Laura Miller MD Ashley Davidoff MD
The Common Vein Copyright 2010
Introduction
The menstrual cycle is a physiological process of the uterus caused by the cyclic rise and fall of estrogen and progesterone levels.
The result is growth and maturation of the endometrium followed by endometrial degeneration and shedding at menses.
Phases
The menstrual cycle is described in three phases, the proliferative, secretory and menstrual phases.
In the proliferative phase, the structural changes are characterized by proliferation of the endometrial glands and stroma. The functional changes are characterized by estrogen production by the ovarian follicle to produce this endometrial growth.
In the secretory phase, the structural changes are characterized by vascular growth and maturation of the cells in the endometrial glands.
The functional changes are characterized by a fall in ovarian estrogen production after ovulation with increasing progesterone production by the ovarian corpus luteum. This hormone production causes the endometrial glands to mature and produce multiple secretory products which allow implantation of an embryo.
The purpose of the proliferative and secretory phases are to produce an ideal environment for embryo implantation after ovulation. If no embryo implants, then the menstrual phase of the cycle begins. The structural changes of the menstrual phase are characterized by degeneration and shedding of the endometrium. This shedding is seen as bleeding at menses. The functional changes are characterized by a fall in progesterone levels as the ovary?s corpus luteum degenerates. This hormonal change produces an increase in the production of digestive enzymes within the endometrium as well as infiltration of the endometrium with inflammatory cells. These changes combined with endometrial vasoconstriction lead to the degeneration and shedding of the endometrium. Disorders of the menstrual cycle include excess bleeding at or between menses (menorrhagia, metrorrhagia, menometrorrhagia), irregular or infrequent menses (oligomenorrhea), a lack of menstrual flow (amenorrhea), pain at menses (dysmenorrhea), or physical and behavioral symptoms that occur in the second half of the menstrual cycle (Premenstrual syndrome). These disorders are diagnosed based on clinical history and physical exam. Disorders of the menstrual cycle have multiple causes and their evaluation includes history, physical exam, pregnancy testing and imaging with ultrasound, hysterosalpingogram and MRI. Treatment depends on the cause found at evaluation.
Size and the Menstrual Cycle
The cyclical changes of the menstrual cycle present a continual change of events controlled by a series of integrated hormonal events. These changes are most easily observed in the endometrium by ultrasound. During the menses, the endometrium sheds and becomes thinner, the junctional zone is irregulalrly thick, and the myometrium loses water and thins.
Changes in the Endometrial Stripe
During the menstrual cycle the ultrasound appearance can characterise and date the phase of the cycle. (Nalaboff) Following menses there is a thin echogenic line which measures between 1-4mms, (Nalaboff) which progressively thickens and changes to a multilayered configuration. On ultrasound the measurement is from echogenic border to echogenic border in the sagittal plane.
First Week Post Menstruation
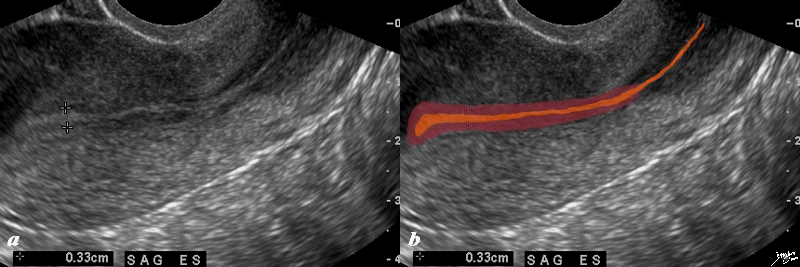
Early Proliferative Phase |
|
The normal sagittal view of the uterus is a transvaginal ultrasound, in the first week after menstruation after menstruation, and just prior to the next menstruation after the endometrium has been shed. It demonstrates that the endometrium becomes a single echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (tan). This layer is more compacted, and relatively hypovascular. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has fallen. The endometrium in this case measures about 3mms
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84698c02b.8s
|
In the proliferative phase (day6-14) the endometrium thickens to 5-7mmsand becomes more echogenic than the myometrium.This reflects growth of the endometrial glands blood vessels and stroma, stimulated by estrogen production by the ovarian follicles. This proliferative endometrium is structurally and functionallly prepared for implantation of the fertilised egg. In the late proliferative phase (periovulatory phase), the endometrium becomes multilayered, with an echogenic basal layer, hypoechoic inner functional layer and a thin echogenic line
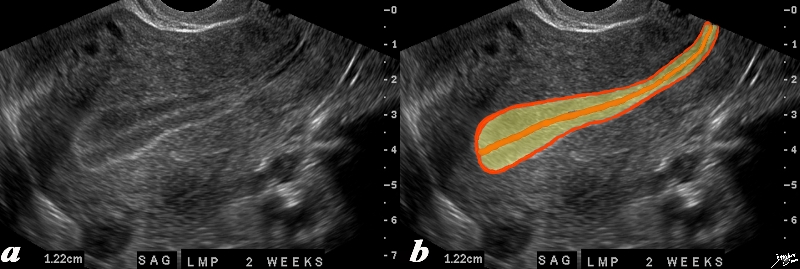
Trilaminar Appearance – Midcycle Preovulation
End of Proliferative Phase |
|
The normal sagittal view of the uterus is a transvaginal ultrasound, 2 weeks after menstruation, and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This pahse is also called the follicular phase, or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe”, and conversely, its presence is seen before progesterone is produced. If present with a 9mm+ diameter, it reflects an ideal potential lining for fertilization.. In this case it measured 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83835c02.8s
|
Following ovulation, the endometrium is under the influence of progesterone secretion by the corpus luteum. The endometrial glands fill up with mucus. The resulting appearance of the endometrium is a thick echogenic structure (secretory phase) The endometrium is at its thickest at this stage (< 14mm). As luteinizing hormone levels fall in the latter phase of the cycle, the level of progesterone falls, and there is shedding of the endometrium. Thus, the cyclical changes of the endometrium (invisible, thin echogenic, multi-layered, thick echogenic) reflect the phases of the menstrual cycle. “Transvaginal ultrasound revealing an endometrial stripe of less than 5 mm is reassuring and essentially rules out cancer (3). An endometrial stripe greater than 4 mm necessitates endometrial sampling, preferably with in-office use of a Pipelle endometrial suction curette or similar device”
In the periovulatory phase the myometrium and endometrium start to thicken, and the junctional zone becomes more easily identified (Kido)
There are 3 distinct zones or parts of the uterus which vary in size and character during each of the menstrual phases.
