
Disease
The Common Vein Copyright 2007
- Disease Introduction
- ?
- Appendicitis
- Bannayan-Riley-Ruvalcaba
- Carcinoma Colon
- Colovaginal Fistula
- Colovesical fistula
- Crohn?s Colitis
- Diverticulosis
- Hyperplastic Polyp of the Colon
- Infarction
- Mucocele of the Appendix
- Obstruction of the Colon
- Oldfield Syndrome
- Peutz-Jeghers syndrome
- Pneumatosis Intestinalis Primary
- Pneumatosis Intestinalis Secondary
- Polyp Adenomatous
- Polyps Colon
- Pseudopolyps
- Rectocele
- Ulcerative Colitis
- Volvulus
Diarrhea and constipation
Diarrhea is caused by mucosal malfunction most commonly called colitis or enteritis as stated above. There are many causes of diarrhea. Infections caused by Salmonella, Shigella and cholera cause diarrhea by affecting the mucosa while others such as amebiasis and Schistosomiasis affect the deeper layers as well. Ulcerative colitis another well known cause of chronic diarrhea is a non infectious mucosal disease while Crohn?s disease, ischemic colitis, and pseudomembranous colitis are transmural diseases, which mean they affect the entire wall of the bowel. When a disease is isolated to the mucosa, CTscan may show bowel thickening but will not show induration of the pericolonic fat. In transmural disease the CT findings include wall thickening as well as changes in the pericolonic fat.
From a clinical standpoint diarrhea is defined as an increased frequency (more than 3 times per day) of liquid like stools. It can also be defined as a daily stool weight of greater than 200grams. The usual weight of stools is 100-200grams. The classifications of diarrhea are based on duration of the illness (acute vs chronic), based on the pathophysiological causes (osmotic vs secretory) or based on the cause (infectious, ischemic, inflammatory). (Sanaka and Soffer)
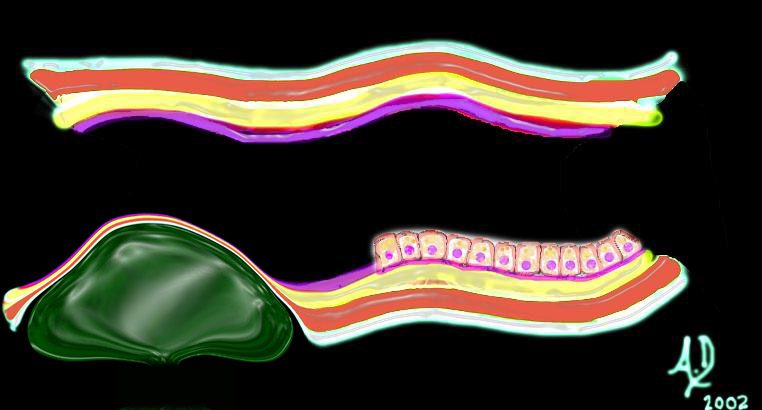
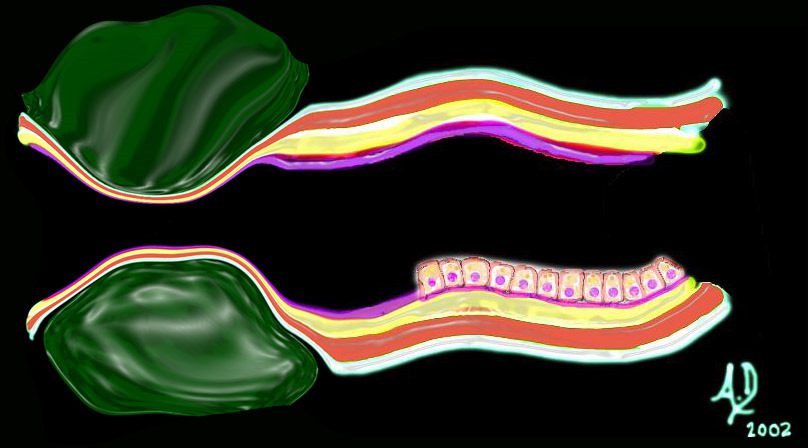
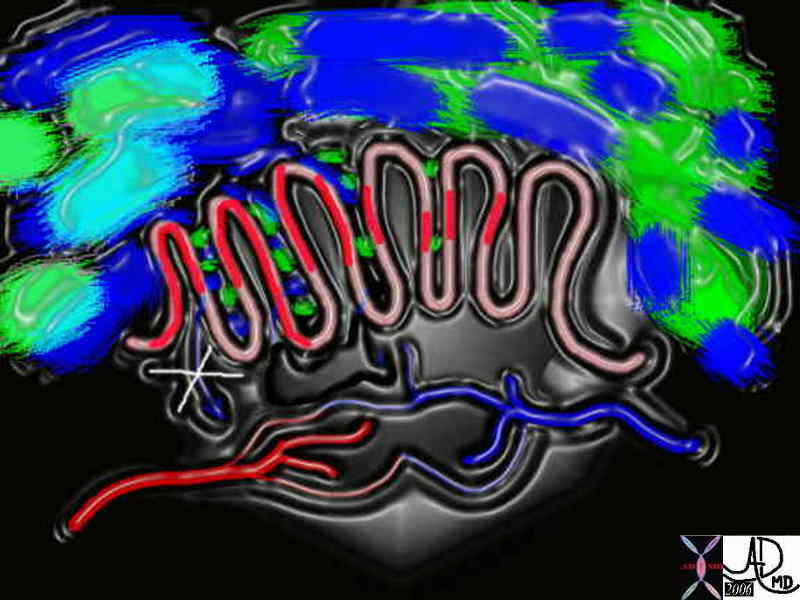  Diagrammatic representation of colon with intact function and malfunction. Diagrammatic representation of colon with intact function and malfunction. |
| Image on left shows normal colon. The chyme to the left contains both fluid (royal blue), semi solid (light blue) and solid components (light green). The chyme is processed in the crypts and the water gets absorbed into the capillaries and then into the veins. The end product is the donut shaped solid nugget (aka scybala) of feces (dark green). In the second image the mucosa in the crypts is inflamed and is malfunctioning. (red) The chyme cannot be optimally processed and the water and electrolytes are not absorbed. In addition mucus may be secreted in excessive amounts resulting in a semisolid or liquid stool.
