Cystic Duct of the Gallbladder
The Common Vein Copyright 2008
Definition
The cystic duct is the duct that connects the gallbladder to the bile duct. It is part of the biliary system and is characterized by its position and by its double spiral and serpiginous nature.
It consists of two parts. The proximal portion is called the spiral portion (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not truly known.. The distal part is straight usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end.
The structure of the cystic duct is quite unique, puzzling, variable and interesting. It is usually 2-4 cms long but can be be up to 10cms. It is usually 1-5mm wide. It is a tube with a course that proximally is usually tortuous or serpentine, much like the splenic artery. Therefore it is a tube with double spiral morphology. It has 4-10 internal spirals of Heister and its overall proximal course shows tortuosity. It lies relatively posteriorly at the medial end of the gallbladder in close association with the portal triad with its surrounding Glisson’s capsule. It also runs in close association with the cystic artery. The cystic duct is supplied by 2 to 4 minor branches called Calot?s arteries that originate just proximal to the origin of the anterior and posterior branches of the cystic artery.
The cystic duct usually enters the bile duct halfway between the porta hepatics and the ampulla, but it may enter the bile duct at the porta hepatis or low down near the ampulla. It most commonly enters the bile duct on its lateral (right) side, but can enter medially, posteriorly or anteriorly. As it enters it changes the name of the bile duct from the upstream common hepatic duct to the downstream common bile duct.
The function of the cystic duct is clearly to transport bile to and from the gallbladder and bile duct. Its spiral forms are structurally interesting but functionally a puzzle. The closest one come to is that the spiral valves of Heister create a resistance to flow that prevents overfilling and overdistension of the gracile bile ducts at the time of gallbladder contraction.
The most common diseases of the cystic duct are of a mechanical nature and are as a result of small stones getting stuck and impacted in the duct and resulting in obstruction of the gallbladder. When inflammation supercedes this event then acute cholecystitis occurs.
Treatment of cystic duct disease is usually surgical.
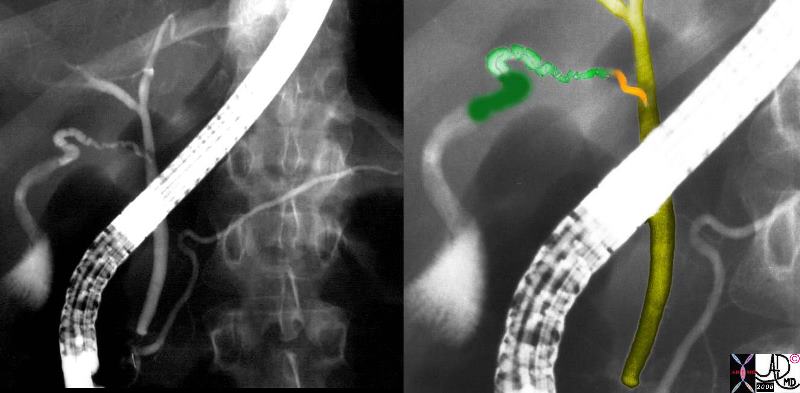
Cyctic Duct Joining the Bile Duct
|
| 29247c04.8s gallbladder parts normal anatomy neck cystic duct spiral portion spiral valves of Heister The proximal portion is called the spiral portion, (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not known.. The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. neck = dark green spiral portion = light green straight portion common hepatic duct light olive common bile duct = dark olive ERCP Courtesy Ashley Davidoff MD copyright 2008 |
Applied Biology
There are a variety of normal variants of the cystic duct including its length and insertion point into the bile duct. An important and well known variation is the long smooth portion of the duct that runs parallel to the bile duct and finally inserts, usually on its left side, at a variable distance from the ampulla.
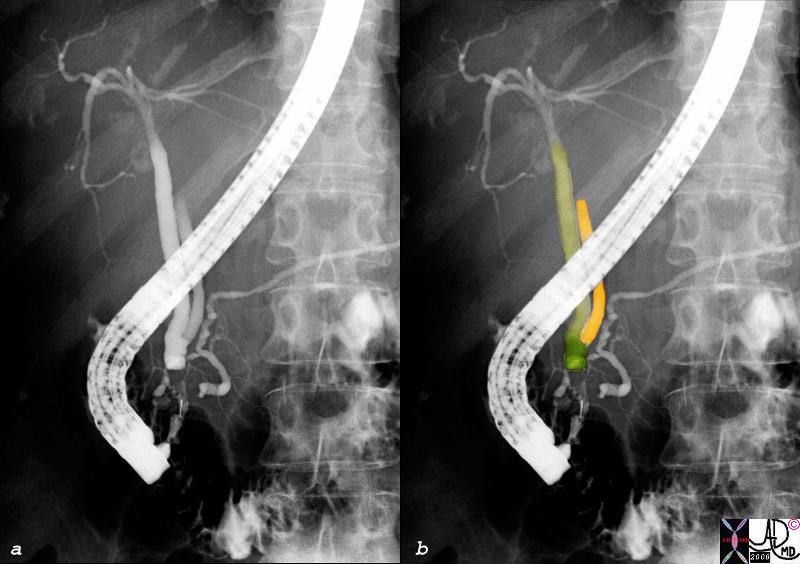
Distal Insertion of the Cystic Duct
|
| In this ERCP the straight portion of the cystic duct (orange) inserts into the medial aspect of the common hepatic duct (light olive) to form the common bile duct (dark olive) just proximal to the ampulla. This a variant of normal for the length of the cystic duct, its coparalely medial course, and its distal medial insertion. The result is also a long common hepatic duct and a short common bile duct.
