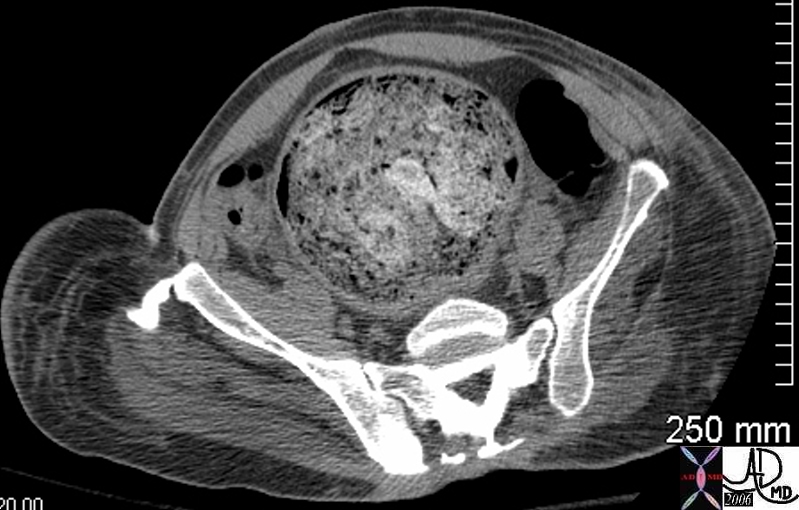
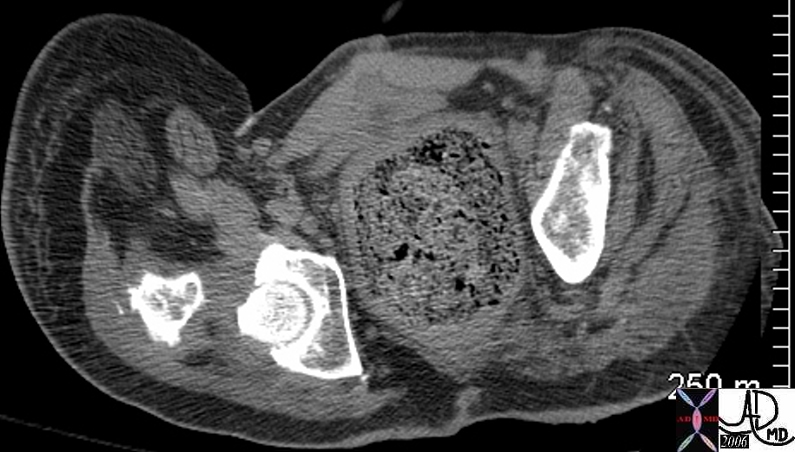
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Sigmoid and rectal impaction with megacolon and no obstruction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Sigmoid and rectal impaction with megacolon and no obstruction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
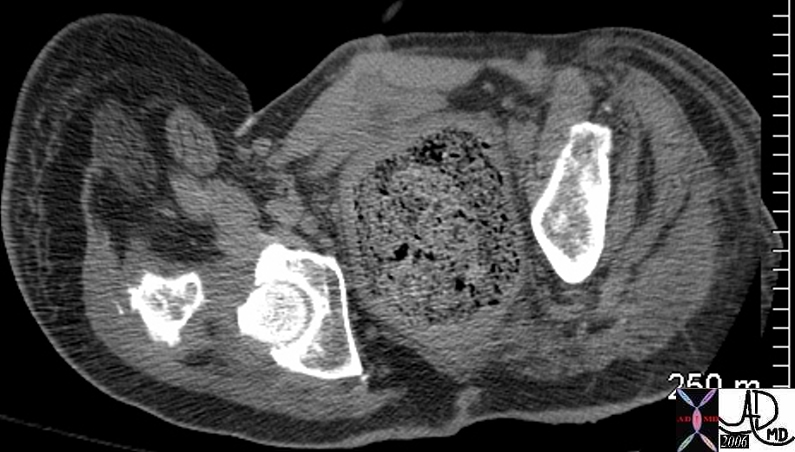
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Sigmoid megacolon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Sigmoid megacolon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Chronic megacolon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Chronic megacolon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
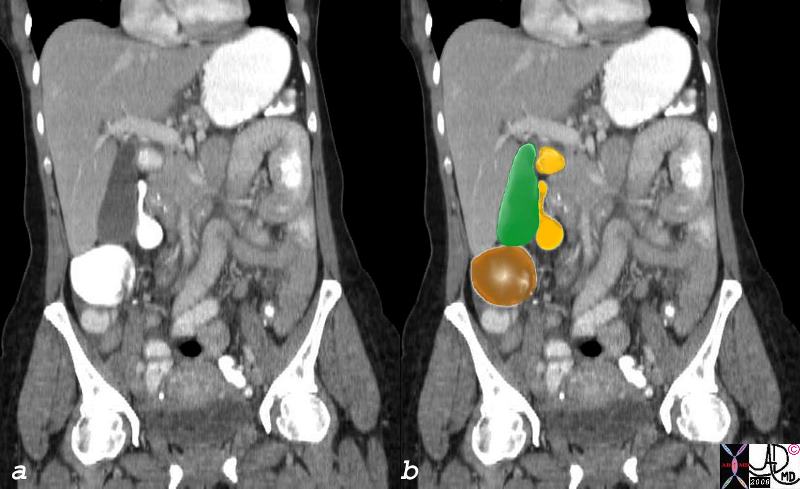
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Relation to the Colon and Duodenum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Relation to the Colon and Duodenum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Description of the Colon
The Common Vein Coyright 2007
Size
The overall length of the colon is 150cms (about 5 feet), and is about 1/5 the length of the small bowel. On average itsdiameter is about 5cms. which is about twice the diameter of the small bowel. It is widest regions are located in the cecum, sigmoid and rectum, while its narrowest diamter is found in the descending colon which when empty simulates the size of the small bowel. The size varies significantly based on functional state and contents.
Shape
The colon has a tubular, saccular shape caused by the presence of the haustral markings, semilunar folds or plica semilunares which are ridges that raise the mucosa so that the mucosa is not completely flat. The pleating effect is caused by the presence of the taenia coli which as mentioned are longitudinal mucle bands that run the length of the colon, and which are shorter thann the colon and hence the pleating effect and the sacculkar haustra. When the taenia contract they become even shorter and the haustrra become more apparent. The colon is characterized by the absence of villi on the mucosal surface, but the presence of mucosal infoldings called crypts of Lieberkuhn. The fatty excrescences called the appendices epiploica on the outer surface are unique and characteristic.
Position
The colon occupies the entire abdominal cavity and lies within the intraperitoneal, retroperitoneal, and the extraperitoneal spaces. It frames the abdominal cavity with the ascending and descending components being the lateral borders and the transverse a superior border. The transverse colon when redundant however coan drop down into thw pelvis while the sigm,oid when it is redundant can reach the upper abdomen.