Courtesy Ashley Davidoff MD 44953c04.800 44953c05.800 |
The character of stools is very easy to evaluate on CTscanning. When stools are watery an air fluid level will be seen and when they are semi solid, there will be a combination of air fluid levels as well as air caught within the substance, while well formed stool will have no water.
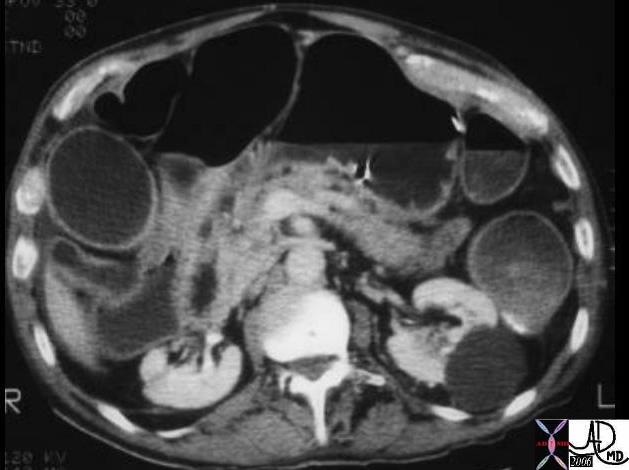 Ulcerative colitis ? fluid contents Ulcerative colitis ? fluid contents |
| Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71year old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff MD 04198 |
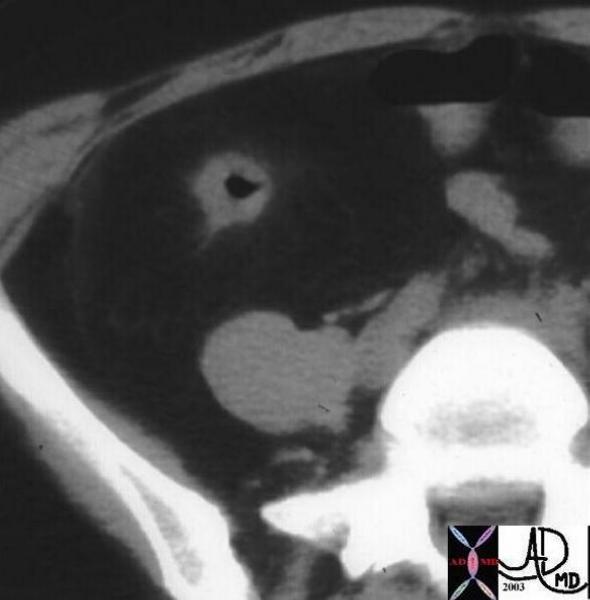 Ascending colon ? Crohn?s disease Ascending colon ? Crohn?s disease |
| In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff MD 12069 |
 Ischemic colitis of the transverse colon Ischemic colitis of the transverse colon |
| The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD 16888 |
There is no single universal definition of constipation because of the wide variability of the bowel habits. The parameters that are considered for the diagnosis include the frequency and nature of the stool, the need and degree of effort to evacuate, and the sensation of incomplete evacuation. There are two basic causes of constipation. The first is called primary or idiopathic constipation which implies that there is no known cause, and the second is called secondary constipation, implying that there is a known cause for the entity. There are 3 types in the idiopathic group including: normal-transit constipation, slow-transit constipation, and dyssynergic defecation. In the normal-transit constipation the time that it takes to form and transport the stool is normal but the patient has a perception of difficulty in passing the stool. In the slow transit constipation, transit time as implied is slow and urge to defecate is also reduced. In the dyssynergic defecation the coordination required to process the action of defecation is lost.
The secondary causes of constipation include a long list of drugs, metabolic, psychogenic, endocrinologic, and gastrointestinal disorders.
 Constipation Constipation |
| The series of images shows the radiological equivalent of constipation in this 28year female patient who complained of bloating. The entire colon is distended with feces (a,b,c,d,e) though the rectum is empty.(f)
Courtesy Ashley Davidoff MD 39195cL |
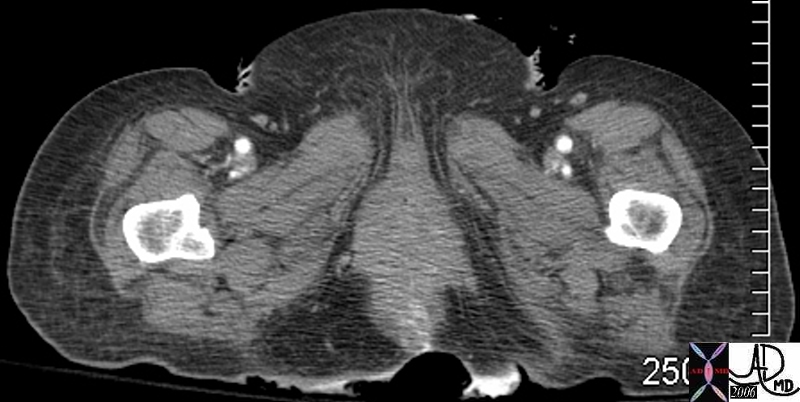
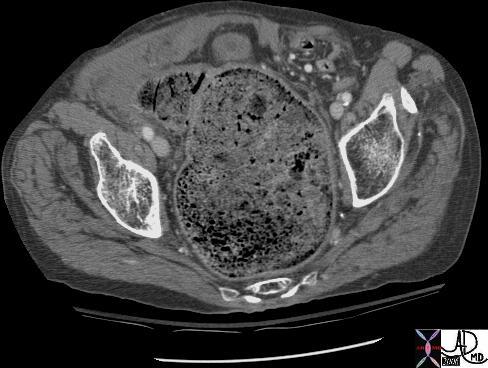 Rectal impaction and megarectum Rectal impaction and megarectum |
| This CTscan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff MD 18278 |
 Diarrhea Diarrhea |
| The contrast we administer orally commonly causes diarrhea and when the patient is also incontinent, spillage of colonic content as apparent on the posterior aspect of this patient can occur.
