The Common Vein Copyright 2008
Ovarian Cysts
Ovarian cysts (follicles) are normal evolutions of the menstrual cycle but in certain instances the cyst physiology is altered for unknown reasons, causing the cyst to enlarge unusually, rupture in a different manner, or become hemorrhagic, resulting in a pain syndrome.
A variety of situations manifest structurally including;
Follicular rupture – mittelschmerz
Enlargement of the follicle without rupture
Hemorrhage into the follicle/cyst without rupture
Hemorrhage into the follicle/cyst with rupture
Hemorrhage into an endometrioma simulating hemorrhage into a follicle usually without rupture
The common result is a pain syndrome that commonly occurs in midcycle.
Physiologically, during each menstrual cycle, a normally functioning ovary produces multiple cysts called graafian follicles. During the middle of the cycle, one cyst dominates and releases an egg. The follicle then becomes the corpus luteum, which can mature to measure up to 2 cm. If fertilization does not occur, the corpus luteum fibroses and is resorbed. If fertilization does occur, the corpus luteum matures and enlarges initially, but later shrinks during pregnancy. Ovarian cysts can be either follicular or luteal, and may respond to gonadotropins (including FSH).
Clinically the pain is different from mittelschmerz in that it may be more severe, prolonged, or with a different character. Sometimes the pain can simulate peritonitis. Most importantly from a diagnostic standpoint, is that a mass is usually felt on clinical examination.
The diagnosis is confirmed by ultrasound which usually shows a cystic mass in the adnexa. The cyst is either larger than the usual follicle, contains hemorrhage, or hemorrhage and large amounts of fluid are noted free in the pelvic cavity. When the patient presents with peritonism, a CTscan is usually indicated and in the case of a ruptured cyst, induration of the greater omentum or proximity of the bleed to the anterior peritoneum is recognized together with the hemorrhagic cyst. When an ovarian cyst ruptures, there is usually minimal blood loss.
Treatment depends on several factors. In most patients, the treatment is conservative with pain management being central to the care. Surgery may be indicated if the cyst does not go away after several periods or is enlarging. In a post menopausal woman, when complex cysts are identified cyclical disease is not a consideration and malignant disease must be suspected.
Add hemorrhagic cyst of the ovary have a fishnet appearance
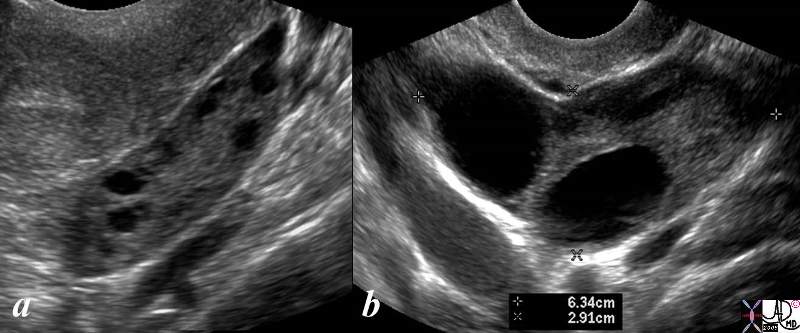
Normal (a) and Large Unruptured Follicles (b)
|
| The ultrasound shows a normal left ovary with small Graaffian follicles (a) and an enlarged ovary with two unruptured simple cysts (b) The latter study is from is from a 46 year female who presents with pelvic discomfort. The transvaginal ultrasound (b) shows a large 6cms ovary that contains two cysts each about 2cms in size.. The ovary is about twice to 3 times normal in size and the distension presumably causes the discomfort. The cysts are simple in nature without hemorrhage.