The most cranial aspect is usually at the splenic flexure and the most caudal aspect at the rectum. The ascending colon and descending colon are relatively posterior while the transverse colon is anterior. The ascending colon and descending colon have a vertical axis and the transverse colon has a relatively horizontal axis.
Character
The mucosa should be pink while the adventitia and serosa are usually paler. To the feel it is muscular, membranous, and distensible.
Relations
Overall the mostimportant and relevant relations of the colon are to the mesenteric attachments, urinary bladder and stomach.
The rectal relations include the sacrum, and coccyx which lie posteriorly, while anteriorly in the male the fundus of the bladder, the ureters, ductus deferentia, seminal vesicles and prostate lie. In the female the cul de sac lies anteriorly followed by the lower uterine segment cervix and vagina.
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
Applied Anatomy
When is the colon too large?
There is a significant difference in clinical implications between an enlarged colon that is an acute presentation and one in which it is chronic. The colon can accomodate large volumes of stool if this is a slow chronic process whereas if it is acute, the blood flow can be compromised, which may be complicated by ischemia and infarction with subsequent rupture. Spillage of stool into the abdominal cavity is tantamount to bacterial warfare and is an extermely serious and often fatal entity.
The acute entities include large bowel obstruction, cecal and sigmoid volvulus, and Ogilvie’s syndrome which is a colonic ileus, and toxic megacolon. These will be discussed in further detail in the sections below. The chronic forms of megacolon and megarectum are seen in institutionalised patients and quadriplegic patients and other patients who have neurologic deficit to the colon. Hirshsprungs disease is a congenital absence of nerves ina segment of the bowel wall which results in a functional obstruction.
The actual measurements that define an enlarged colon have to used with caution since there is such variability in size between tpatients. As a general rule the following sizes are concerning;
a cecum that is larger than 12cms, an ascending colon larger than 8cms, and a rectosigmoid that is greater than 6.5cms.