Courtesy Ashley Davidoff MD 45358 |
Disease
Principles
 Basic Strcture of Tubular Systems Basic Strcture of Tubular Systems |
| 32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology |
 Mucosal Lesion Mucosal Lesion |
| 32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
 Submucosal Lesion Submucosal Lesion |
| 32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
 Submucosal Lesion Submucosal Lesion |
| 32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
 Extrinsic Lesion Extrinsic Lesion |
| 32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
 Circumferential Lesion Circumferential Lesion |
| 32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD |
Inflammation
Vasculitis
 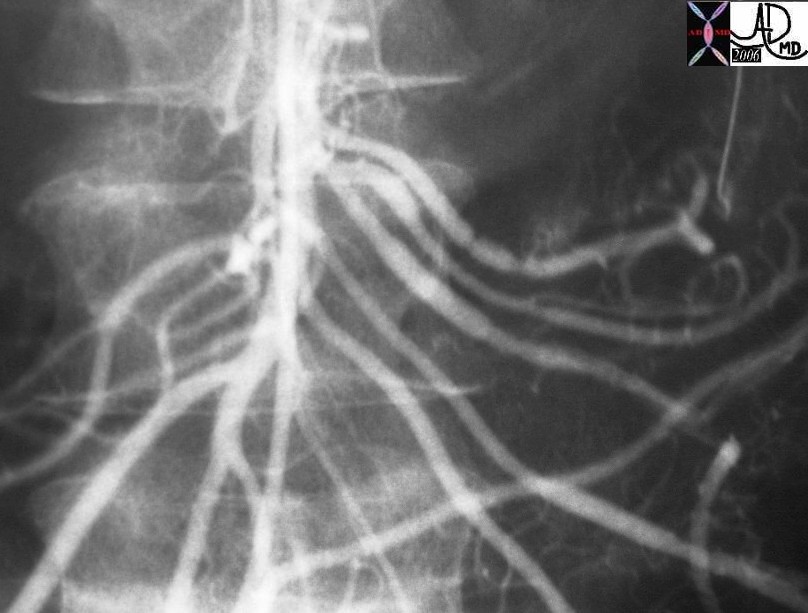 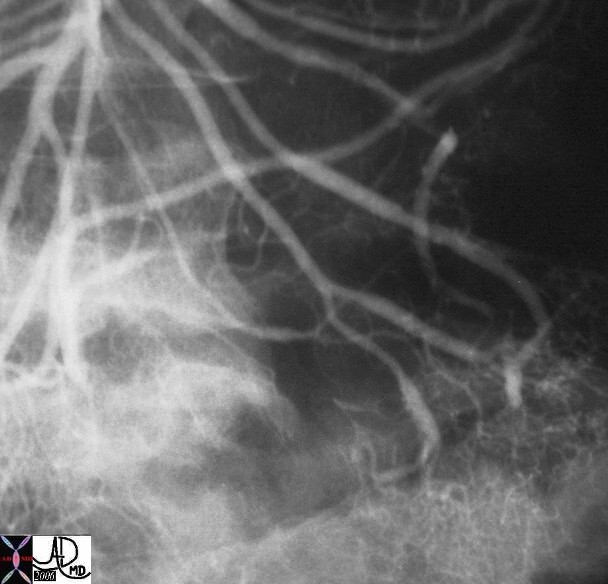 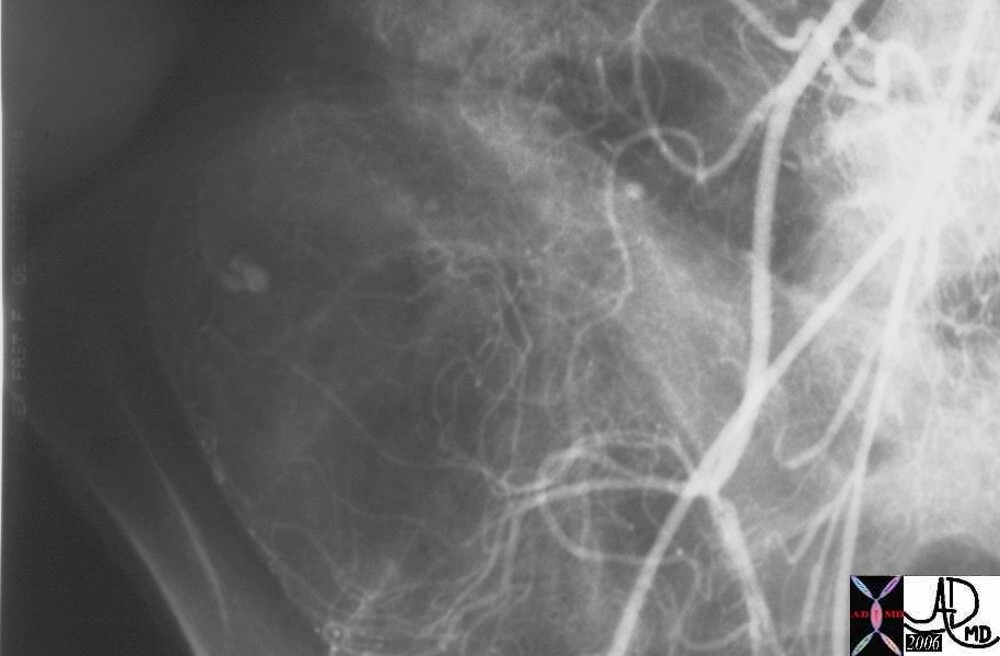 Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage |
| Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia |
Tumors
The most common site for tumor development is the mucosa. The mucosa is a highly active structure and cell turnover is rapid, with the reproduction of new cells and death of old cells occurring about every four days.