ovary pain cysts discomfort nrmal variant enlarged normal follicles USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD 83269c.8s |
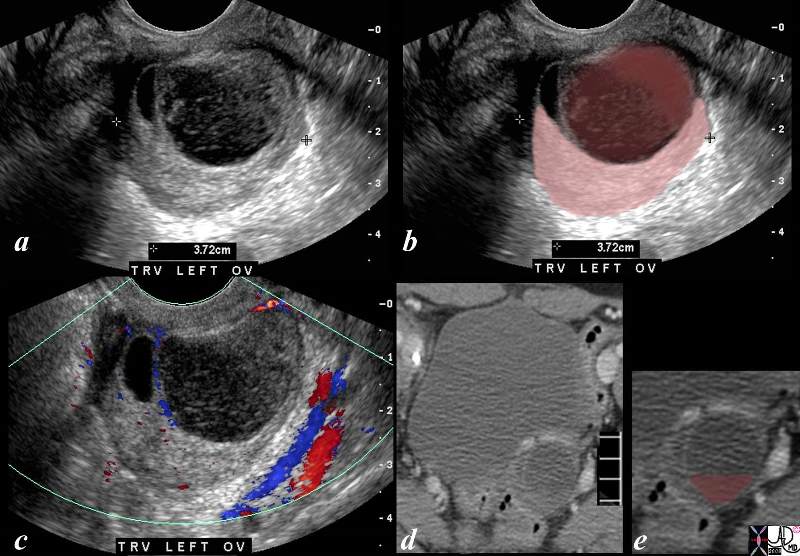
Hemorrhage into a Cyst with Clot Formation
|
| The ultrasound (a,b,c) and CTscan (d,e) are from a 39year old female with midcycle pain and show linear stranding and soft tissue changes into a large cyst in the left adnexa (a and b), with the hemorrhage outlined in maroon in b and displaced crescentic ovary in pink. The hemorrhage consists of soft tissue components (dark maroon in b) and the lighter maroon overlies the fibrinous and linear component of the clot that is better visualized in a. The doppler study in c, shows no color in the cyst implying that it is a non vascular structure. These findings are most characteristic of a cyst that has hemorrhaged into the cyst but without rupture of the cyst. The sudden distension of the cyst incites the pressure receptors and accounts for the pain.
The CTscan limoited to the bladder and left adnexa in d, shows a rounded complex lesion in the left adnexa with a fluid fluid level overlaid in maroon in e. This reflects sedimented red cells that were free to fall to the dependant portion of the hemorrhagic cyst.
ovary cyst hemorrhage clot fibrin pain midcycle USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 83279c02.8s |
83268c02.8c |
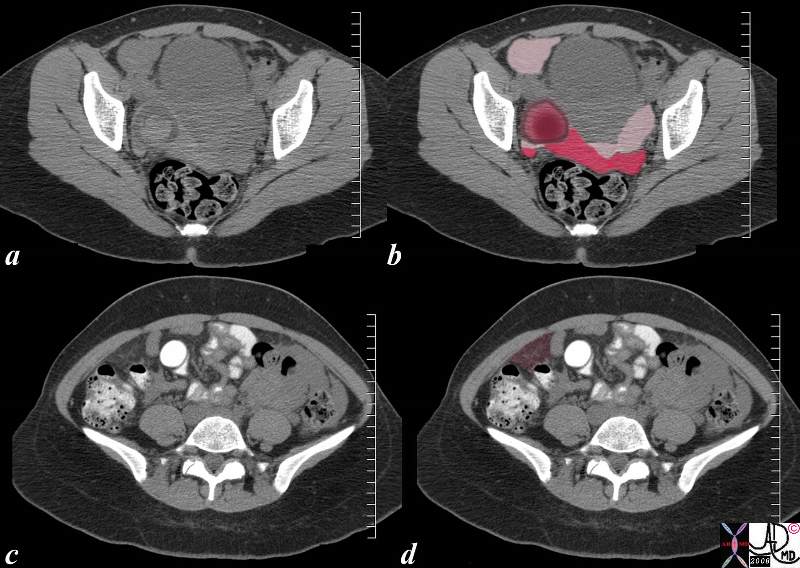
| 26 year old female presents with acute midcycle right lower quadrant pain without a fever, associated with peritonism in the right lower quadrant. Differential diagnosis included appendicitis, ruptured cyst, torsion, endometrioma and ectopic pregnancy, but her HCG was normal.