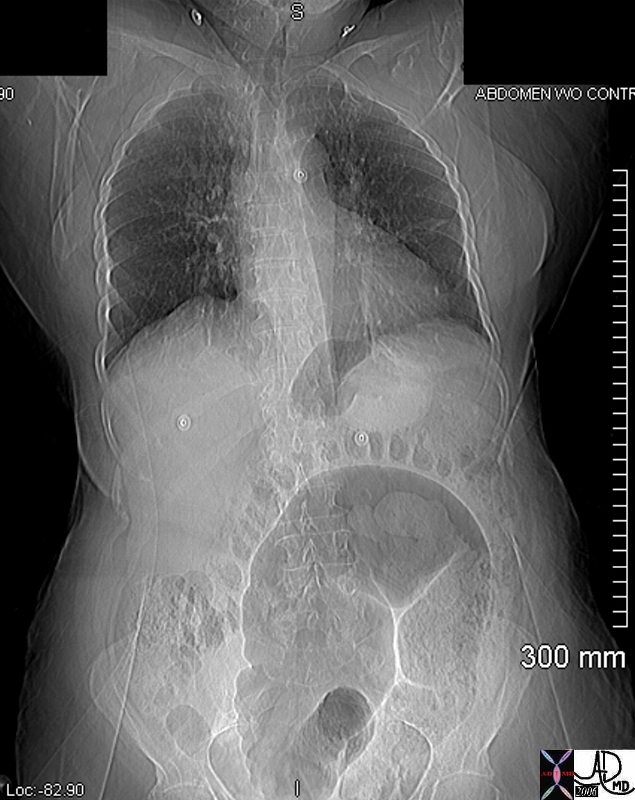
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
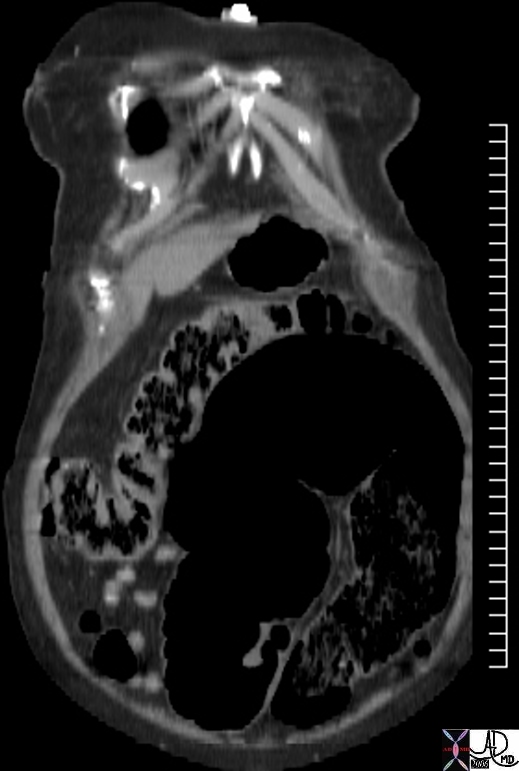
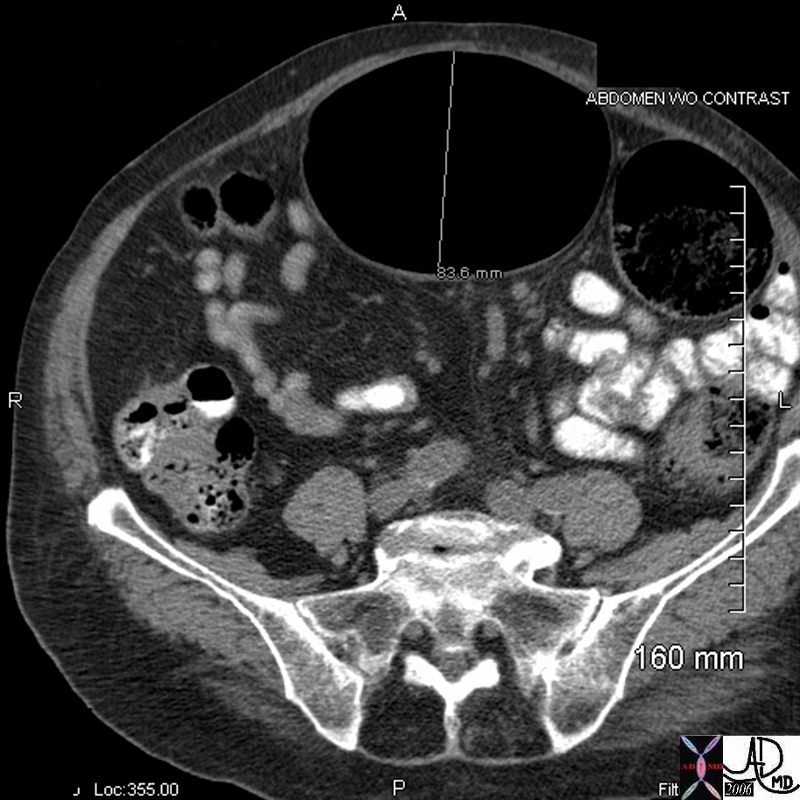
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
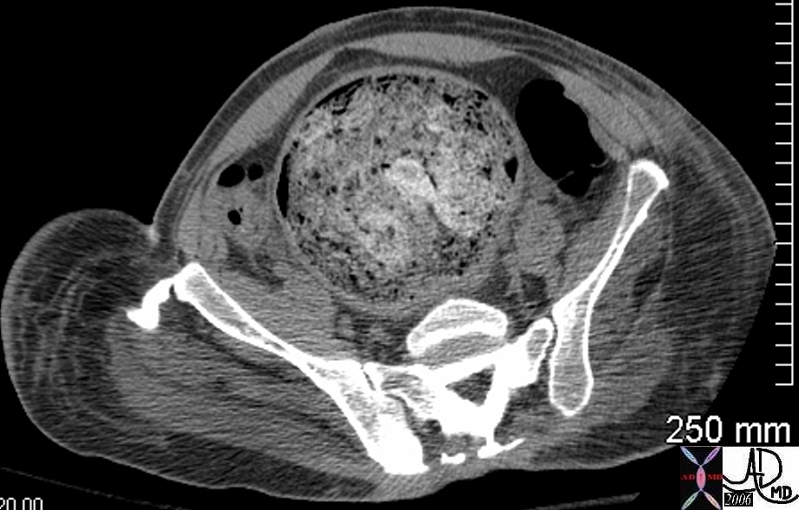
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Description of the Colon
The Common Vein Coyright 2007
Size
The overall length of the colon is 150cms (about 5 feet), and is about 1/5 the length of the small bowel. On average itsdiameter is about 5cms. which is about twice the diameter of the small bowel. It is widest regions are located in the cecum, sigmoid and rectum, while its narrowest diamter is found in the descending colon which when empty simulates the size of the small bowel. The size varies significantly based on functional state and contents.
Shape
The colon has a tubular, saccular shape caused by the presence of the haustral markings, semilunar folds or plica semilunares which are ridges that raise the mucosa so that the mucosa is not completely flat. The pleating effect is caused by the presence of the taenia coli which as mentioned are longitudinal mucle bands that run the length of the colon, and which are shorter thann the colon and hence the pleating effect and the sacculkar haustra. When the taenia contract they become even shorter and the haustrra become more apparent. The colon is characterized by the absence of villi on the mucosal surface, but the presence of mucosal infoldings called crypts of Lieberkuhn. The fatty excrescences called the appendices epiploica on the outer surface are unique and characteristic.
Position
