The Common Vein Copyright 2008
Alok Anand
Definition
Polyps in the gallbladder can be used to describe a number of types of tissue proliferation which may be inflammatory or neoplastic in nature
The characteristics and causes of polyps depend on their type:
Cholesterol polyps are yellow spots on the mucosal surface of the gallbladder. They are usually multiple and diffuse.
Adenomyomatosis represents thickenings of the epithelium and mucosa, and mucosal herniations called Rokitansky-Aschoff sinuses.
Inflammatory polyps are tissue on narrow, vascularized stalks that extend into the lumen of the gallbladder
Adenomas are focal proliferations of the epithelium and are considered premalignant.
Miscellaneous neoplasms are cancerous lesions of the gallbladder or varying histologic types.
Cholesterol polyps account for nearly half of all polyps, and along with adenomyomatosis collectively comprise the hyperplastic cholecystoses.
- Inflammatory polyps are caused by chronic inflammation, and contain granulation and fibrous tissue mixed with white cells.
- Adenomas are described as papillary, tubulopapillary or tubular, and are similar in structure to those in the rest of the GI tract.
Although most polyps are benign the adenomas may result in malignancy and particulalry when they are larger than 1cms. In certain cases, such as sclerosing cholangitis, this malignant potential may be even greater. For the rest of the benign polyps there is usually little clinical significance, although sloughing off of proliferative tissue may be a result in biliary obstruction.
Functionally there is normal bile synthesis and processing and the liver is not affected
Clinically polyps are generally found incidentally when evaluating biliary pain.
Diagnosis is usually by ultrasound, and if large enough may be seen by CT imaging.
Generally polyps are left untreated, however surgical removal of the gallbladder is performed when polyps grow to greater than 10 mm, when malignant potential is a reality. In suspicious cases, or with concomitant sclerosing cholangitis, more aggressive treatment of <10mm polyps may be indicated.
 Polyp Polyp |
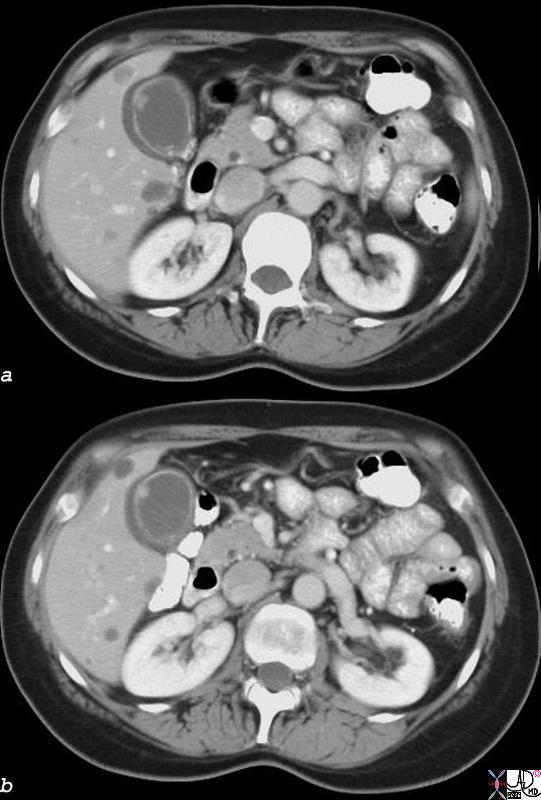
| 18333c02.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008 |
 Polyp Polyp |
| 47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD |
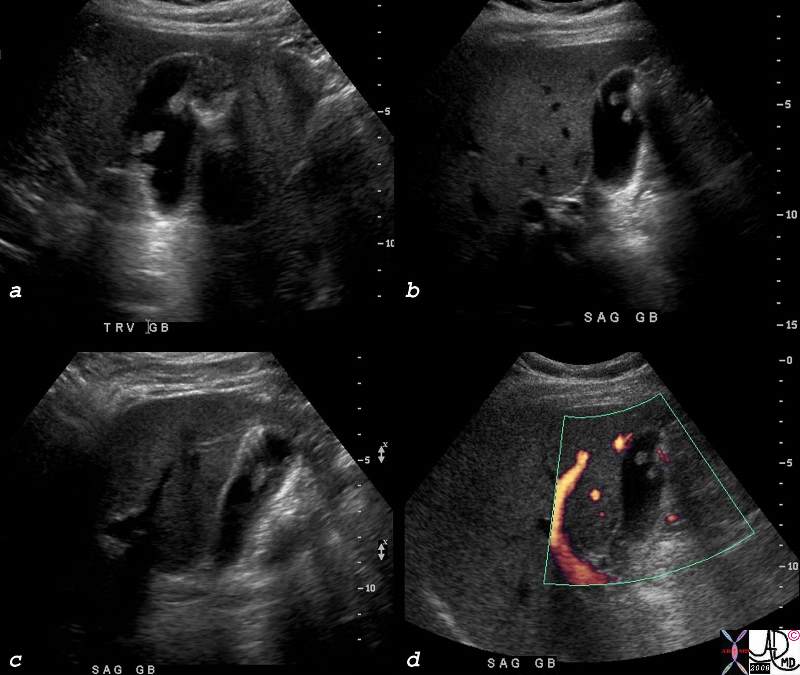 Large Polyps Large Polyps |
| 82195c01.8s 56M multiple polyps in the gallbladder gallbladder cholesterolosis or papillomatosis ring down artefact artifact hyperplastic cholecystoses USscan Courtesy Ashley DAvidoff MD copyright 2008 |
Links and References
Radiology 2022- Kamaya- SRU Mgmt of Incidental GB Polyps
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large Polyps
82195c01.8s 56M multiple polyps in the gallbladder gallbladder cholesterolosis or papillomatosis ring down artefact artifact hyperplastic cholecystoses USscan Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large Polyps
82195c01.8s 56M multiple polyps in the gallbladder gallbladder cholesterolosis or papillomatosis ring down artefact artifact hyperplastic cholecystoses USscan Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 82195c01.8s 56M multiple polyps in the gallbladder gallbladder cholesterolosis or papillomatosis ring down artefact artifact hyperplastic cholecystoses USscan Courtesy Ashley DAvidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82195c01.8s 56M multiple polyps in the gallbladder gallbladder cholesterolosis or papillomatosis ring down artefact artifact hyperplastic cholecystoses USscan Courtesy Ashley DAvidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Large Polyps
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Large Polyps
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Polyp
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Polyp
47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Polyp
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Polyp
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Polyp
18333c02.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Polyp
18333c02.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 18333c02.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 18333c02.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Polyp
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Polyp
)