Endometrial Changes During the Cycle
During the follicular phase (proliferative phase) which occurs in the first half of the cycle, and after the shedding of the endometrial lining, there is a rise in estrogen which causes the endometrial lining to start to thicken. In mid cycle after ovulation, luteinizing hormone is released, which heralds in the luteal phase (aka secretory phase). Progesterone now rises and further proliferation of the endometrium occurs. In the absence of pregnancy progesterone levels and estrogen levels fall, and the endometrium sheds. The cervical canal has a maximal dimension of 8mms.
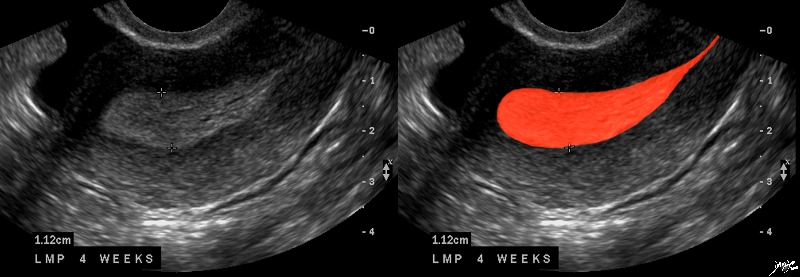
Premenstrual Endometrium
End of Secretory Phase |
|
The normal sagittal view of the uterus is a transvaginal ultrasound, about 4 weeks after menstruation, and just prior to the next menstrauation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 46318c01.8s
|
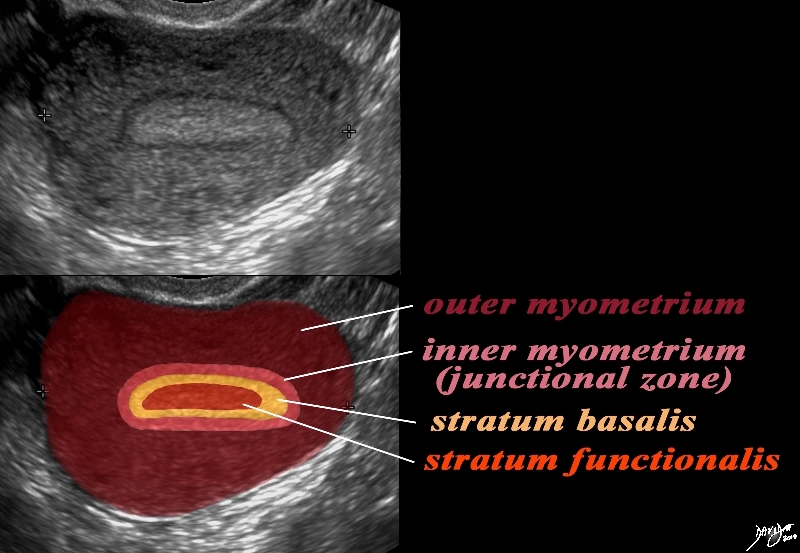
The Layers in the Premenstrual Uterus
Stratum Basalis and Stratum Functionalis are Not Distinguished by this US and appear as One LAyer |
|
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540cc06.8s
|
Spiral Arteries Staratum Functionalis and Menstruation |
|
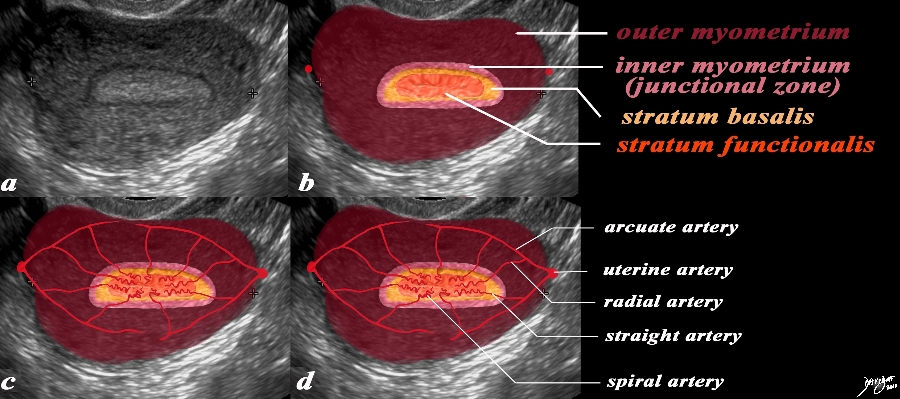