The colon occupies the entire abdominal cavity and lies within the intraperitoneal, retroperitoneal, and the extraperitoneal spaces. It frames the abdominal cavity with the ascending and descending components being the lateral borders and the transverse a superior border. The transverse colon when redundant however coan drop down into thw pelvis while the sigm,oid when it is redundant can reach the upper abdomen.
The most cranial aspect is usually at the splenic flexure and the most caudal aspect at the rectum. The ascending colon and descending colon are relatively posterior while the transverse colon is anterior. The ascending colon and descending colon have a vertical axis and the transverse colon has a relatively horizontal axis.
Character
The mucosa should be pink while the adventitia and serosa are usually paler. To the feel it is muscular, membranous, and distensible.
Relations
Overall the mostimportant and relevant relations of the colon are to the mesenteric attachments, urinary bladder and stomach.
The rectal relations include the sacrum, and coccyx which lie posteriorly, while anteriorly in the male the fundus of the bladder, the ureters, ductus deferentia, seminal vesicles and prostate lie. In the female the cul de sac lies anteriorly followed by the lower uterine segment cervix and vagina.
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
Applied Anatomy
When is the colon too large?
There is a significant difference in clinical implications between an enlarged colon that is an acute presentation and one in which it is chronic. The colon can accomodate large volumes of stool if this is a slow chronic process whereas if it is acute, the blood flow can be compromised, which may be complicated by ischemia and infarction with subsequent rupture. Spillage of stool into the abdominal cavity is tantamount to bacterial warfare and is an extermely serious and often fatal entity.