39963c02.8s gallbladder parts normal anatomy cystic duct The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. straight portion = orange common hepatic duct = light olive yellow variant of length insertion position anatomy parts ERCP Courtesy Ashley Davidoff MD copyright 2008 |
The most common disease affecting the cystic duct is impaction of small stones. This results in obstruction and bile cannot get in nor out. The gallbladder becomes inflammed, acute cholecystitis manifests with exudation of fluid and the gallbladder becomes distended.

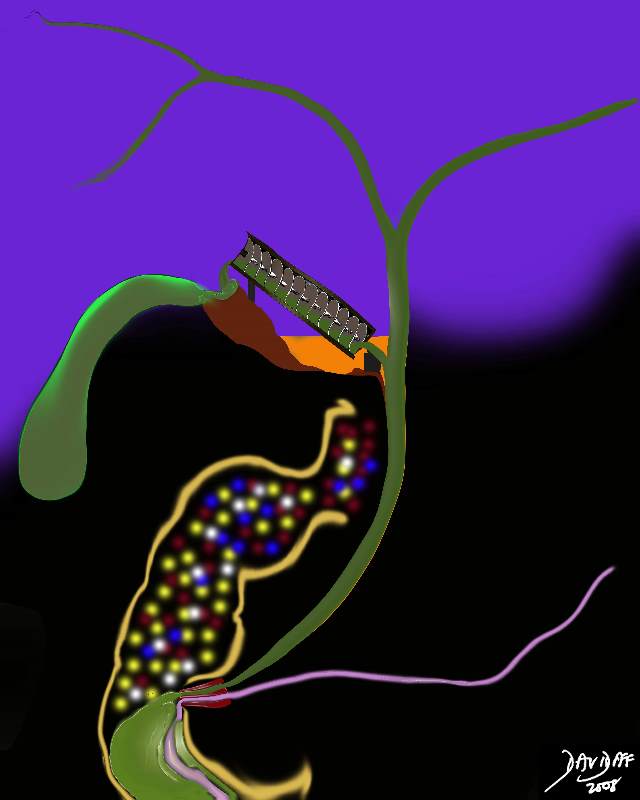
Stone Imapacted in the Cystic Duct
|
| The artistic rendition shows a smallstone impacted in the spiral valves of Heister, with inflammation of the wall, upstream distension due to exudation of fluid. The gallbladder enlarges becomes rotund, and the upstream cystic duct distends. new bile cannot enter and bile cannot leave the gallbladder.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008 |
The other relatively common disease that results in disease of the cystic duct is cancer of the head of the pancreas. This usually causes obstruction of the pancreatic duct, common bile duct, and by default the cystic duct and gallbladder as well.
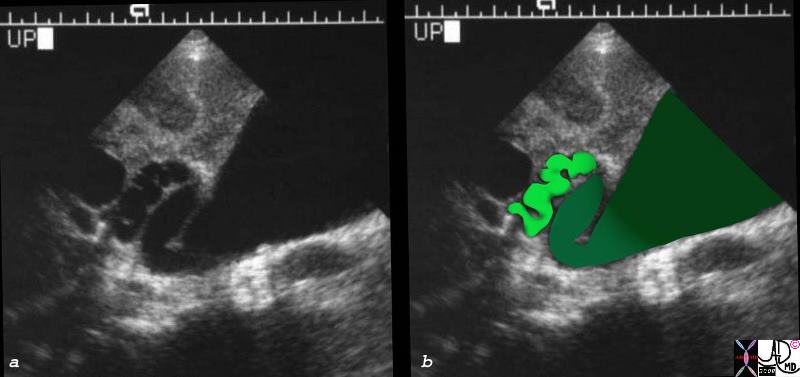
Dilated Cystic Duct Pancreatic Carcinoma
|
| The transverse section of the base of the gallbladder shows the distended body (darkest green), sinusoid neck of the gallbladder (intermediate green) connected to the similalrly distended spiral portion of the cystic duct (light green) in this patient with carcinoma of the head of the pancreas. The cystic duct is dilated and therefore visualized. The cystic duct is not normally visualized for a number of reasons. It is relatively small (1-2mm), lies deep in the porta hepatis surrounded by the echogenic Glissons capsule and other structures of the porta , and it is of itself echogenic because of the many valves which reflect echoes as well. All the echogenic structures prevent resolution of the small duct. Because the bile duct is obstructed by the pancreatic cancer, all the upstream components have become distended and the patient as a result becomes jaundiced.