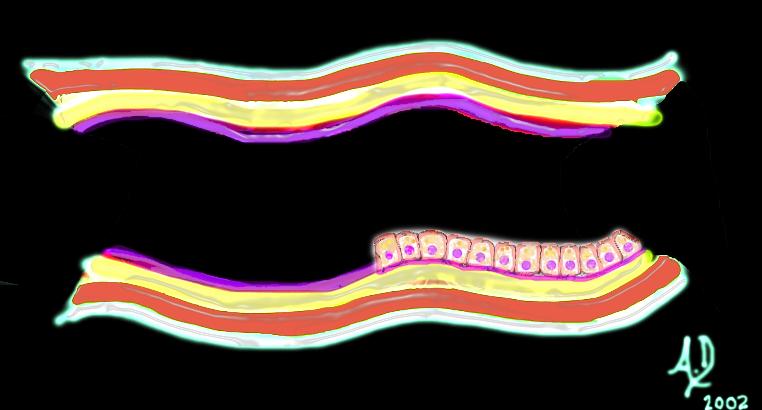
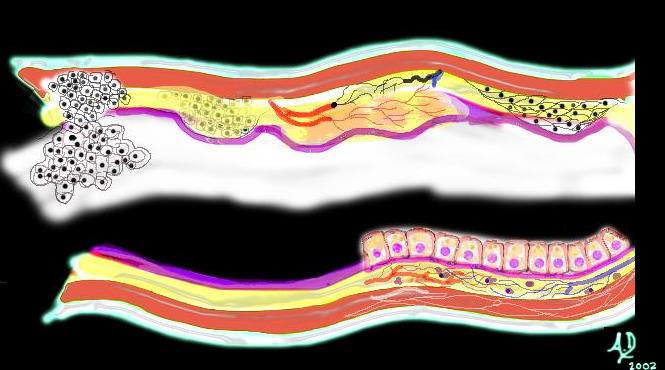
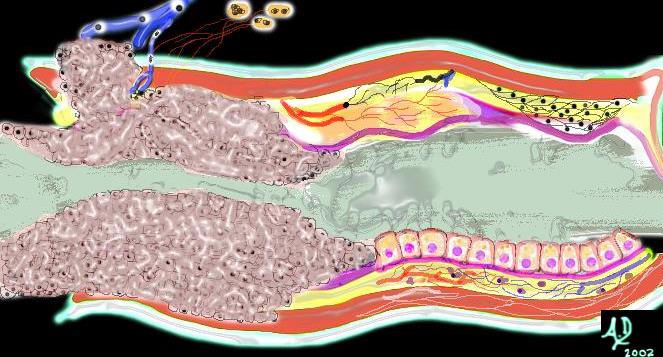
 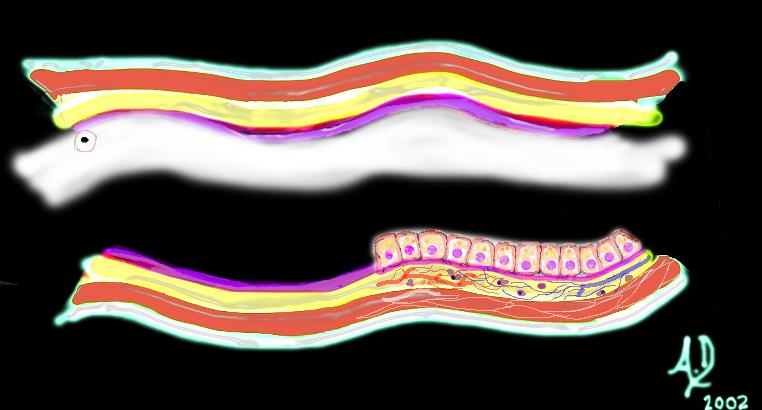 Mucosal disease ?beginning of a neoplasm Mucosal disease ?beginning of a neoplasm |
| The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? ie a new growth.
Courtesy Ashley Davidoff MD 32354 |
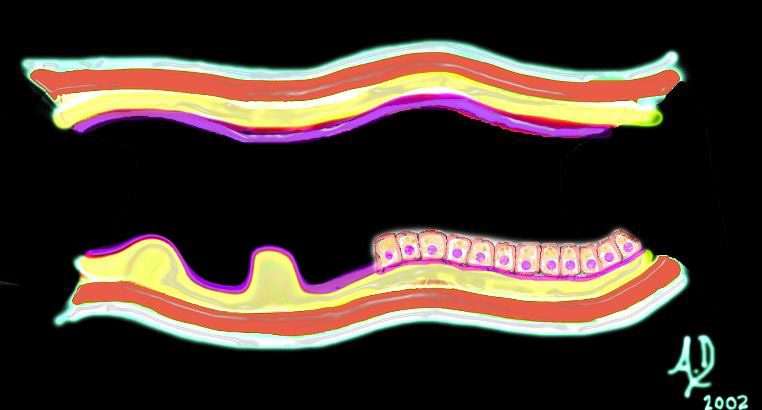
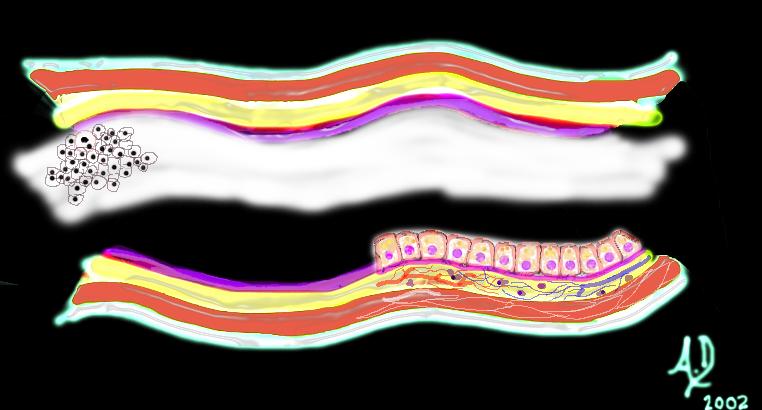 Mucosal disease -neoplasm Mucosal disease -neoplasm |
| Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD 32355 |
 5mm benign polyp 5mm benign polyp |
| This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD 12087 |
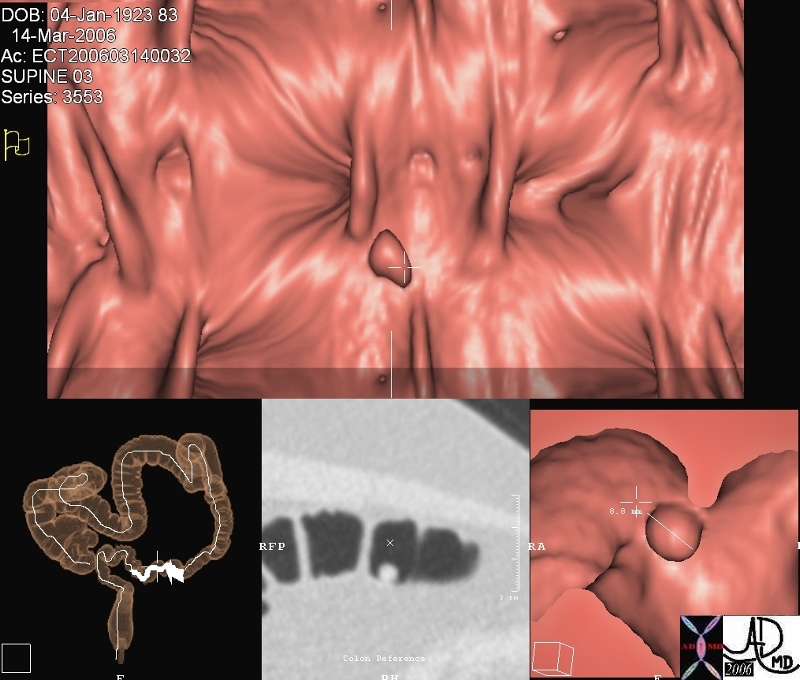
This series of images from a virtual colonoscopy shows an 8 mms polyp seen on the surface rendering images (salmon colored images) referenced to the sigmoid colon (bottom left) and with conventional CTimaging (bottom middle) At this size the polyp is almost certainly benign and can be removed through the colonoscope safely. Note in the gray scale image (middle image 2nd row) the acute angles formed by the polyp with the underlying mucosa. The distal location raises the likelihood that it represents a hyperplastic polyp.