The CTscan shows acute hemorrhage in a cyst int the right adnexa consistent with a hemorrhagic and ruptured follicle, (maroon nodule with a pink circle in b), but also shows a large amount of blood and fluid, some accumulating in the right lower quadrant, (light pink anteriorly on right in b) some in the cul de sac (bright red sediment, and light pink supernatant in b) and some in the greater omentum on the right side (maroon in d). It is the latter component that incites the somatic nocicptors of the peritoneum to simulate peritonitis.
The patient was treated conservatively and improved over the next 24-48 hours.
pain ovary mittelschmerz hemorrhage rupture right lower quadrant pain RLQ peritonism peritonitis CTscan Courtesy Ashley Davidoff MD copyright 2008 83268c02.8c |
 2 2
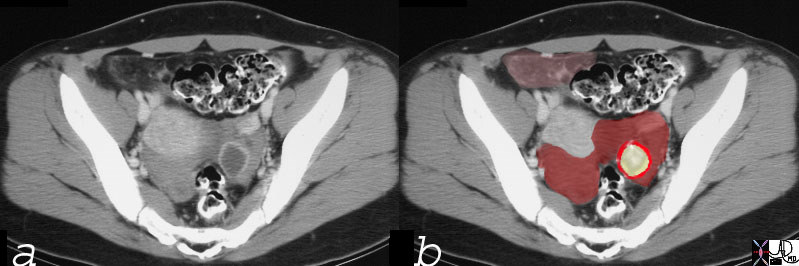
Left Sided Ruptured Hemorrhagic Cyst with Free Blood in the Pelvis and Bleeding onto the Greater Omentum RLQ (pink)
|
|
This CT scan is that of a 27 year old female who presented with acute lower pelvic pain in mid cycle. The findings of free blood in the pelvis (maroon) the cyst (yellow) with an enhancing rim (bright red) and spillage of blood onto the greater omentum (pink let anterior) are consistent with a ruptured hemorrhagic cyst . The intense ring around the cyst suggests that a corpus luteum cyst has formed already.
24480c01 27 year old female presented with lower abdominal pain pelvic pain ovary fx cyst cul de sac blood free blood hyperdense corpus luteum cyst greater ometum congested fx enhancing dx hemorhagic ovarian cyst CT scan C- CTscan Courtesy Ashley DAvidoff MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
2
Left Sided Ruptured Hemorrhagic Cyst with Free Blood in the Pelvis and Bleeding onto the Greater Omentum RLQ (pink)
This CT scan is that of a 27 year old female who presented with acute lower pelvic pain in mid cycle. The findings of free blood in the pelvis (maroon) the cyst (yellow) with an enhancing rim (bright red) and spillage of blood onto the greater omentum (pink let anterior) are consistent with a ruptured hemorrhagic cyst . The intense ring around the cyst suggests that a corpus luteum cyst has formed already.
24480c01 27 year old female presented with lower abdominal pain pelvic pain ovary fx cyst cul de sac blood free blood hyperdense corpus luteum cyst greater ometum congested fx enhancing dx hemorhagic ovarian cyst CT scan C- CTscan Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
2
Left Sided Ruptured Hemorrhagic Cyst with Free Blood in the Pelvis and Bleeding onto the Greater Omentum RLQ (pink)
This CT scan is that of a 27 year old female who presented with acute lower pelvic pain in mid cycle. The findings of free blood in the pelvis (maroon) the cyst (yellow) with an enhancing rim (bright red) and spillage of blood onto the greater omentum (pink let anterior) are consistent with a ruptured hemorrhagic cyst . The intense ring around the cyst suggests that a corpus luteum cyst has formed already.