04648c.8s patient with pancreatic carcinoma gallbladder dilated neck cystic duct valves of Heister dilated enlarged obstruction USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD |
The Variation in cystic duct anatomy is quite common. The standard relationship of cystic duct, extrahepatic bile duct and related arteries is present in only 33% of cases. However, a double cystic duct is extremely rare.
Accompanied by the cystic artery
runs downward back and to the left and usually joins the bile duct on its right side after travelleing parallel for a variable distance with it
Heister 1732
Heister (1732) reported his observation of spiraling folds in the lumen of the duct and described them as valves (http://64.233.169.104/search?q=cache:qDJJBSQ8OUkJ:www.maths.gla.ac.uk/~xl/Anatomy-06.pdf+What+functional+purpose+do+the+spiral+valves+of+heister+have%3F&hl=en&ct=clnk&cd=1&gl=us)
The spiral valves of Heister have been a puzzle for many years. We theorise that they have been ingeniously designed to hold and pass on the bile during this ascent against the forces of gravity, in much the same way that Archimedes design of the waterscrew helped the delivery of water from a low source to a high receptacle, also going against the force of gravity, and with the least energy expenditure.
 Archimedes Water Screw Archimedes Water Screw |
| The design of the water screw has been attributed to Archimedes from 3rd century BC though some designate the originator of the screw to be Nebuchadnezzar II of 7th century BC who purportedly used the screw to deliver water to the Hanging Gardens of Babylon. Water at a low level is scooped up into the spiral mechanism. As the screw rotates, the water advances upward and gets delivered to a higher level until it finally reaches its destination and is delivered to a repository.
has been 82656b15.8s Archimedes water screw elevation gravity screw delivery cystic duct spiral valves of Heister anatomy physiology function uploading Davidoff art copyright 2008
The image was modified from Wikipedia; detail of image: Archimedes’ screw. Public domain, from Chambers’s Encyclopedia (Philadelphia: J. B. Lippincott Company, 1875). Added to illustrate article :Archimedes. |
In the body there is no handle to turn the valves (screws ) of Heister. There are hydrostatic forces from below caused by the continued 24hour production of bile by the liver at about the rate of 1/2ccs per minute. (approximately 800ccs in 24 hours, = approximately 1/2ccs per minute)
The maximum secreting pressures of bile from the hepatocystes is approximately 30cms of water. The resting pressure of the sphincter of Oddi is 12-15cms of water, the opening pressure of the cystic duct is 8cms of water and the opening pressure of the gallbladder is 10cms of water. Thus when the sphincter is closed the lowest pressure is in the cystic duct and hence filling of the cystic duct occurs. (Clavien)
As the new drop of bile spills into the bile ducts it will cause a minute rise in pressure against the closed sphincter of Oddi. Flow in the system is directed toward the cystic duct offers the least resistance as described above. Bile will therefore fill the first valve which will push the bile upward to the second valve and so on. With this repeated many times, each valve is filled until the bile reaches the top of the ladder after which it will spill over like a waterfall into the neck, and then body, and finally into the fundus.
The sphincter of Oddi is composed of a ring of circular and longitudinal muscle at the distal end of the common bile duct which has a phasic resting pressure of about 13mmHg. It has a cyclical pattern during fasting that works in concordance with the intermittant myoelectric migratory complex of the intestinal tract (IMMC), as well as a pattern specific to the presence of CCK and the parasympathetic nerve supply.
The common bile duct unites with with the pancreatic duct to form a common channel called the ampulla of Vater which empties into the duodenum at the papilla which is seen as a small nipple in the middle of the descending duodenum.

Filling
|
| This diagram illustrates the concept of how the gallbladder receives bile via the relatively high lying (cranially positioned) cystic duct, using a stepwise ladder system of valves to deliver the dilute bile to the gallbladder without a pump. An Archimedes water screw in the position of the spiral valves is shown revealing the parallel mechanism of action. In the case of the spiral valves the driving force is a is a push from the bottom, rather than a pull from the top. The spirals are not as complete as the screws of the Archomedes device. Rather they are a series of sacs of small diameter that have membranous folds that spiral and prevent backflow. (we propose)
The bile produced during the day in the biliary system will cause a minimal rise in pressure 82656b20.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008 |
Valves of Heister and the Archimedes Waterscrew
|
| 82656b23.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008 |
References
Turner MA Fulcher AS The Cystic Duct: Normal Anatomy and Disease Processes Radiographics. 2001;21:3-22
Netter FH. The Ciba collection of medical illustrations Vol 111. Digestive system. Part III. Liver, biliary tract and pancreas. Summit, NJ: Ciba Pharmaceutical, 1957; 22-24.