Courtesy Scott Tsai MD
45119
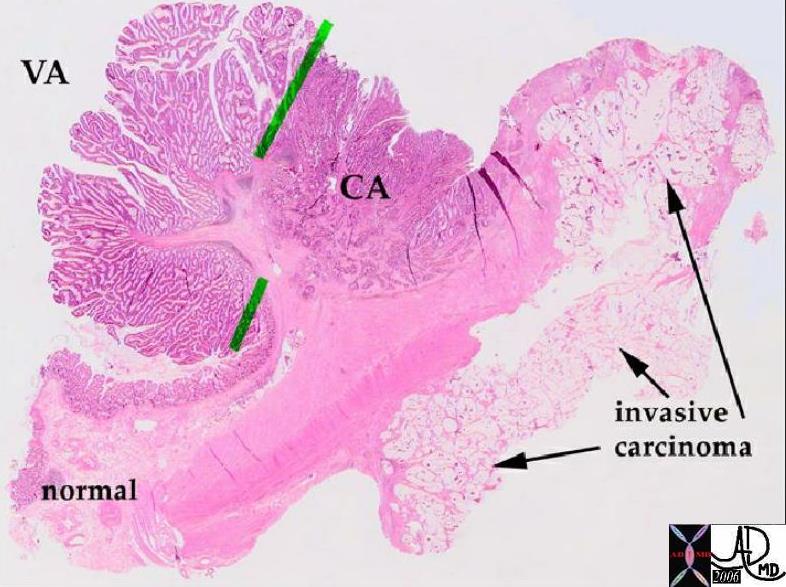 Pathology whole mount showing malignant transformation of a polyp Pathology whole mount showing malignant transformation of a polyp |
| In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base rightward and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD 12160 |
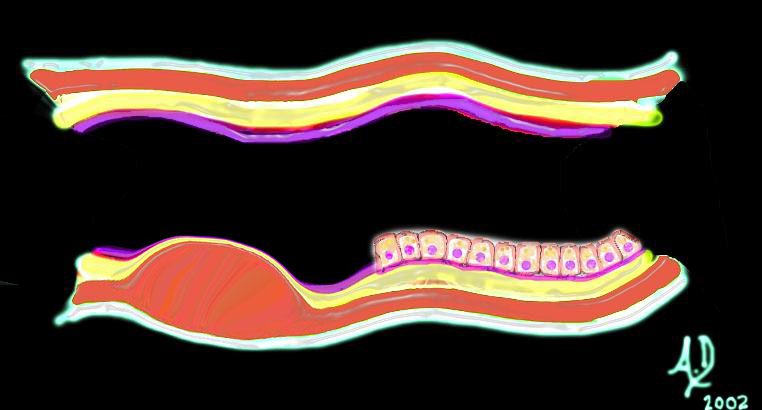
 Malignant and aggressive growth Malignant and aggressive growth |
| The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD 32362b01 |
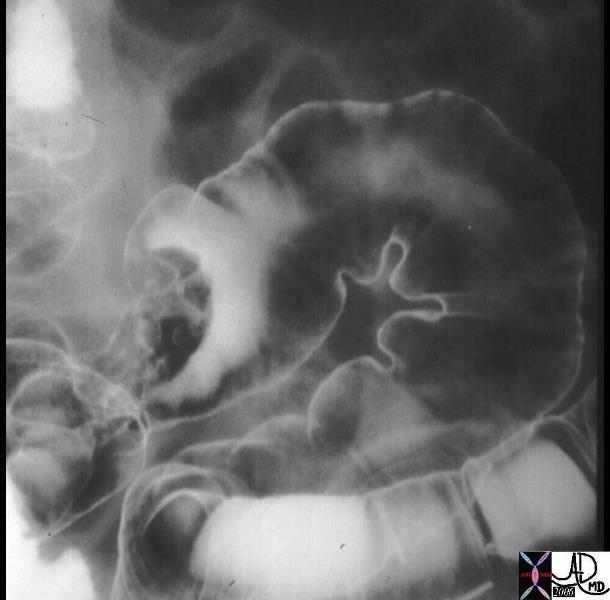 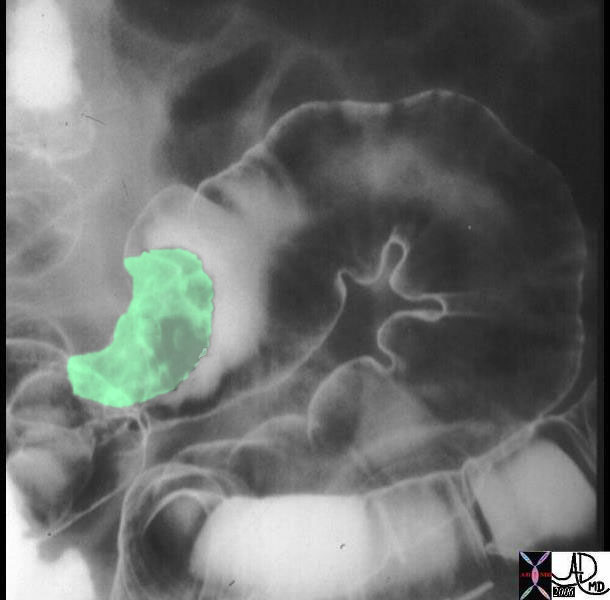 Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema. Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema. |
| The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the second image is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD 12175 12175bo1 |
Left undiagnosed and untreated the malignant cells continue to grow without regard to the neighboring structures. It encircles the colon in ?napkin-ring? fashion (as shown above) eventually