24480c01 27 year old female presented with lower abdominal pain pelvic pain ovary fx cyst cul de sac blood free blood hyperdense corpus luteum cyst greater ometum congested fx enhancing dx hemorhagic ovarian cyst CT scan C- CTscan Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This CT scan is that of a 27 year old female who presented with acute lower pelvic pain in mid cycle. The findings of free blood in the pelvis (maroon) the cyst (yellow) with an enhancing rim (bright red) and spillage of blood onto the greater omentum (pink let anterior) are consistent with a ruptured hemorrhagic cyst . The intense ring around the cyst suggests that a corpus luteum cyst has formed already.
24480c01 27 year old female presented with lower abdominal pain pelvic pain ovary fx cyst cul de sac blood free blood hyperdense corpus luteum cyst greater ometum congested fx enhancing dx hemorhagic ovarian cyst CT scan C- CTscan Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This CT scan is that of a 27 year old female who presented with acute lower pelvic pain in mid cycle. The findings of free blood in the pelvis (maroon) the cyst (yellow) with an enhancing rim (bright red) and spillage of blood onto the greater omentum (pink let anterior) are consistent with a ruptured hemorrhagic cyst . The intense ring around the cyst suggests that a corpus luteum cyst has formed already.
24480c01 27 year old female presented with lower abdominal pain pelvic pain ovary fx cyst cul de sac blood free blood hyperdense corpus luteum cyst greater ometum congested fx enhancing dx hemorhagic ovarian cyst CT scan C- CTscan Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 2
Left Sided Ruptured Hemorrhagic Cyst with Free Blood in the Pelvis and Bleeding onto the Greater Omentum RLQ (pink)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 2
Left Sided Ruptured Hemorrhagic Cyst with Free Blood in the Pelvis and Bleeding onto the Greater Omentum RLQ (pink)
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
83268c02.8c
26 year old female presents with acute midcycle right lower quadrant pain without a fever, associated with peritonism in the right lower quadrant. Differential diagnosis included appendicitis, ruptured cyst, torsion, endometrioma and ectopic pregnancy, but her HCG was normal.
The CTscan shows acute hemorrhage in a cyst int the right adnexa consistent with a hemorrhagic and ruptured follicle, (maroon nodule with a pink circle in b), but also shows a large amount of blood and fluid, some accumulating in the right lower quadrant, (light pink anteriorly on right in b) some in the cul de sac (bright red sediment, and light pink supernatant in b) and some in the greater omentum on the right side (maroon in d). It is the latter component that incites the somatic nocicptors of the peritoneum to simulate peritonitis.
The patient was treated conservatively and improved over the next 24-48 hours.
pain ovary mittelschmerz hemorrhage rupture right lower quadrant pain RLQ peritonism peritonitis CTscan Courtesy Ashley Davidoff MD copyright 2008 83268c02.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
83268c02.8c
26 year old female presents with acute midcycle right lower quadrant pain without a fever, associated with peritonism in the right lower quadrant. Differential diagnosis included appendicitis, ruptured cyst, torsion, endometrioma and ectopic pregnancy, but her HCG was normal.
The CTscan shows acute hemorrhage in a cyst int the right adnexa consistent with a hemorrhagic and ruptured follicle, (maroon nodule with a pink circle in b), but also shows a large amount of blood and fluid, some accumulating in the right lower quadrant, (light pink anteriorly on right in b) some in the cul de sac (bright red sediment, and light pink supernatant in b) and some in the greater omentum on the right side (maroon in d). It is the latter component that incites the somatic nocicptors of the peritoneum to simulate peritonitis.
The patient was treated conservatively and improved over the next 24-48 hours.
pain ovary mittelschmerz hemorrhage rupture right lower quadrant pain RLQ peritonism peritonitis CTscan Courtesy Ashley Davidoff MD copyright 2008 83268c02.8c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 26 year old female presents with acute midcycle right lower quadrant pain without a fever, associated with peritonism in the right lower quadrant. Differential diagnosis included appendicitis, ruptured cyst, torsion, endometrioma and ectopic pregnancy, but her HCG was normal.
