
|
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cms in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease the most common being acute pancreatitis. It receives its blood supply from the left colic artery and drains into the left colic vein.
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon. Applied AnatomyCrohn?s disease
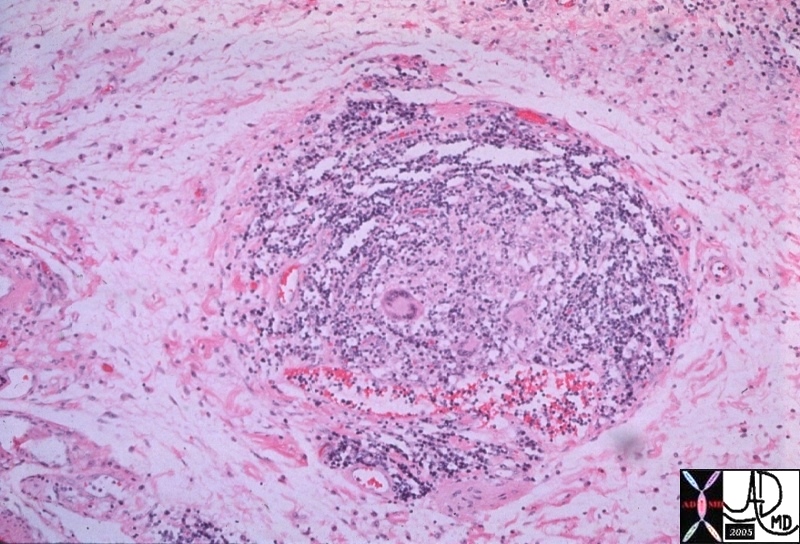
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.
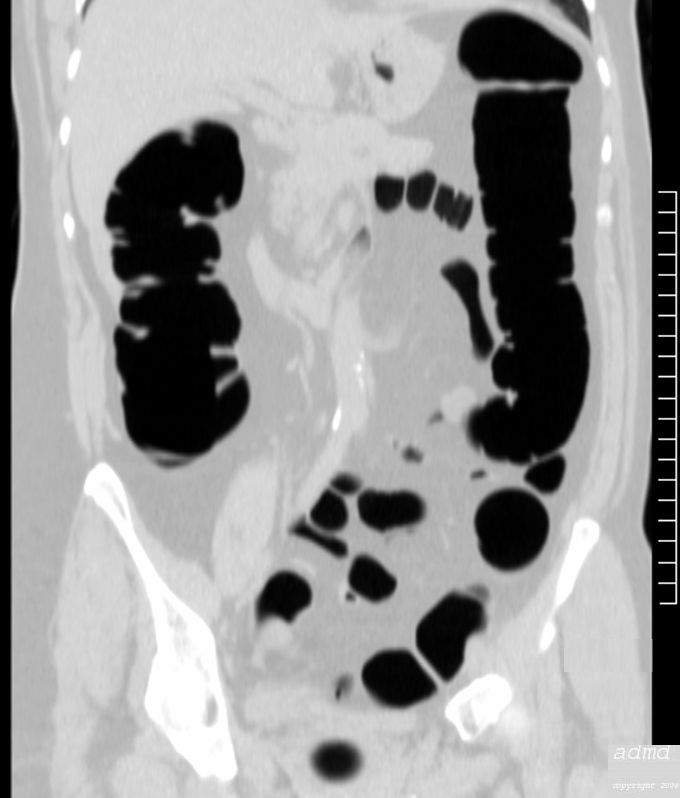
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.