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. (a) The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon). (b) In the second series of images (c,d) the blood supply of the uterus is exemplified to demonstrate the branches that lead to the spiral arteries which undergo vasoconstriction at the time of the menses resulting in ischemia of the functionalis and subsequent shedding . The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.2kc07L.9s
|
The Spiral Arteries and the Stratum Functionalis |
|
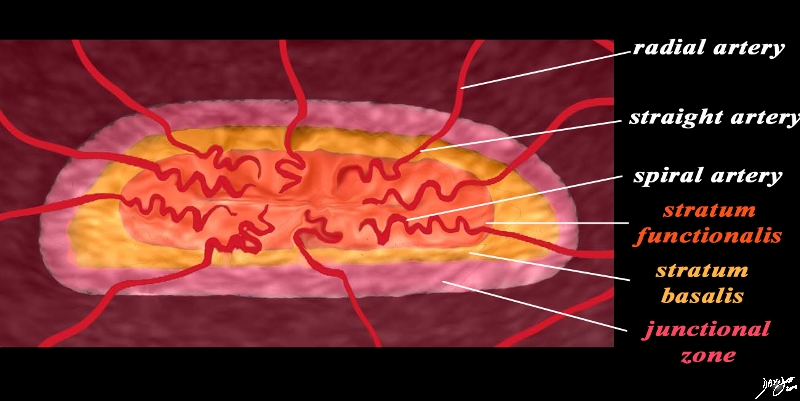
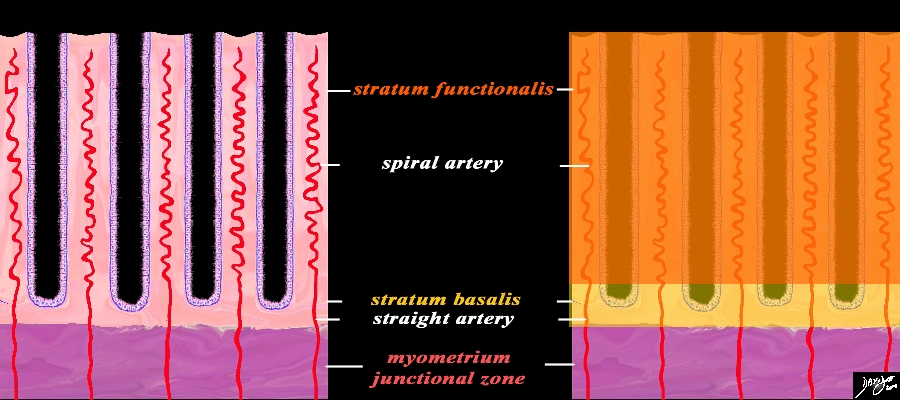
The magnifies view of the spiral arteries demonstrates its relationship to the stratum functionalis (deep orange). The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries. The spiral arteries undergo vasoconstriction at the time of the menses, resulting in ischemia of the stratum functionalis and subsequent shedding of this layer leaving stratum basalis intact.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.33b02.8s
|
Hysterosalpingogram During Menstruation |
|
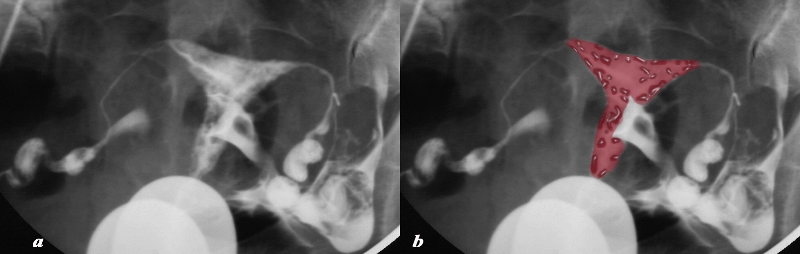
This patient presents with infertility. The hysterosalpingogram in the frontal view reveals normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The Fallopian tubes are patent.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 28208c02.8s
|
Menstruation
Ultrasound in Sagittal Projection |
|
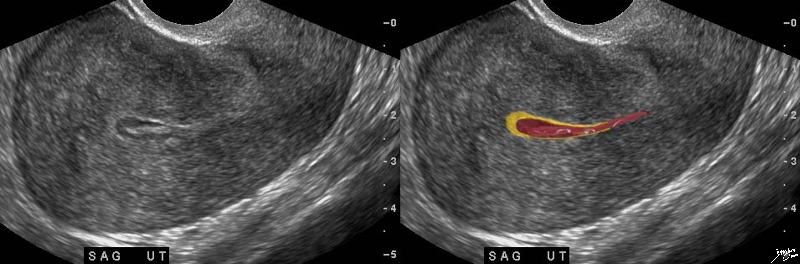
This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83112c.8s
|
Menstruation – CT scan
|
|
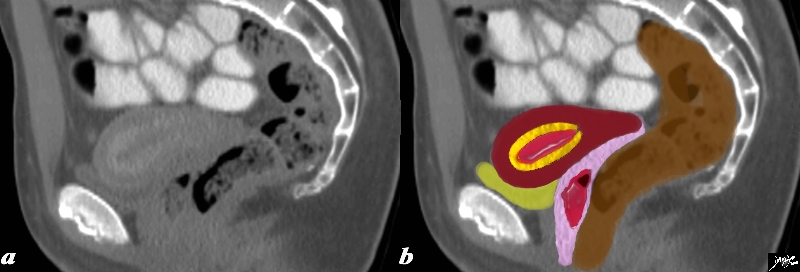