blocking off the lumen and causing a bowel obstruction. It may grow through the wall and cause a bowel perforation and or grow into regional lymph nodes and portal venous radicles after which it will metastasize to the liver and other organs.
Courtesy Ashley Davidoff MD
32367b01
 Ugly ulcerating malignant tumor Ugly ulcerating malignant tumor |
| The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD 02330 |
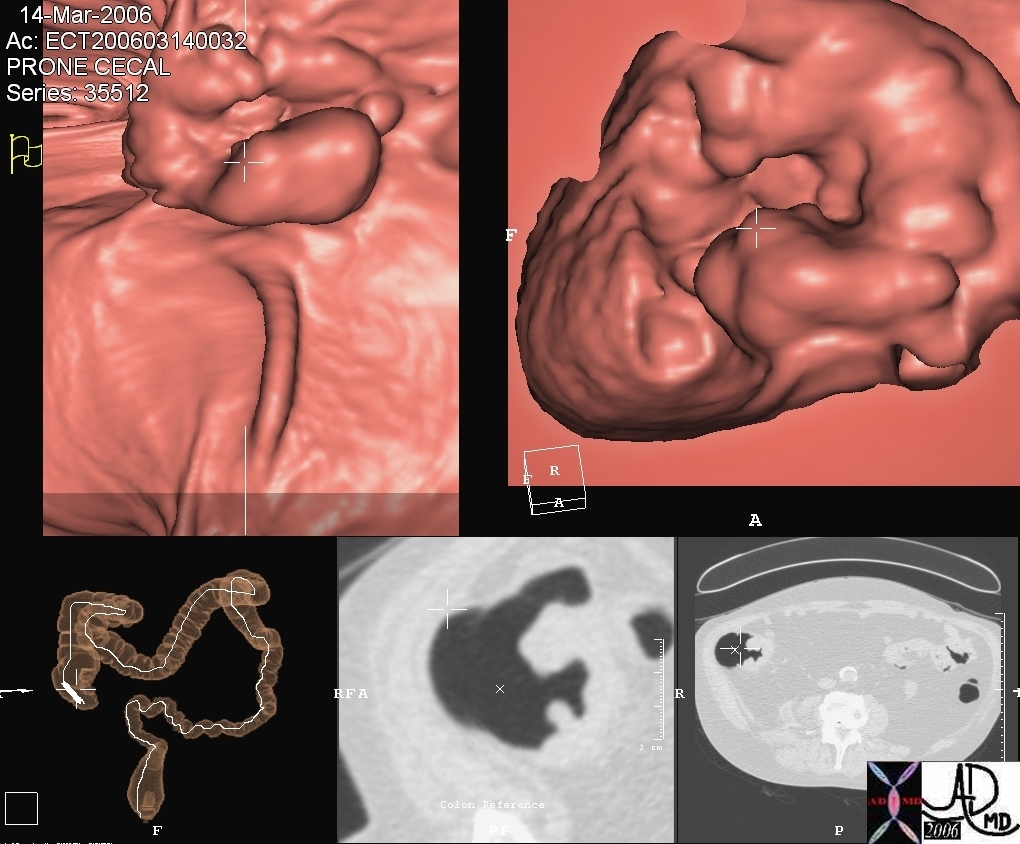
This series of images from a virtual colonoscopy shows a 5cms ulcerated mass seen on the surface rendering images (salmon colored images) referenced to the cecum (bottom left) and with conventional CT imaging (bottom middle) At this size and shape the mass is almost certainly malignant and cannot be removed through the colonoscope safely. Note how similar the morphology of this tumor is to the pathology of the specimen above (different patient)
Courtesy Scott Tsai MD
45123
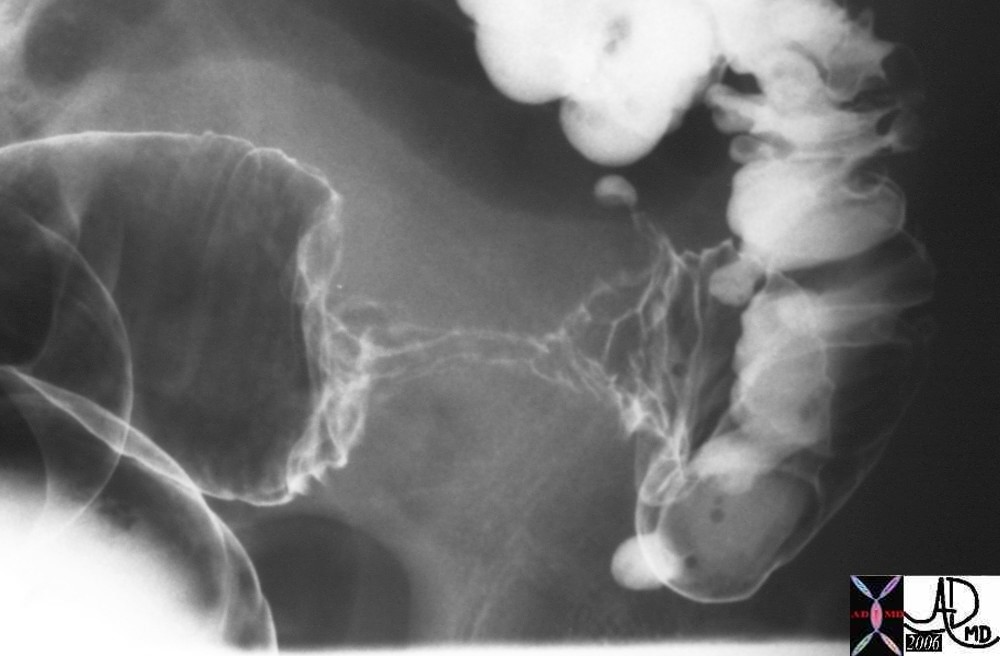 Apple core lesion of the sigmoid colon Apple core lesion of the sigmoid colon |
| The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD 28655 |
- Disease Introduction
- ?