Friedman AC, Sachs L. Embryology, anatomy, histology and radiologic anatomy. In: Friedman AC, eds. Radiology of the liver, biliary tract, pancreas and spleen. Baltimore, Md: Williams & Wilkins, 1987; 305-332.
Shaw MJ, Dorsher PJ, Vennes JA. Cystic duct anatomy: an endoscopic perspective. Am J Gastroenterol 1993; 88:2102-2106.[Medline]
Zeman RK, Burrell MI. Gallbladder and bile duct imaging New York, NY: Churchill-Livingstone, 1987; 36-46.
Rohrmann CA, Jr, Ansel HJ, Protell RL. Significance of the non-opacified gallbladder in endoscopic retrograde cholangiography. AJR Am J Roentgenol 1979; 132:191-195.[Abstract]
Mittelstaedt CA. Ultrasound of the bile ducts. Semin Roentgenol 1997; 32:161-171.[Medline]
Baron RL. Computed tomography of the bile ducts. Semin Roentgenol 1997; 32:172-187.[Medline]
Barish MA, Soto JA. MR cholangiopancreatography: techniques and clinical applications. AJR Am J Roentgenol 1997; 169:1295-1299.[Free Full Text]
Fulcher AS, Turner MA, Capps GW, Zfass AM, Baker KM. Half-Fourier RARE MRCP in 300 subjects. Radiology 1998; 207:21-28.[Abstract/Free Full Text]
Fulcher AS, Turner MA. Pitfalls of MR cholangiopancreatography (MRCP). J Comput Assist Tomogr 1998; 22:845-850.[Medline]
Taourel P, Bret PM, Reinhold C, Borkun AN, Atri M. Anatomic variations of the biliary tree: diagnosis with MR cholangiopancreatography. Radiology 1996; 199:521-526.[Abstract/Free Full Text]
Puente SG, Bannura GC. Radiological anatomy of the biliary tract: variations and congenital abnormalities. World J Surg 1983; 7:271-276.[Medline]
Hayes MA, Goldenberg IS, Bishop CC. The developmental basis for bile duct anomalies. Surg Gynecol Obstet 1958; 107:447-456.[Medline]
Schulte SJ. Embryology and congenital anomalies of the biliary and pancreatic ducts. In: Silvis SE, Rohrmann CA, Ansel HJ, eds. Techniques and interpretation of endoscopic retrograde cholangiopancreatography with endoscopic intervention. New York, NY: Igaku-Shoin, 1995; 114-145.
Hopkins SF, Bivins BA, Griffin WO. The problem of the cystic duct remnant. Surg Gynecol Obstet 1979; 148:531-533.[Medline]
Ghahremani GG. Post-surgical biliary tract complications. Gastroenterologist 1997; 5:46-57.[Medline]
Ghahremani GG, Crampton AR, Bernstein JR, Caprini JA. Iatrogenic biliary tract complications: radiologic features and clinical significance. RadioGraphics 1991; 11:441-456.[Abstract]
Goor DA, Ebert PA. Anomalies of the biliary tree. Arch Surg 1972; 104:302-309.[Medline]
Turner MA, Cho SR, Messmer JM. Pitfalls in cholangiographic interpretation. RadioGraphics 1987; 7:1067-1105.[Abstract]
Fulcher AS, Turner MA. Benign diseases of the biliary tract: evaluation with MR cholangiography. Semin Ultrasound CT MR 1999; 20:294-303.[Medline]
Reid SH, Cho SR, Shaw CI, Turner MA. Anomalous hepatic duct inserting into the cystic duct. AJR Am J Roentgenol 1988; 147:1181-1182.
Champetier J, Letoublon C, Alnaasan I, Charvin B. The cystohepatic ducts: surgical implications. Surg Radiol Anat 1991; 13:203-211.[Medline]
Christensen RA, vanSonnenberg E, Nemcek AA, Jr, D’Agostino HB. Inadvertent ligation of the aberrant right hepatic duct at cholecystectomy: radiologic diagnosis and therapy. Radiology 1992; 183:549-553.[Abstract/Free Full Text]
Laing FC, Jeffrey RB, Jr. Choledocholithiasis and cystic duct obstruction: difficult ultrasonographic diagnosis. Radiology 1983; 146:475-479.[Abstract/Free Full Text]
Brink JA, Semin MD. Biliary stone disease. In: Gazelle GS, Saini S, Mueller PR, eds. Hepatobiliary and pancreatic radiology: imaging and intervention. New York, NY: Thieme, 1998; 590-630.