Lymphoma
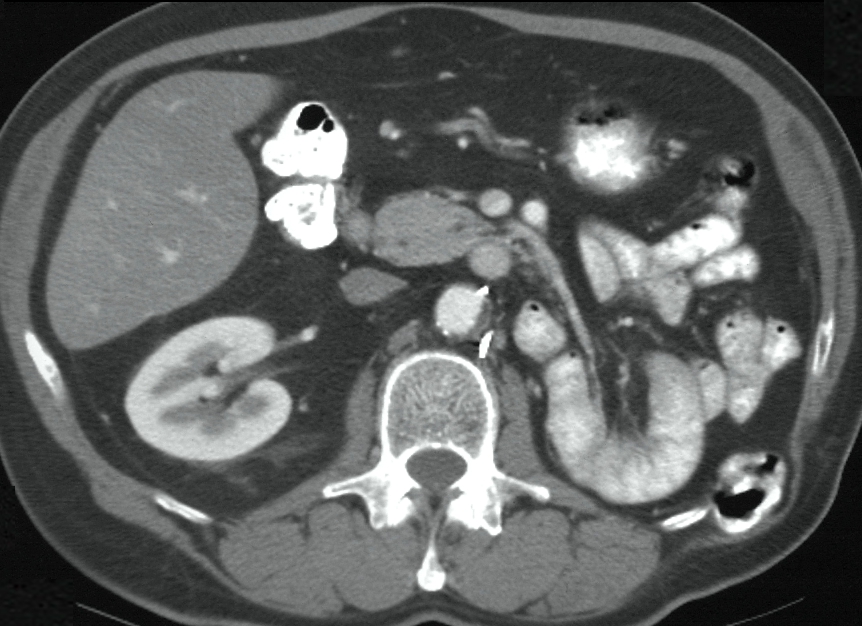
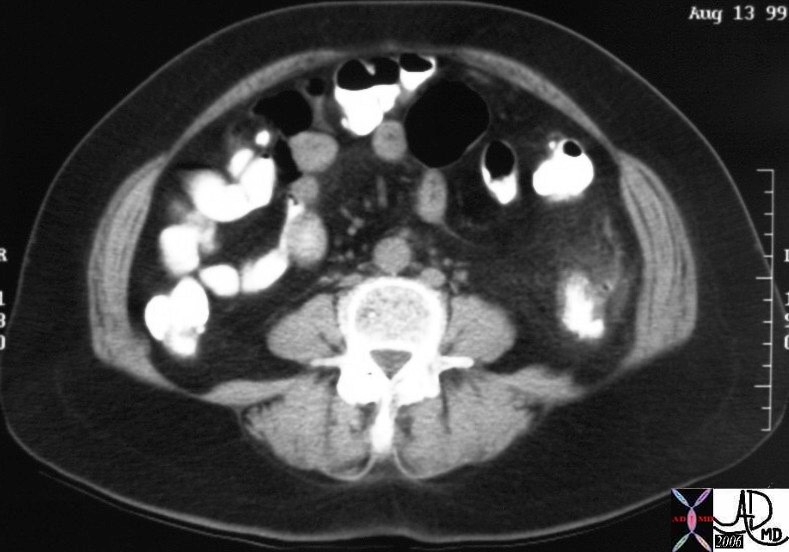
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes however the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma.. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus when we identify a large mass in the intestinal system, that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.
Appendagitis
In the opening passages of this module we described the fatty beads that hang on the outside of the colon called the appendices epiploica. We cannot usually identify the appendices epiploica since we cannot distinguish them from the other peritoneal fat that surrounds the bowel. When there is ascites, the mobile fat is displaced by the fluid and the fat attached to the bowel wall becomes apparent. In the case below the appendices epiploica of the sigmoid colon are floating in the ascetic fluid.
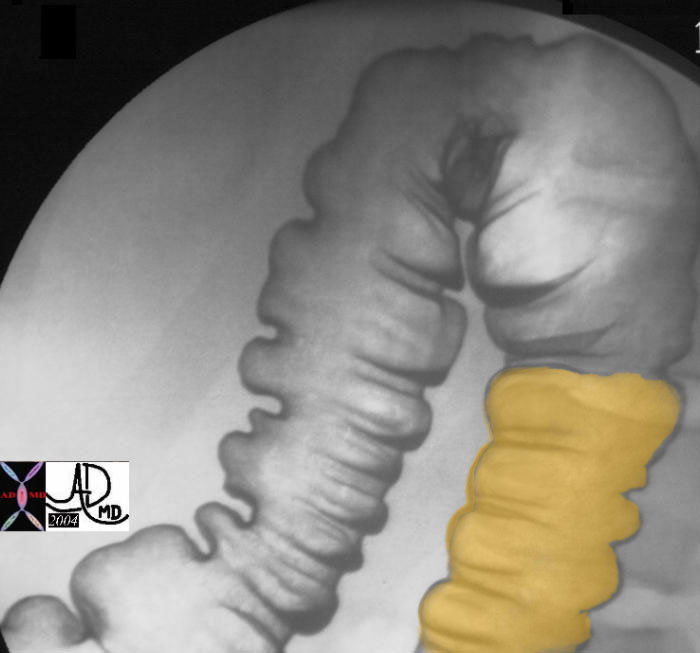
Since the appendices are mobile on a stalk and since there is continual peristalsis of the bowel, it is possible that they can twist on themselves and infarct resulting in an entity called appendagitis ? inflammation of the appendage. It is important to make this diagnosis since it is treated conservatively while uncomplicated diverticulitis that has a similar clinical presentation and a not too dissimilar radiological presentation would be treated with antibiotics. Appendagitis is characterized by a bull?s eye appearance with the fatty central area being the appendage, with a surrounding rind of inflammation and associated stranding of the pericolic fat. It is truly an ?aunt Minnie?, meaning that once seen never forgotten with the findings very characteristic of the condition.