- Appendicitis
- Bannayan-Riley-Ruvalcaba
- Carcinoma Colon
- Colovaginal Fistula
- Colovesical fistula
- Crohn?s Colitis
- Diverticulosis
- Hyperplastic Polyp of the Colon
- Infarction
- Mucocele of the Appendix
- Obstruction of the Colon
- Oldfield Syndrome
- Peutz-Jeghers syndrome
- Pneumatosis Intestinalis Primary
- Pneumatosis Intestinalis Secondary
- Polyp Adenomatous
- Polyps Colon
- Pseudopolyps
- Rectocele
- Ulcerative Colitis
- Volvulus
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Apple core lesion of the sigmoid colon
The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD
28655
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Apple core lesion of the sigmoid colon
The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD
28655
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD
28655
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in ?napkin-ring? fashion. The lumen is compromised. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD
28655
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Apple core lesion of the sigmoid colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Apple core lesion of the sigmoid colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ugly ulcerating malignant tumor
The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD
02330
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ugly ulcerating malignant tumor
The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD
02330
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD
02330
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD
02330
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Ugly ulcerating malignant tumor
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Ugly ulcerating malignant tumor
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema.
The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the second image is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD
12175 12175bo1
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema.
The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the second image is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD
12175 12175bo1
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the second image is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD
12175 12175bo1
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the second image is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD
12175 12175bo1
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Malignant and aggressive growth
The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD
32362b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Malignant and aggressive growth
The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD
32362b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD
32362b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD
32362b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Malignant and aggressive growth
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Malignant and aggressive growth
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pathology whole mount showing malignant transformation of a polyp
In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base rightward and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD
12160
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pathology whole mount showing malignant transformation of a polyp
In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base rightward and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD
12160
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base rightward and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD
12160
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base rightward and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD
12160
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Pathology whole mount showing malignant transformation of a polyp
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Pathology whole mount showing malignant transformation of a polyp
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
5mm benign polyp
This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD
12087
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
5mm benign polyp
This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD
12087
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD
12087
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD
12087
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 5mm benign polyp
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 5mm benign polyp
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Mucosal disease -neoplasm
Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD
32355
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Mucosal disease -neoplasm
Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD
32355
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD
32355
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD
32355
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Mucosal disease -neoplasm
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Mucosal disease -neoplasm
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Mucosal disease ?beginning of a neoplasm
The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? ie a new growth.
Courtesy Ashley Davidoff MD
32354
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Mucosal disease ?beginning of a neoplasm
The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? ie a new growth.
Courtesy Ashley Davidoff MD
32354
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? ie a new growth.
Courtesy Ashley Davidoff MD
32354
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become ?different? and instead of growing with characteristic columnar shape with pink nucleus and ?peaches and cream? cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm ? ie a new growth.
Courtesy Ashley Davidoff MD
32354
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Mucosal disease ?beginning of a neoplasm
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Mucosal disease ?beginning of a neoplasm
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Young female presents with GI bleed hemorrhage bleeding blood small bowel colon SMA superior mesenteric artery jejunal branches ileocolic artery fx arterial spasm fx contrast extravasation RLQ in cecum dx arteritis angiitis vasculitis arteriopathy dx Henoch -Schonlein arteritis angiography angiogram Courtesy Ashley Davidoff MD 28514 28515 28516 28517 surgical specimen showed plaque like ulcers in the bowel consistent with chronic ischemia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Henoch Schonlein Arteritis Segmental Spasm with Hemorrhage
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Circumferential Lesion
32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Circumferential Lesion
32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Circumferential Lesion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Circumferential Lesion
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Extrinsic Lesion
32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Extrinsic Lesion
32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Extrinsic Lesion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Extrinsic Lesion
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Submucosal Lesion
32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Submucosal Lesion
32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Submucosal Lesion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Submucosal Lesion
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Submucosal Lesion
32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Submucosal Lesion
32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Submucosal Lesion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Submucosal Lesion
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Mucosal Lesion
32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Mucosal Lesion
32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Mucosal Lesion
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Mucosal Lesion
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Basic Strcture of Tubular Systems
32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Basic Strcture of Tubular Systems
32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Basic Strcture of Tubular Systems
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Basic Strcture of Tubular Systems
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Diarrhea
The contrast we administer orally commonly causes diarrhea and when the patient is also incontinent, spillage of colonic content as apparent on the posterior aspect of this patient can occur.
Courtesy Ashley Davidoff MD
45358
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Diarrhea
The contrast we administer orally commonly causes diarrhea and when the patient is also incontinent, spillage of colonic content as apparent on the posterior aspect of this patient can occur.