The CTscan shows acute hemorrhage in a cyst int the right adnexa consistent with a hemorrhagic and ruptured follicle, (maroon nodule with a pink circle in b), but also shows a large amount of blood and fluid, some accumulating in the right lower quadrant, (light pink anteriorly on right in b) some in the cul de sac (bright red sediment, and light pink supernatant in b) and some in the greater omentum on the right side (maroon in d). It is the latter component that incites the somatic nocicptors of the peritoneum to simulate peritonitis.
The patient was treated conservatively and improved over the next 24-48 hours.
pain ovary mittelschmerz hemorrhage rupture right lower quadrant pain RLQ peritonism peritonitis CTscan Courtesy Ashley Davidoff MD copyright 2008 83268c02.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 26 year old female presents with acute midcycle right lower quadrant pain without a fever, associated with peritonism in the right lower quadrant. Differential diagnosis included appendicitis, ruptured cyst, torsion, endometrioma and ectopic pregnancy, but her HCG was normal.
The CTscan shows acute hemorrhage in a cyst int the right adnexa consistent with a hemorrhagic and ruptured follicle, (maroon nodule with a pink circle in b), but also shows a large amount of blood and fluid, some accumulating in the right lower quadrant, (light pink anteriorly on right in b) some in the cul de sac (bright red sediment, and light pink supernatant in b) and some in the greater omentum on the right side (maroon in d). It is the latter component that incites the somatic nocicptors of the peritoneum to simulate peritonitis.
The patient was treated conservatively and improved over the next 24-48 hours.
pain ovary mittelschmerz hemorrhage rupture right lower quadrant pain RLQ peritonism peritonitis CTscan Courtesy Ashley Davidoff MD copyright 2008 83268c02.8c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
83268c02.8c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
83268c02.8c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Hemorrhage into a Cyst with Clot Formation
The ultrasound (a,b,c) and CTscan (d,e) are from a 39year old female with midcycle pain and show linear stranding and soft tissue changes into a large cyst in the left adnexa (a and b), with the hemorrhage outlined in maroon in b and displaced crescentic ovary in pink. The hemorrhage consists of soft tissue components (dark maroon in b) and the lighter maroon overlies the fibrinous and linear component of the clot that is better visualized in a. The doppler study in c, shows no color in the cyst implying that it is a non vascular structure. These findings are most characteristic of a cyst that has hemorrhaged into the cyst but without rupture of the cyst. The sudden distension of the cyst incites the pressure receptors and accounts for the pain.
The CTscan limoited to the bladder and left adnexa in d, shows a rounded complex lesion in the left adnexa with a fluid fluid level overlaid in maroon in e. This reflects sedimented red cells that were free to fall to the dependant portion of the hemorrhagic cyst.
ovary cyst hemorrhage clot fibrin pain midcycle USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 83279c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Hemorrhage into a Cyst with Clot Formation
The ultrasound (a,b,c) and CTscan (d,e) are from a 39year old female with midcycle pain and show linear stranding and soft tissue changes into a large cyst in the left adnexa (a and b), with the hemorrhage outlined in maroon in b and displaced crescentic ovary in pink. The hemorrhage consists of soft tissue components (dark maroon in b) and the lighter maroon overlies the fibrinous and linear component of the clot that is better visualized in a. The doppler study in c, shows no color in the cyst implying that it is a non vascular structure. These findings are most characteristic of a cyst that has hemorrhaged into the cyst but without rupture of the cyst. The sudden distension of the cyst incites the pressure receptors and accounts for the pain.
The CTscan limoited to the bladder and left adnexa in d, shows a rounded complex lesion in the left adnexa with a fluid fluid level overlaid in maroon in e. This reflects sedimented red cells that were free to fall to the dependant portion of the hemorrhagic cyst.
ovary cyst hemorrhage clot fibrin pain midcycle USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 83279c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The ultrasound (a,b,c) and CTscan (d,e) are from a 39year old female with midcycle pain and show linear stranding and soft tissue changes into a large cyst in the left adnexa (a and b), with the hemorrhage outlined in maroon in b and displaced crescentic ovary in pink. The hemorrhage consists of soft tissue components (dark maroon in b) and the lighter maroon overlies the fibrinous and linear component of the clot that is better visualized in a. The doppler study in c, shows no color in the cyst implying that it is a non vascular structure. These findings are most characteristic of a cyst that has hemorrhaged into the cyst but without rupture of the cyst. The sudden distension of the cyst incites the pressure receptors and accounts for the pain.