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity presumably filled with blood (red) surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow) A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough. (red). The bladder (yellow) is empty, and the rectum is brown and lies posterior.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 47664b02c03.8s
|
Histological Correlation
|
Functional Layer (Stratum Functionalis) Basal Layer (Stratum Basalis) and the Arteries
Premenstrual Phase |
|
A closer view of the endometrium as seen in the premenstrual phase exemplified by the characteristic spiral (helical) arteries running in the stroma (pink) between the simple tubular test tube shaped glands (purple) The spiral arteries supply the functional layer (stratum functionalis deep orange) and the straight arteries supply the basal layer (stratum basalis- light orange). Beneath the basal layer is the myometrium- Subendometrial smooth muscle or junctional zone (dark pink).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.9s
|
|
Distribution of the Arterial Supply Histologic Level |
|
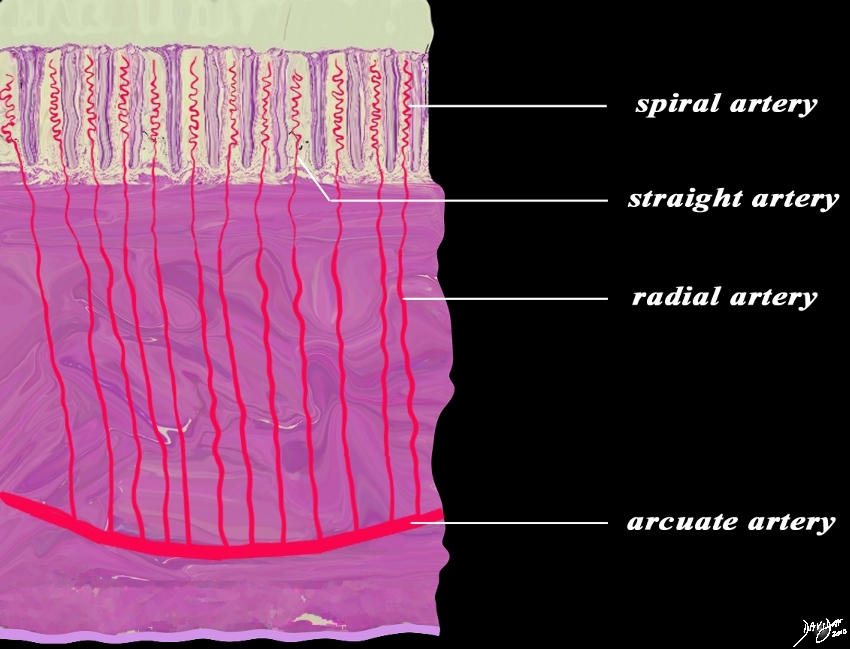
This diagram exemplifies the position the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis, the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 12047e04b04L02.8s
|
Cyclical Changes of the Endometrium
The three major phases of the cycle that manifest in the endometrium are the proliferative (follicular), secretory (luteal), and menstrual phases.