Brink JA, Semin MD, Simeone JF. The gallbladder: pathology. In: Taveras JM, Ferrucci JT, eds. Radiology: diagnosis, imaging, intervention. New York, NY: Lippincott-Raven, 1996; 67:1-27.
Barakos JA, Ralls PW, Lapin SA. Cholelithiasis: evaluation with CT. Radiology 1987; 162:415-418.[Abstract/Free Full Text]
Weissmann HS, Badia J, Sugarman LA. Spectrum of 99m-Tc-IDA cholescintigraphic patterns in acute cholecystitis. Radiology 1981; 138:167-175.[Abstract/Free Full Text]
Kim EE, Pjura G, Lowry P. Morphine augmented cholescintigraphy in the diagnosis of acute cholecystitis. AJR Am J Roentgenol 1986; 147:1177-1179.[Abstract/Free Full Text]
Park MS, Yu JS, Kim YH, et al. Acute cholecystitis: comparison of MR cholangiography and US. Radiology 1998; 209:781-785.[Abstract/Free Full Text]
Htoo MM. Surgical implications of stone impaction in the gallbladder neck with compression of the common hepatic duct (Mirizzi syndrome). Clin Radiol 1983; 34:651-655.[Medline]
Cruz FO, Barriga P, Tocornali J, Burhenne HJ. Radiology of the Mirizzi syndrome: diagnostic importance of the percutaneous transhepatic cholangiogram. Gastrointest Radiol 1983; 8:249-253.[Medline]
Hilger DJ, Versteeg KR, Beaty PJ. Mirizzi syndrome with common septum: ultrasound and computed tomography findings. J Ultrasound Med 1988; 7:409-411.[Medline]
Becker CD, Hassler H, Terrier F. Preoperative diagnosis of the Mirizzi syndrome: limitations of sonography and computed tomography. AJR Am J Roentgenol 1984; 143:591-596.[Abstract/Free Full Text]
Fulcher AS, Turner MA, Capps GW. MR cholangiography: technical advances and clinical applications. RadioGraphics 1999; 19:25-41.[Abstract/Free Full Text]
Beachley MC, Ghahremani GG, Southworth LE, Siconolfi EP. Clinical and roentgen manifestations of cholecystoduodenal fistula. Am J Dig Dis 1976; 21:482-488.[Medline]
Yedlicka JW, Tadavarthy SM, Letourneau JG. Biliary tract intervention: interventional techniques in the hepatobiliary system. In: Castaneda-Zuniga WR, eds. Interventional radiology. Baltimore, Md: Williams & Wilkins, 1997; 1439-1573.
MacCarty RL, LaRusso NF, Wiesner RH, Ludwig J. Primary sclerosing cholangitis: findings on cholangiography and pancreatography. Radiology 1983; 149:39-44.[Abstract/Free Full Text]
Bodnall B, Overgaard B. Cystic duct remnant after cholecystectomy: incidence studied by cholangiography in 500 cases and significance in 103 reoperations. Ann Surg 1966; 163:382-390.[Medline]
Zajko AB, Campbell WL, Bron KM. Cholangiography and interventional biliary radiology in adult liver transplantation. AJR Am J Roentgenol 1985; 149:127-133.
Zajko AB, Campbell WL, Bron KM, Shade RR, Koneru B, Van Thiel DH. Diagnostic and interventional radiology in liver transplantation. Gastroenterol Clin North Am 1988; 17:105-143.[Medline]
Zajko AB, Campbell WL, Bron KM, Behal R, VanThiel DH, Starzl TE. Percutaneous cholangiography and biliary drainage after liver transplantation: a five-year experience. Gastrointest Radiol 1987; 12:137-143.[Medline]
Rappaport AS, Diamond AB. Cholangiographic demonstration of post-operative bile leakage from aberrant biliary ducts. Gastrointest Radiol 1981; 5:273-276.