The acute entities include large bowel obstruction, cecal and sigmoid volvulus, and Ogilvie’s syndrome which is a colonic ileus, and toxic megacolon. These will be discussed in further detail in the sections below. The chronic forms of megacolon and megarectum are seen in institutionalised patients and quadriplegic patients and other patients who have neurologic deficit to the colon. Hirshsprungs disease is a congenital absence of nerves ina segment of the bowel wall which results in a functional obstruction.
The actual measurements that define an enlarged colon have to used with caution since there is such variability in size between tpatients. As a general rule the following sizes are concerning;
a cecum that is larger than 12cms, an ascending colon larger than 8cms, and a rectosigmoid that is greater than 6.5cms.
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Sigmoid and rectal impaction with megacolon and no obstruction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Sigmoid and rectal impaction with megacolon and no obstruction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Sigmoid megacolon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Sigmoid megacolon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Chronic megacolon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Chronic megacolon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Relation to the Colon and Duodenum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Relation to the Colon and Duodenum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 33
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Description of the Colon
The Common Vein Coyright 2007
Size
The overall length of the colon is 150cms (about 5 feet), and is about 1/5 the length of the small bowel. On average itsdiameter is about 5cms. which is about twice the diameter of the small bowel. It is widest regions are located in the cecum, sigmoid and rectum, while its narrowest diamter is found in the descending colon which when empty simulates the size of the small bowel. The size varies significantly based on functional state and contents.
Shape
The colon has a tubular, saccular shape caused by the presence of the haustral markings, semilunar folds or plica semilunares which are ridges that raise the mucosa so that the mucosa is not completely flat. The pleating effect is caused by the presence of the taenia coli which as mentioned are longitudinal mucle bands that run the length of the colon, and which are shorter thann the colon and hence the pleating effect and the sacculkar haustra. When the taenia contract they become even shorter and the haustrra become more apparent. The colon is characterized by the absence of villi on the mucosal surface, but the presence of mucosal infoldings called crypts of Lieberkuhn. The fatty excrescences called the appendices epiploica on the outer surface are unique and characteristic.
Position
The colon occupies the entire abdominal cavity and lies within the intraperitoneal, retroperitoneal, and the extraperitoneal spaces. It frames the abdominal cavity with the ascending and descending components being the lateral borders and the transverse a superior border. The transverse colon when redundant however coan drop down into thw pelvis while the sigm,oid when it is redundant can reach the upper abdomen.
The most cranial aspect is usually at the splenic flexure and the most caudal aspect at the rectum. The ascending colon and descending colon are relatively posterior while the transverse colon is anterior. The ascending colon and descending colon have a vertical axis and the transverse colon has a relatively horizontal axis.
Character
The mucosa should be pink while the adventitia and serosa are usually paler. To the feel it is muscular, membranous, and distensible.
Relations
Overall the mostimportant and relevant relations of the colon are to the mesenteric attachments, urinary bladder and stomach.
The rectal relations include the sacrum, and coccyx which lie posteriorly, while anteriorly in the male the fundus of the bladder, the ureters, ductus deferentia, seminal vesicles and prostate lie. In the female the cul de sac lies anteriorly followed by the lower uterine segment cervix and vagina.
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
Applied Anatomy
When is the colon too large?
There is a significant difference in clinical implications between an enlarged colon that is an acute presentation and one in which it is chronic. The colon can accomodate large volumes of stool if this is a slow chronic process whereas if it is acute, the blood flow can be compromised, which may be complicated by ischemia and infarction with subsequent rupture. Spillage of stool into the abdominal cavity is tantamount to bacterial warfare and is an extermely serious and often fatal entity.
The acute entities include large bowel obstruction, cecal and sigmoid volvulus, and Ogilvie’s syndrome which is a colonic ileus, and toxic megacolon. These will be discussed in further detail in the sections below. The chronic forms of megacolon and megarectum are seen in institutionalised patients and quadriplegic patients and other patients who have neurologic deficit to the colon. Hirshsprungs disease is a congenital absence of nerves ina segment of the bowel wall which results in a functional obstruction.
The actual measurements that define an enlarged colon have to used with caution since there is such variability in size between tpatients. As a general rule the following sizes are concerning;
a cecum that is larger than 12cms, an ascending colon larger than 8cms, and a rectosigmoid that is greater than 6.5cms.