|
Premenstrual (left) and Active Menstruation (right) |
|
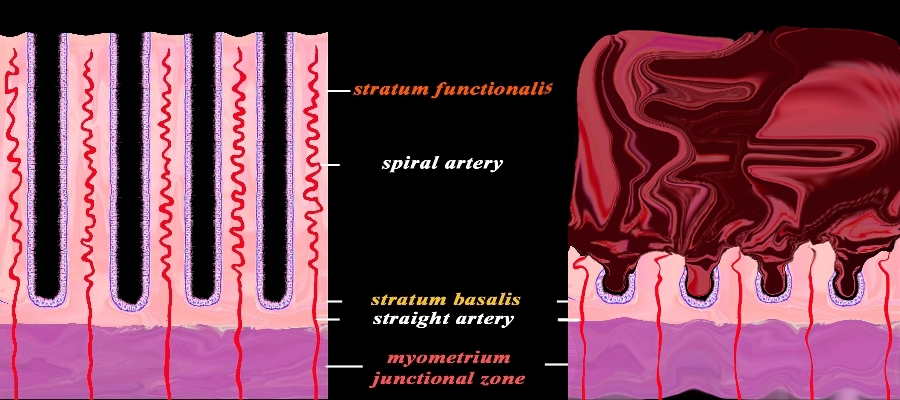
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the staright arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.92s
|
|
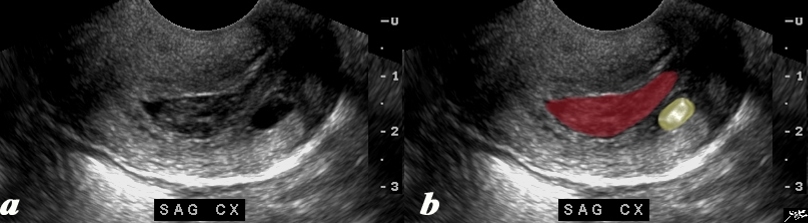
Cervical Canal distended with the Sloughed Functional Layer of Endometrium |
|
The transvaginal ultrasound of the cervix in sagittal view reveals a cervical canal filled and distended with the heterogeneous products of the shedded endometrium (maroon). A Nabothian syst (yellow) is of incidental note.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 85283c01.8s
|

Tampon in Vagina |
|
This 37 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Courtesy Ashley Davidoff MD Copyright 2009 all rights reserved 83626bc01.8s
|
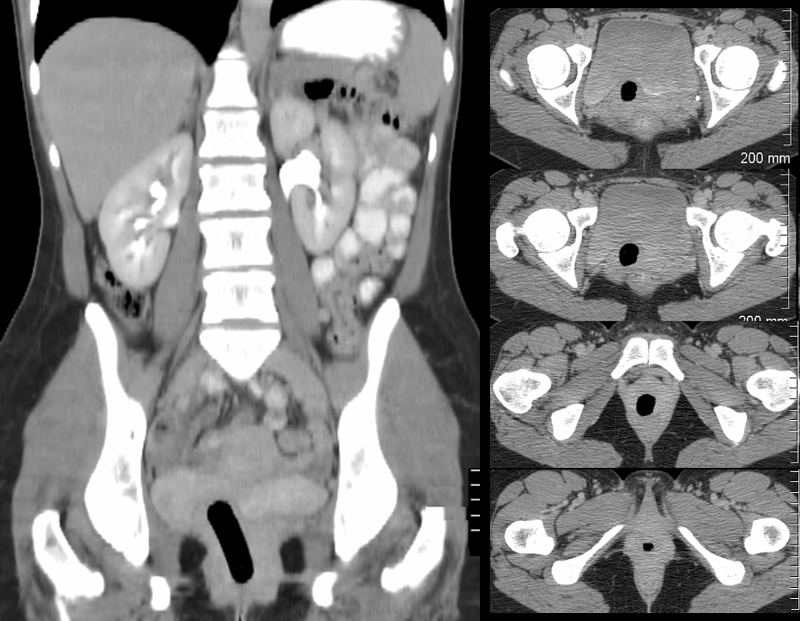
CT scan Showing A Tampon in the Vagina |
|
This 42 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CTscan in coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 97187c.8s
|
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
CT scan Showing A Tampon in the Vagina
This 42 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CTscan in coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 97187c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
CT scan Showing A Tampon in the Vagina
This 42 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CTscan in coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 97187c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 42 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CTscan in coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 97187c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 42 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients right. The reformatted CTscan in coronal section shows an air filled tubular structure in the pelvis representing an air filled tampon in the vagina. The axial images (right) show the tampon as a black circle behind the bladder from its high point behind the bladder to its inferior aspect in the perineum representing the position of the vagina.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 97187c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
CT scan Showing A Tampon in the Vagina
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
CT scan Showing A Tampon in the Vagina
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Tampon in Vagina
This 37 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Courtesy Ashley Davidoff MD Copyright 2009 all rights reserved 83626bc01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Tampon in Vagina
This 37 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Courtesy Ashley Davidoff MD Copyright 2009 all rights reserved 83626bc01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 37 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Courtesy Ashley Davidoff MD Copyright 2009 all rights reserved 83626bc01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 37 year old female is actively menstruating and the air filled tampon is seen as a tubular structure in the pelvis directed to the patients left. It is overlaid in green in image b.