Courtesy Ashley Davidoff MD
45358
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The contrast we administer orally commonly causes diarrhea and when the patient is also incontinent, spillage of colonic content as apparent on the posterior aspect of this patient can occur.
Courtesy Ashley Davidoff MD
45358
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The contrast we administer orally commonly causes diarrhea and when the patient is also incontinent, spillage of colonic content as apparent on the posterior aspect of this patient can occur.
Courtesy Ashley Davidoff MD
45358
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Diarrhea
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Diarrhea
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Rectal impaction and megarectum
This CTscan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff MD
18278
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Rectal impaction and megarectum
This CTscan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff MD
18278
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This CTscan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff MD
18278
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CTscan reflects a very uncomfortable looking scan which unfortunately is not uncommon in the elderly. The rectum is truly impacted with feces. Since this is a slow process of accumulation the mucosa muscularis and blood supply can usually accommodate the large volume, but at some point the wall can become compromised with ensuing obstruction, ischemia and perforation.
Courtesy Ashley Davidoff MD
18278
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Rectal impaction and megarectum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Rectal impaction and megarectum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Constipation
The series of images shows the radiological equivalent of constipation in this 28year female patient who complained of bloating. The entire colon is distended with feces (a,b,c,d,e) though the rectum is empty.(f)
Courtesy Ashley Davidoff MD
39195cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Constipation
The series of images shows the radiological equivalent of constipation in this 28year female patient who complained of bloating. The entire colon is distended with feces (a,b,c,d,e) though the rectum is empty.(f)
Courtesy Ashley Davidoff MD
39195cL
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The series of images shows the radiological equivalent of constipation in this 28year female patient who complained of bloating. The entire colon is distended with feces (a,b,c,d,e) though the rectum is empty.(f)
Courtesy Ashley Davidoff MD
39195cL
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The series of images shows the radiological equivalent of constipation in this 28year female patient who complained of bloating. The entire colon is distended with feces (a,b,c,d,e) though the rectum is empty.(f)
Courtesy Ashley Davidoff MD
39195cL
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Constipation
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Constipation
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ischemic colitis of the transverse colon
The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD
16888
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ischemic colitis of the transverse colon
The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD
16888
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD
16888
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The transverse colon in this patient is thick walled with mild transmural changes in the pericolonic fat in the right and left upper quadrants. Transmural changes occurred as a result of ischemia. Note the calcific atherosclerotic changes in the aorta.
Courtesy Ashley Davidoff MD
16888
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Ischemic colitis of the transverse colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Ischemic colitis of the transverse colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ascending colon ? Crohn?s disease
In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff MD
12069
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ascending colon ? Crohn?s disease
In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff MD
12069
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff MD
12069
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this patient with Crohn?s disease the ascending colon is empty, thick walled with changes noted in the pericolonic fat.
Courtesy Ashley Davidoff MD
12069
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Ascending colon ? Crohn?s disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Ascending colon ? Crohn?s disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ulcerative colitis ? fluid contents
Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71year old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff MD
04198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ulcerative colitis ? fluid contents
Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71year old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff MD
04198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71year old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff MD
04198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Note that in this patient the colon is mildly distended and the contents are fluid in nature, unlike the feces seen in the CT scans above. This 71year old male patient has diarrhea caused by ulcerative colitis which is a disease of the mucosa.
Courtesy Ashley Davidoff MD
04198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Ulcerative colitis ? fluid contents
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Ulcerative colitis ? fluid contents
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Diagrammatic representation of colon with intact function and malfunction.
Image on left shows normal colon. The chyme to the left contains both fluid (royal blue), semi solid (light blue) and solid components (light green). The chyme is processed in the crypts and the water gets absorbed into the capillaries and then into the veins. The end product is the donut shaped solid nugget (aka scybala) of feces (dark green). In the second image the mucosa in the crypts is inflamed and is malfunctioning. (red) The chyme cannot be optimally processed and the water and electrolytes are not absorbed. In addition mucus may be secreted in excessive amounts resulting in a semisolid or liquid stool.
Courtesy Ashley Davidoff MD
44953c04.800 44953c05.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Diagrammatic representation of colon with intact function and malfunction.
Image on left shows normal colon. The chyme to the left contains both fluid (royal blue), semi solid (light blue) and solid components (light green). The chyme is processed in the crypts and the water gets absorbed into the capillaries and then into the veins. The end product is the donut shaped solid nugget (aka scybala) of feces (dark green). In the second image the mucosa in the crypts is inflamed and is malfunctioning. (red) The chyme cannot be optimally processed and the water and electrolytes are not absorbed. In addition mucus may be secreted in excessive amounts resulting in a semisolid or liquid stool.
Courtesy Ashley Davidoff MD
44953c04.800 44953c05.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Image on left shows normal colon. The chyme to the left contains both fluid (royal blue), semi solid (light blue) and solid components (light green). The chyme is processed in the crypts and the water gets absorbed into the capillaries and then into the veins. The end product is the donut shaped solid nugget (aka scybala) of feces (dark green). In the second image the mucosa in the crypts is inflamed and is malfunctioning. (red) The chyme cannot be optimally processed and the water and electrolytes are not absorbed. In addition mucus may be secreted in excessive amounts resulting in a semisolid or liquid stool.
Courtesy Ashley Davidoff MD
44953c04.800 44953c05.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Image on left shows normal colon. The chyme to the left contains both fluid (royal blue), semi solid (light blue) and solid components (light green). The chyme is processed in the crypts and the water gets absorbed into the capillaries and then into the veins. The end product is the donut shaped solid nugget (aka scybala) of feces (dark green). In the second image the mucosa in the crypts is inflamed and is malfunctioning. (red) The chyme cannot be optimally processed and the water and electrolytes are not absorbed. In addition mucus may be secreted in excessive amounts resulting in a semisolid or liquid stool.
Courtesy Ashley Davidoff MD
44953c04.800 44953c05.800
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Diagrammatic representation of colon with intact function and malfunction.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Diagrammatic representation of colon with intact function and malfunction.
)