Train JS, Norick A, Dan SJ. Radiolucency in the common bile duct simulating a gallstone. AJR Am J Roentgenol 1987; 148:136-138.[Free Full Text]
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Valves of Heister and the Archimedes Waterscrew
82656b23.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Valves of Heister and the Archimedes Waterscrew
82656b23.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 82656b23.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 82656b23.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Valves of Heister and the Archimedes Waterscrew
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Valves of Heister and the Archimedes Waterscrew
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Filling
This diagram illustrates the concept of how the gallbladder receives bile via the relatively high lying (cranially positioned) cystic duct, using a stepwise ladder system of valves to deliver the dilute bile to the gallbladder without a pump. An Archimedes water screw in the position of the spiral valves is shown revealing the parallel mechanism of action. In the case of the spiral valves the driving force is a is a push from the bottom, rather than a pull from the top. The spirals are not as complete as the screws of the Archomedes device. Rather they are a series of sacs of small diameter that have membranous folds that spiral and prevent backflow. (we propose)
The bile produced during the day in the biliary system will cause a minimal rise in pressure 82656b20.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Filling
This diagram illustrates the concept of how the gallbladder receives bile via the relatively high lying (cranially positioned) cystic duct, using a stepwise ladder system of valves to deliver the dilute bile to the gallbladder without a pump. An Archimedes water screw in the position of the spiral valves is shown revealing the parallel mechanism of action. In the case of the spiral valves the driving force is a is a push from the bottom, rather than a pull from the top. The spirals are not as complete as the screws of the Archomedes device. Rather they are a series of sacs of small diameter that have membranous folds that spiral and prevent backflow. (we propose)
The bile produced during the day in the biliary system will cause a minimal rise in pressure 82656b20.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This diagram illustrates the concept of how the gallbladder receives bile via the relatively high lying (cranially positioned) cystic duct, using a stepwise ladder system of valves to deliver the dilute bile to the gallbladder without a pump. An Archimedes water screw in the position of the spiral valves is shown revealing the parallel mechanism of action. In the case of the spiral valves the driving force is a is a push from the bottom, rather than a pull from the top. The spirals are not as complete as the screws of the Archomedes device. Rather they are a series of sacs of small diameter that have membranous folds that spiral and prevent backflow. (we propose)
The bile produced during the day in the biliary system will cause a minimal rise in pressure 82656b20.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This diagram illustrates the concept of how the gallbladder receives bile via the relatively high lying (cranially positioned) cystic duct, using a stepwise ladder system of valves to deliver the dilute bile to the gallbladder without a pump. An Archimedes water screw in the position of the spiral valves is shown revealing the parallel mechanism of action. In the case of the spiral valves the driving force is a is a push from the bottom, rather than a pull from the top. The spirals are not as complete as the screws of the Archomedes device. Rather they are a series of sacs of small diameter that have membranous folds that spiral and prevent backflow. (we propose)
The bile produced during the day in the biliary system will cause a minimal rise in pressure 82656b20.8s gallbladder Archimedes water screw cystic duct gravity upright spiral valves of Heister filling ampulla of VAter closed neck body fundus distended sympathetic bile duct Davidoff art Copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Filling
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Filling
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Archimedes Water Screw
The design of the water screw has been attributed to Archimedes from 3rd century BC though some designate the originator of the screw to be Nebuchadnezzar II of 7th century BC who purportedly used the screw to deliver water to the Hanging Gardens of Babylon. Water at a low level is scooped up into the spiral mechanism. As the screw rotates, the water advances upward and gets delivered to a higher level until it finally reaches its destination and is delivered to a repository.
has been 82656b15.8s Archimedes water screw elevation gravity screw delivery cystic duct spiral valves of Heister anatomy physiology function uploading Davidoff art copyright 2008
The image was modified from Wikipedia; detail of image: Archimedes’ screw. Public domain, from Chambers’s Encyclopedia (Philadelphia: J. B. Lippincott Company, 1875). Added to illustrate article :Archimedes.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Archimedes Water Screw
The design of the water screw has been attributed to Archimedes from 3rd century BC though some designate the originator of the screw to be Nebuchadnezzar II of 7th century BC who purportedly used the screw to deliver water to the Hanging Gardens of Babylon. Water at a low level is scooped up into the spiral mechanism. As the screw rotates, the water advances upward and gets delivered to a higher level until it finally reaches its destination and is delivered to a repository.
has been 82656b15.8s Archimedes water screw elevation gravity screw delivery cystic duct spiral valves of Heister anatomy physiology function uploading Davidoff art copyright 2008
The image was modified from Wikipedia; detail of image: Archimedes’ screw. Public domain, from Chambers’s Encyclopedia (Philadelphia: J. B. Lippincott Company, 1875). Added to illustrate article :Archimedes.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The design of the water screw has been attributed to Archimedes from 3rd century BC though some designate the originator of the screw to be Nebuchadnezzar II of 7th century BC who purportedly used the screw to deliver water to the Hanging Gardens of Babylon. Water at a low level is scooped up into the spiral mechanism. As the screw rotates, the water advances upward and gets delivered to a higher level until it finally reaches its destination and is delivered to a repository.