Courtesy Ashley Davidoff MD Copyright 2009 all rights reserved 83626bc01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Tampon in Vagina
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Tampon in Vagina
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cervical Canal distended with the Sloughed Functional Layer of Endometrium
The transvaginal ultrasound of the cervix in sagittal view reveals a cervical canal filled and distended with the heterogeneous products of the shedded endometrium (maroon). A Nabothian syst (yellow) is of incidental note.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 85283c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cervical Canal distended with the Sloughed Functional Layer of Endometrium
The transvaginal ultrasound of the cervix in sagittal view reveals a cervical canal filled and distended with the heterogeneous products of the shedded endometrium (maroon). A Nabothian syst (yellow) is of incidental note.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 85283c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The transvaginal ultrasound of the cervix in sagittal view reveals a cervical canal filled and distended with the heterogeneous products of the shedded endometrium (maroon). A Nabothian syst (yellow) is of incidental note.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 85283c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The transvaginal ultrasound of the cervix in sagittal view reveals a cervical canal filled and distended with the heterogeneous products of the shedded endometrium (maroon). A Nabothian syst (yellow) is of incidental note.
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 85283c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cervical Canal distended with the Sloughed Functional Layer of Endometrium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cervical Canal distended with the Sloughed Functional Layer of Endometrium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Premenstrual (left) and Active Menstruation (right)
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the staright arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.92s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Premenstrual (left) and Active Menstruation (right)
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the staright arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.92s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the staright arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.92s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The diagram reflects the premenstrual endometrium (left) and the post menstrual endometrium right, revealing the necrosis of the functional layer with sloughing and hemorrhage. The basal layer with the staright arteries and a small portion of the spiral artery remains intact. The hemorrhage is controlled by spasm of the arteries and contraction of the myometrium.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.92s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Premenstrual (left) and Active Menstruation (right)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Premenstrual (left) and Active Menstruation (right)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Distribution of the Arterial Supply Histologic Level
This diagram exemplifies the position the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis, the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 12047e04b04L02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Distribution of the Arterial Supply Histologic Level
This diagram exemplifies the position the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis, the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 12047e04b04L02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This diagram exemplifies the position the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis, the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 12047e04b04L02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This diagram exemplifies the position the arteries in the epithelial and muscular layers. The spiral arteries run in the stratum functionalis, the straight arteries run in the stratum basalis, while the radial arteries and the arcuate arteries run in the muscularis.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 12047e04b04L02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Distribution of the Arterial Supply Histologic Level
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Distribution of the Arterial Supply Histologic Level
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Functional Layer (Stratum Functionalis) Basal Layer (Stratum Basalis) and the Arteries
Premenstrual Phase
A closer view of the endometrium as seen in the premenstrual phase exemplified by the characteristic spiral (helical) arteries running in the stroma (pink) between the simple tubular test tube shaped glands (purple) The spiral arteries supply the functional layer (stratum functionalis deep orange) and the straight arteries supply the basal layer (stratum basalis- light orange). Beneath the basal layer is the myometrium- Subendometrial smooth muscle or junctional zone (dark pink).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.9s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Functional Layer (Stratum Functionalis) Basal Layer (Stratum Basalis) and the Arteries
Premenstrual Phase
A closer view of the endometrium as seen in the premenstrual phase exemplified by the characteristic spiral (helical) arteries running in the stroma (pink) between the simple tubular test tube shaped glands (purple) The spiral arteries supply the functional layer (stratum functionalis deep orange) and the straight arteries supply the basal layer (stratum basalis- light orange). Beneath the basal layer is the myometrium- Subendometrial smooth muscle or junctional zone (dark pink).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.9s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
A closer view of the endometrium as seen in the premenstrual phase exemplified by the characteristic spiral (helical) arteries running in the stroma (pink) between the simple tubular test tube shaped glands (purple) The spiral arteries supply the functional layer (stratum functionalis deep orange) and the straight arteries supply the basal layer (stratum basalis- light orange). Beneath the basal layer is the myometrium- Subendometrial smooth muscle or junctional zone (dark pink).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.9s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
A closer view of the endometrium as seen in the premenstrual phase exemplified by the characteristic spiral (helical) arteries running in the stroma (pink) between the simple tubular test tube shaped glands (purple) The spiral arteries supply the functional layer (stratum functionalis deep orange) and the straight arteries supply the basal layer (stratum basalis- light orange). Beneath the basal layer is the myometrium- Subendometrial smooth muscle or junctional zone (dark pink).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 32347f08cL.9s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Functional Layer (Stratum Functionalis) Basal Layer (Stratum Basalis) and the Arteries
Premenstrual Phase
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Functional Layer (Stratum Functionalis) Basal Layer (Stratum Basalis) and the Arteries
Premenstrual Phase
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Menstruation – CT scan
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity presumably filled with blood (red) surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow) A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough. (red). The bladder (yellow) is empty, and the rectum is brown and lies posterior.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 47664b02c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Menstruation – CT scan
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity presumably filled with blood (red) surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow) A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough. (red). The bladder (yellow) is empty, and the rectum is brown and lies posterior.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 47664b02c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity presumably filled with blood (red) surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow) A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough. (red). The bladder (yellow) is empty, and the rectum is brown and lies posterior.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 47664b02c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This adult patient presents with pain during menstruation. The CT in the sagittal plane reveals a hypodense endometrial cavity presumably filled with blood (red) surrounded by a hyperemic wall that likely represents the stratum basalis (basal layer ? yellow) A surrounding hypodense layer and then a relatively hyperdense outside layer are thought to represent inner and outer myocardium. The vagina (pink) contains some complex tissue with air bubbles representing blood clots and endometrial slough. (red). The bladder (yellow) is empty, and the rectum is brown and lies posterior.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 47664b02c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Menstruation – CT scan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Menstruation – CT scan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Menstruation