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Description of the Colon
The Common Vein Coyright 2007
Size
The overall length of the colon is 150cms (about 5 feet), and is about 1/5 the length of the small bowel. On average itsdiameter is about 5cms. which is about twice the diameter of the small bowel. It is widest regions are located in the cecum, sigmoid and rectum, while its narrowest diamter is found in the descending colon which when empty simulates the size of the small bowel. The size varies significantly based on functional state and contents.
Shape
The colon has a tubular, saccular shape caused by the presence of the haustral markings, semilunar folds or plica semilunares which are ridges that raise the mucosa so that the mucosa is not completely flat. The pleating effect is caused by the presence of the taenia coli which as mentioned are longitudinal mucle bands that run the length of the colon, and which are shorter thann the colon and hence the pleating effect and the sacculkar haustra. When the taenia contract they become even shorter and the haustrra become more apparent. The colon is characterized by the absence of villi on the mucosal surface, but the presence of mucosal infoldings called crypts of Lieberkuhn. The fatty excrescences called the appendices epiploica on the outer surface are unique and characteristic.
Position
The colon occupies the entire abdominal cavity and lies within the intraperitoneal, retroperitoneal, and the extraperitoneal spaces. It frames the abdominal cavity with the ascending and descending components being the lateral borders and the transverse a superior border. The transverse colon when redundant however coan drop down into thw pelvis while the sigm,oid when it is redundant can reach the upper abdomen.
The most cranial aspect is usually at the splenic flexure and the most caudal aspect at the rectum. The ascending colon and descending colon are relatively posterior while the transverse colon is anterior. The ascending colon and descending colon have a vertical axis and the transverse colon has a relatively horizontal axis.
Character
The mucosa should be pink while the adventitia and serosa are usually paler. To the feel it is muscular, membranous, and distensible.
Relations
Overall the mostimportant and relevant relations of the colon are to the mesenteric attachments, urinary bladder and stomach.
The rectal relations include the sacrum, and coccyx which lie posteriorly, while anteriorly in the male the fundus of the bladder, the ureters, ductus deferentia, seminal vesicles and prostate lie. In the female the cul de sac lies anteriorly followed by the lower uterine segment cervix and vagina.
Relation to the Colon and Duodenum
37957c01.8s gallbladder position relations colon duodenum abdomen normal anatomy CTscan Courtesy Ashley Davidoff MD copyright 2008
Applied Anatomy
When is the colon too large?
There is a significant difference in clinical implications between an enlarged colon that is an acute presentation and one in which it is chronic. The colon can accomodate large volumes of stool if this is a slow chronic process whereas if it is acute, the blood flow can be compromised, which may be complicated by ischemia and infarction with subsequent rupture. Spillage of stool into the abdominal cavity is tantamount to bacterial warfare and is an extermely serious and often fatal entity.
The acute entities include large bowel obstruction, cecal and sigmoid volvulus, and Ogilvie’s syndrome which is a colonic ileus, and toxic megacolon. These will be discussed in further detail in the sections below. The chronic forms of megacolon and megarectum are seen in institutionalised patients and quadriplegic patients and other patients who have neurologic deficit to the colon. Hirshsprungs disease is a congenital absence of nerves ina segment of the bowel wall which results in a functional obstruction.
The actual measurements that define an enlarged colon have to used with caution since there is such variability in size between tpatients. As a general rule the following sizes are concerning;
a cecum that is larger than 12cms, an ascending colon larger than 8cms, and a rectosigmoid that is greater than 6.5cms.
Chronic megacolon
This plain film is from an asymptomatic institutionalized patient. Talking about an organ that jumps out at you from the film ? diagnosis ? chronic megacolon. Previous films over a few years had shown similar appearance in this asymptomatic patient (aside from chronic abdominal distension) and hence sigmoid volvulus was not a clinical consideration.
Courtesy Ashley Davidoff MD
16667
Sigmoid megacolon
A CT performed shows that the sigmoid measured 8.3cms in diameter and was filled with air.
Courtesy Ashley Davidoff MD
45450 45451 45454
Sigmoid and rectal impaction with megacolon and no obstruction
In this case there is impaction of feces in the sigmoid colon and rectum but there is no evidence of obstruction since the rest of the colon is not dilated. These findings were of a chronic nature and unchanged. A diagnosis of chronic megacolon is likely.
Courtesy Ashley Davidoff MD
45461 45462 45464
Although it is rather surprising that the patient above was not obstructed other complications such as stercoral ulcers due to chronic irritation of the feces on the mucosa, and bowel ischemia from vascular compromise must be considered in the appropriate clinical setting.
)