has been 82656b15.8s Archimedes water screw elevation gravity screw delivery cystic duct spiral valves of Heister anatomy physiology function uploading Davidoff art copyright 2008
The image was modified from Wikipedia; detail of image: Archimedes’ screw. Public domain, from Chambers’s Encyclopedia (Philadelphia: J. B. Lippincott Company, 1875). Added to illustrate article :Archimedes.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The design of the water screw has been attributed to Archimedes from 3rd century BC though some designate the originator of the screw to be Nebuchadnezzar II of 7th century BC who purportedly used the screw to deliver water to the Hanging Gardens of Babylon. Water at a low level is scooped up into the spiral mechanism. As the screw rotates, the water advances upward and gets delivered to a higher level until it finally reaches its destination and is delivered to a repository.
has been 82656b15.8s Archimedes water screw elevation gravity screw delivery cystic duct spiral valves of Heister anatomy physiology function uploading Davidoff art copyright 2008
The image was modified from Wikipedia; detail of image: Archimedes’ screw. Public domain, from Chambers’s Encyclopedia (Philadelphia: J. B. Lippincott Company, 1875). Added to illustrate article :Archimedes.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Archimedes Water Screw
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Archimedes Water Screw
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dilated Cystic Duct Pancreatic Carcinoma
The transverse section of the base of the gallbladder shows the distended body (darkest green), sinusoid neck of the gallbladder (intermediate green) connected to the similalrly distended spiral portion of the cystic duct (light green) in this patient with carcinoma of the head of the pancreas. The cystic duct is dilated and therefore visualized. The cystic duct is not normally visualized for a number of reasons. It is relatively small (1-2mm), lies deep in the porta hepatis surrounded by the echogenic Glissons capsule and other structures of the porta , and it is of itself echogenic because of the many valves which reflect echoes as well. All the echogenic structures prevent resolution of the small duct. Because the bile duct is obstructed by the pancreatic cancer, all the upstream components have become distended and the patient as a result becomes jaundiced.
04648c.8s patient with pancreatic carcinoma gallbladder dilated neck cystic duct valves of Heister dilated enlarged obstruction USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dilated Cystic Duct Pancreatic Carcinoma
The transverse section of the base of the gallbladder shows the distended body (darkest green), sinusoid neck of the gallbladder (intermediate green) connected to the similalrly distended spiral portion of the cystic duct (light green) in this patient with carcinoma of the head of the pancreas. The cystic duct is dilated and therefore visualized. The cystic duct is not normally visualized for a number of reasons. It is relatively small (1-2mm), lies deep in the porta hepatis surrounded by the echogenic Glissons capsule and other structures of the porta , and it is of itself echogenic because of the many valves which reflect echoes as well. All the echogenic structures prevent resolution of the small duct. Because the bile duct is obstructed by the pancreatic cancer, all the upstream components have become distended and the patient as a result becomes jaundiced.
04648c.8s patient with pancreatic carcinoma gallbladder dilated neck cystic duct valves of Heister dilated enlarged obstruction USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The transverse section of the base of the gallbladder shows the distended body (darkest green), sinusoid neck of the gallbladder (intermediate green) connected to the similalrly distended spiral portion of the cystic duct (light green) in this patient with carcinoma of the head of the pancreas. The cystic duct is dilated and therefore visualized. The cystic duct is not normally visualized for a number of reasons. It is relatively small (1-2mm), lies deep in the porta hepatis surrounded by the echogenic Glissons capsule and other structures of the porta , and it is of itself echogenic because of the many valves which reflect echoes as well. All the echogenic structures prevent resolution of the small duct. Because the bile duct is obstructed by the pancreatic cancer, all the upstream components have become distended and the patient as a result becomes jaundiced.
04648c.8s patient with pancreatic carcinoma gallbladder dilated neck cystic duct valves of Heister dilated enlarged obstruction USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The transverse section of the base of the gallbladder shows the distended body (darkest green), sinusoid neck of the gallbladder (intermediate green) connected to the similalrly distended spiral portion of the cystic duct (light green) in this patient with carcinoma of the head of the pancreas. The cystic duct is dilated and therefore visualized. The cystic duct is not normally visualized for a number of reasons. It is relatively small (1-2mm), lies deep in the porta hepatis surrounded by the echogenic Glissons capsule and other structures of the porta , and it is of itself echogenic because of the many valves which reflect echoes as well. All the echogenic structures prevent resolution of the small duct. Because the bile duct is obstructed by the pancreatic cancer, all the upstream components have become distended and the patient as a result becomes jaundiced.