Ultrasound in Sagittal Projection
This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83112c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Menstruation
Ultrasound in Sagittal Projection
This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83112c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83112c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This adult patient presents with pain during menstruation. The transvaginal ultrasound in the sagittal plane reveals a slightly thickened and heterogeneous uterus with a sloughed endometrium (functional layer) appearing as the echogenic material within the endometrial cavity (brighter red). The hypoechoic dark regions are overlaid in a darker red reflecting blood in the cavity. These are characteristic findings of menstrual products within the endometrial cavity. The remaining stratum basalis is overlaid in orange. The junctional layer of the myometrium is not evident.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83112c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Menstruation
Ultrasound in Sagittal Projection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Menstruation
Ultrasound in Sagittal Projection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hysterosalpingogram During Menstruation
This patient presents with infertility. The hysterosalpingogram in the frontal view reveals normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The Fallopian tubes are patent.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 28208c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hysterosalpingogram During Menstruation
This patient presents with infertility. The hysterosalpingogram in the frontal view reveals normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The Fallopian tubes are patent.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 28208c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This patient presents with infertility. The hysterosalpingogram in the frontal view reveals normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The Fallopian tubes are patent.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 28208c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This patient presents with infertility. The hysterosalpingogram in the frontal view reveals normal sized endometrial cavity filled with sloughed endometrium (dark maroon filling defects in b). The contrast has been overlaid in a lighter maroon to indicate blood. These are characteristic findings of menstrual products within the endometrial cavity. The Fallopian tubes are patent.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 28208c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hysterosalpingogram During Menstruation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hysterosalpingogram During Menstruation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Spiral Arteries and the Stratum Functionalis
The magnifies view of the spiral arteries demonstrates its relationship to the stratum functionalis (deep orange). The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries. The spiral arteries undergo vasoconstriction at the time of the menses, resulting in ischemia of the stratum functionalis and subsequent shedding of this layer leaving stratum basalis intact.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.33b02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Spiral Arteries and the Stratum Functionalis
The magnifies view of the spiral arteries demonstrates its relationship to the stratum functionalis (deep orange). The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries. The spiral arteries undergo vasoconstriction at the time of the menses, resulting in ischemia of the stratum functionalis and subsequent shedding of this layer leaving stratum basalis intact.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.33b02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The magnifies view of the spiral arteries demonstrates its relationship to the stratum functionalis (deep orange). The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries. The spiral arteries undergo vasoconstriction at the time of the menses, resulting in ischemia of the stratum functionalis and subsequent shedding of this layer leaving stratum basalis intact.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.33b02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The magnifies view of the spiral arteries demonstrates its relationship to the stratum functionalis (deep orange). The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries. The spiral arteries undergo vasoconstriction at the time of the menses, resulting in ischemia of the stratum functionalis and subsequent shedding of this layer leaving stratum basalis intact.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.33b02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Spiral Arteries and the Stratum Functionalis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Spiral Arteries and the Stratum Functionalis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Spiral Arteries Staratum Functionalis and Menstruation
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. (a) The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon). (b) In the second series of images (c,d) the blood supply of the uterus is exemplified to demonstrate the branches that lead to the spiral arteries which undergo vasoconstriction at the time of the menses resulting in ischemia of the functionalis and subsequent shedding . The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.2kc07L.9s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Spiral Arteries Staratum Functionalis and Menstruation
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. (a) The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon). (b) In the second series of images (c,d) the blood supply of the uterus is exemplified to demonstrate the branches that lead to the spiral arteries which undergo vasoconstriction at the time of the menses resulting in ischemia of the functionalis and subsequent shedding . The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.2kc07L.9s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. (a) The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon). (b) In the second series of images (c,d) the blood supply of the uterus is exemplified to demonstrate the branches that lead to the spiral arteries which undergo vasoconstriction at the time of the menses resulting in ischemia of the functionalis and subsequent shedding . The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.2kc07L.9s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. (a) The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon). (b) In the second series of images (c,d) the blood supply of the uterus is exemplified to demonstrate the branches that lead to the spiral arteries which undergo vasoconstriction at the time of the menses resulting in ischemia of the functionalis and subsequent shedding . The uterine arteries give rise to the arcuate arteries which in turn give rise to the radial arteries, straight arteries and finally the spiral arteries.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540.2kc07L.9s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Spiral Arteries Staratum Functionalis and Menstruation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Spiral Arteries Staratum Functionalis and Menstruation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
The Layers in the Premenstrual Uterus
Stratum Basalis and Stratum Functionalis are Not Distinguished by this US and appear as One LAyer
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540cc06.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The Layers in the Premenstrual Uterus
Stratum Basalis and Stratum Functionalis are Not Distinguished by this US and appear as One LAyer
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540cc06.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540cc06.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
In this 26 year premenstrual female a transvaginal ultrasound reveals a normal transverse view of the uterus with characteristic premenstrual appearance. The stripe is homogeneously echogenic and thick but also shows a hypoechoic halo of the junctional zone or inner myometrium. (salmon) The homogeneous stripe is made up from two histological layers (not distinguished by this ultrasound)? the inner stratum functionalis (deep orange) that will shed once the spiral arteries vasoconstrict, and the outer stratum basalis (deep yellow) that will not shed, and will be the basis for regenerating the endometrium in the next cycle. The next layer as stated above is the compact myometrium – the junctional zone (aka inner myometrium) , and is followed by the thicker outer myometrium (maroon).