The CTscan limoited to the bladder and left adnexa in d, shows a rounded complex lesion in the left adnexa with a fluid fluid level overlaid in maroon in e. This reflects sedimented red cells that were free to fall to the dependant portion of the hemorrhagic cyst.
ovary cyst hemorrhage clot fibrin pain midcycle USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 83279c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The ultrasound (a,b,c) and CTscan (d,e) are from a 39year old female with midcycle pain and show linear stranding and soft tissue changes into a large cyst in the left adnexa (a and b), with the hemorrhage outlined in maroon in b and displaced crescentic ovary in pink. The hemorrhage consists of soft tissue components (dark maroon in b) and the lighter maroon overlies the fibrinous and linear component of the clot that is better visualized in a. The doppler study in c, shows no color in the cyst implying that it is a non vascular structure. These findings are most characteristic of a cyst that has hemorrhaged into the cyst but without rupture of the cyst. The sudden distension of the cyst incites the pressure receptors and accounts for the pain.
The CTscan limoited to the bladder and left adnexa in d, shows a rounded complex lesion in the left adnexa with a fluid fluid level overlaid in maroon in e. This reflects sedimented red cells that were free to fall to the dependant portion of the hemorrhagic cyst.
ovary cyst hemorrhage clot fibrin pain midcycle USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 83279c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Hemorrhage into a Cyst with Clot Formation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Hemorrhage into a Cyst with Clot Formation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal (a) and Large Unruptured Follicles (b)
The ultrasound shows a normal left ovary with small Graaffian follicles (a) and an enlarged ovary with two unruptured simple cysts (b) The latter study is from is from a 46 year female who presents with pelvic discomfort. The transvaginal ultrasound (b) shows a large 6cms ovary that contains two cysts each about 2cms in size.. The ovary is about twice to 3 times normal in size and the distension presumably causes the discomfort. The cysts are simple in nature without hemorrhage.
ovary pain cysts discomfort nrmal variant enlarged normal follicles USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD 83269c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal (a) and Large Unruptured Follicles (b)
The ultrasound shows a normal left ovary with small Graaffian follicles (a) and an enlarged ovary with two unruptured simple cysts (b) The latter study is from is from a 46 year female who presents with pelvic discomfort. The transvaginal ultrasound (b) shows a large 6cms ovary that contains two cysts each about 2cms in size.. The ovary is about twice to 3 times normal in size and the distension presumably causes the discomfort. The cysts are simple in nature without hemorrhage.
ovary pain cysts discomfort nrmal variant enlarged normal follicles USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD 83269c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The ultrasound shows a normal left ovary with small Graaffian follicles (a) and an enlarged ovary with two unruptured simple cysts (b) The latter study is from is from a 46 year female who presents with pelvic discomfort. The transvaginal ultrasound (b) shows a large 6cms ovary that contains two cysts each about 2cms in size.. The ovary is about twice to 3 times normal in size and the distension presumably causes the discomfort. The cysts are simple in nature without hemorrhage.
ovary pain cysts discomfort nrmal variant enlarged normal follicles USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD 83269c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The ultrasound shows a normal left ovary with small Graaffian follicles (a) and an enlarged ovary with two unruptured simple cysts (b) The latter study is from is from a 46 year female who presents with pelvic discomfort. The transvaginal ultrasound (b) shows a large 6cms ovary that contains two cysts each about 2cms in size.. The ovary is about twice to 3 times normal in size and the distension presumably causes the discomfort. The cysts are simple in nature without hemorrhage.
ovary pain cysts discomfort nrmal variant enlarged normal follicles USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD 83269c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal (a) and Large Unruptured Follicles (b)
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal (a) and Large Unruptured Follicles (b)
)