04648c.8s patient with pancreatic carcinoma gallbladder dilated neck cystic duct valves of Heister dilated enlarged obstruction USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Dilated Cystic Duct Pancreatic Carcinoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Dilated Cystic Duct Pancreatic Carcinoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Stone Imapacted in the Cystic Duct
The artistic rendition shows a smallstone impacted in the spiral valves of Heister, with inflammation of the wall, upstream distension due to exudation of fluid. The gallbladder enlarges becomes rotund, and the upstream cystic duct distends. new bile cannot enter and bile cannot leave the gallbladder.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Stone Imapacted in the Cystic Duct
The artistic rendition shows a smallstone impacted in the spiral valves of Heister, with inflammation of the wall, upstream distension due to exudation of fluid. The gallbladder enlarges becomes rotund, and the upstream cystic duct distends. new bile cannot enter and bile cannot leave the gallbladder.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The artistic rendition shows a smallstone impacted in the spiral valves of Heister, with inflammation of the wall, upstream distension due to exudation of fluid. The gallbladder enlarges becomes rotund, and the upstream cystic duct distends. new bile cannot enter and bile cannot leave the gallbladder.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The artistic rendition shows a smallstone impacted in the spiral valves of Heister, with inflammation of the wall, upstream distension due to exudation of fluid. The gallbladder enlarges becomes rotund, and the upstream cystic duct distends. new bile cannot enter and bile cannot leave the gallbladder.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Stone Imapacted in the Cystic Duct
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Stone Imapacted in the Cystic Duct
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Distal Insertion of the Cystic Duct
In this ERCP the straight portion of the cystic duct (orange) inserts into the medial aspect of the common hepatic duct (light olive) to form the common bile duct (dark olive) just proximal to the ampulla. This a variant of normal for the length of the cystic duct, its coparalely medial course, and its distal medial insertion. The result is also a long common hepatic duct and a short common bile duct.
39963c02.8s gallbladder parts normal anatomy cystic duct The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. straight portion = orange common hepatic duct = light olive yellow variant of length insertion position anatomy parts ERCP Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Distal Insertion of the Cystic Duct
In this ERCP the straight portion of the cystic duct (orange) inserts into the medial aspect of the common hepatic duct (light olive) to form the common bile duct (dark olive) just proximal to the ampulla. This a variant of normal for the length of the cystic duct, its coparalely medial course, and its distal medial insertion. The result is also a long common hepatic duct and a short common bile duct.
39963c02.8s gallbladder parts normal anatomy cystic duct The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. straight portion = orange common hepatic duct = light olive yellow variant of length insertion position anatomy parts ERCP Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this ERCP the straight portion of the cystic duct (orange) inserts into the medial aspect of the common hepatic duct (light olive) to form the common bile duct (dark olive) just proximal to the ampulla. This a variant of normal for the length of the cystic duct, its coparalely medial course, and its distal medial insertion. The result is also a long common hepatic duct and a short common bile duct.
39963c02.8s gallbladder parts normal anatomy cystic duct The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. straight portion = orange common hepatic duct = light olive yellow variant of length insertion position anatomy parts ERCP Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this ERCP the straight portion of the cystic duct (orange) inserts into the medial aspect of the common hepatic duct (light olive) to form the common bile duct (dark olive) just proximal to the ampulla. This a variant of normal for the length of the cystic duct, its coparalely medial course, and its distal medial insertion. The result is also a long common hepatic duct and a short common bile duct.
39963c02.8s gallbladder parts normal anatomy cystic duct The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. straight portion = orange common hepatic duct = light olive yellow variant of length insertion position anatomy parts ERCP Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Distal Insertion of the Cystic Duct
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Distal Insertion of the Cystic Duct
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cyctic Duct Joining the Bile Duct
29247c04.8s gallbladder parts normal anatomy neck cystic duct spiral portion spiral valves of Heister The proximal portion is called the spiral portion, (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not known.. The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. neck = dark green spiral portion = light green straight portion common hepatic duct light olive common bile duct = dark olive ERCP Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cyctic Duct Joining the Bile Duct
29247c04.8s gallbladder parts normal anatomy neck cystic duct spiral portion spiral valves of Heister The proximal portion is called the spiral portion, (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not known.. The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. neck = dark green spiral portion = light green straight portion common hepatic duct light olive common bile duct = dark olive ERCP Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 29247c04.8s gallbladder parts normal anatomy neck cystic duct spiral portion spiral valves of Heister The proximal portion is called the spiral portion, (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not known.. The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. neck = dark green spiral portion = light green straight portion common hepatic duct light olive common bile duct = dark olive ERCP Courtesy Ashley Davidoff MD copyright 2008
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 29247c04.8s gallbladder parts normal anatomy neck cystic duct spiral portion spiral valves of Heister The proximal portion is called the spiral portion, (pars spiralis) and as its name implies is tortuos and contains the spiral valves of Heister. They appear to regulate flow into and out of the gallbladder but their true function is not known.. The distal part is straight, usually short and and smooth and is called the pars glabra. This portion in some patients can be extremely long if it joins with the bile duct at its distal downstream end. neck = dark green spiral portion = light green straight portion common hepatic duct light olive common bile duct = dark olive ERCP Courtesy Ashley Davidoff MD copyright 2008
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Cyctic Duct Joining the Bile Duct
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Cyctic Duct Joining the Bile Duct
)