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84540cc06.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The Layers in the Premenstrual Uterus
Stratum Basalis and Stratum Functionalis are Not Distinguished by this US and appear as One LAyer
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The Layers in the Premenstrual Uterus
Stratum Basalis and Stratum Functionalis are Not Distinguished by this US and appear as One LAyer
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Premenstrual Endometrium
End of Secretory Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, about 4 weeks after menstruation, and just prior to the next menstrauation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 46318c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Premenstrual Endometrium
End of Secretory Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, about 4 weeks after menstruation, and just prior to the next menstrauation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 46318c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, about 4 weeks after menstruation, and just prior to the next menstrauation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 46318c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, about 4 weeks after menstruation, and just prior to the next menstrauation when the endometrium is overripe. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the hyperechoic, homogeneous, thick endometrium characteristic of the secretory phase. It is during this time that progesterone is the dominant hormonal influence and estrogen influence is minimal. The endometrium in this case measures 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 46318c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Premenstrual Endometrium
End of Secretory Phase
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Premenstrual Endometrium
End of Secretory Phase
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Trilaminar Appearance – Midcycle Preovulation
End of Proliferative Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, 2 weeks after menstruation, and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This pahse is also called the follicular phase, or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe”, and conversely, its presence is seen before progesterone is produced. If present with a 9mm+ diameter, it reflects an ideal potential lining for fertilization.. In this case it measured 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83835c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Trilaminar Appearance – Midcycle Preovulation
End of Proliferative Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, 2 weeks after menstruation, and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This pahse is also called the follicular phase, or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe”, and conversely, its presence is seen before progesterone is produced. If present with a 9mm+ diameter, it reflects an ideal potential lining for fertilization.. In this case it measured 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83835c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, 2 weeks after menstruation, and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This pahse is also called the follicular phase, or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe”, and conversely, its presence is seen before progesterone is produced. If present with a 9mm+ diameter, it reflects an ideal potential lining for fertilization.. In this case it measured 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83835c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, 2 weeks after menstruation, and just prior to ovulation. It demonstrates that the uterus and more specifically the endometrium is more complex than just a simple columnar epithelium. This is an example of the trilaminar appearance of the endometrium and is characteristic of the appearance of the endometrium in the preovulatory phase. This pahse is also called the follicular phase, or proliferative phase. It is during this time that estrogen is the dominant hormonal influence. The appearance is also known as a “triple stripe”, and conversely, its presence is seen before progesterone is produced. If present with a 9mm+ diameter, it reflects an ideal potential lining for fertilization.. In this case it measured 1.2cms.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 83835c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Trilaminar Appearance – Midcycle Preovulation
End of Proliferative Phase
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Trilaminar Appearance – Midcycle Preovulation
End of Proliferative Phase
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
First Week Post Menstruation
Early Proliferative Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, in the first week after menstruation after menstruation, and just prior to the next menstruation after the endometrium has been shed. It demonstrates that the endometrium becomes a single echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (tan). This layer is more compacted, and relatively hypovascular. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has fallen. The endometrium in this case measures about 3mms
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84698c02b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
First Week Post Menstruation
Early Proliferative Phase
The normal sagittal view of the uterus is a transvaginal ultrasound, in the first week after menstruation after menstruation, and just prior to the next menstruation after the endometrium has been shed. It demonstrates that the endometrium becomes a single echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (tan). This layer is more compacted, and relatively hypovascular. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has fallen. The endometrium in this case measures about 3mms
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84698c02b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, in the first week after menstruation after menstruation, and just prior to the next menstruation after the endometrium has been shed. It demonstrates that the endometrium becomes a single echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (tan). This layer is more compacted, and relatively hypovascular. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has fallen. The endometrium in this case measures about 3mms
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84698c02b.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The normal sagittal view of the uterus is a transvaginal ultrasound, in the first week after menstruation after menstruation, and just prior to the next menstruation after the endometrium has been shed. It demonstrates that the endometrium becomes a single echogenic line consisting of opposing walls (orange) and is surrounded by a subendometrial halo of the junctional zone (tan). This layer is more compacted, and relatively hypovascular. This image is typical of the early proliferative phase. It is during this time that estrogen starts to rise and progesterone has fallen. The endometrium in this case measures about 3mms
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 84698c02b.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
First Week Post Menstruation
Early Proliferative Phase
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
First Week Post Menstruation
Early Proliferative Phase
)