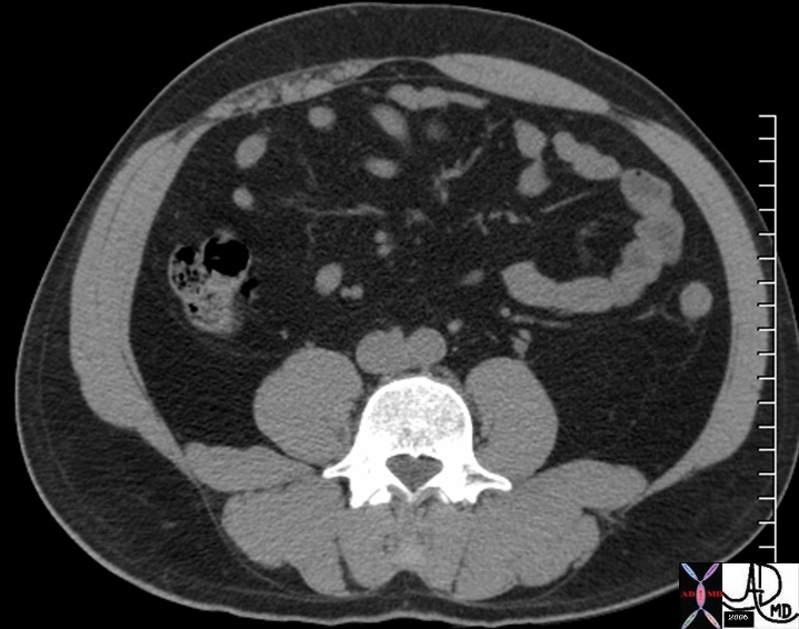
While diverticulitis is more common than appendagitis the most common site for this entity is the sigmoid colon though it can affect any part of the colon. The following case of acute diverticulitis in the descending colon has been chosen in order to contrast it with the case of appendagitis above.
Posterior abdominal wall hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.
Colonic fistula
|








DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Fistula to posterior pararenal space
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Fistula to posterior pararenal space
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Fistula to posterior pararenal space
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Fistula to posterior pararenal space
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Fistula to posterior pararenal space
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Fistula to posterior pararenal space
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Lumbar hernia following nephrectomy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lumbar hernia following nephrectomy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute diverticulitis of the descending colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute diverticulitis of the descending colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendices epiploica on descending colon – ascites
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendices epiploica on descending colon – ascites
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Lymphoma of the descending colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lymphoma of the descending colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Chronic Crohn?s disease of the colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Chronic Crohn?s disease of the colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Crohn?s disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Crohn?s disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Cobblestone changes in Crohn?s disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Cobblestone changes in Crohn?s disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Submucosal granuloma of Crohn?s disease in the colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Submucosal granuloma of Crohn?s disease in the colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 46611 colon ascending colon descending colon normal anatomy size Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 46611 colon ascending colon descending colon normal anatomy size Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Smallest part of the Colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Smallest part of the Colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Descending colon ? normal
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Descending colon ? normal
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cms in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease the most common being acute pancreatitis.
It receives its blood supply from the left colic artery and drains into the left colic vein.
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon.
Applied Anatomy
Crohn?s disease
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
Lymphoma
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes however the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma.. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus when we identify a large mass in the intestinal system, that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
Appendagitis
In the opening passages of this module we described the fatty beads that hang on the outside of the colon called the appendices epiploica. We cannot usually identify the appendices epiploica since we cannot distinguish them from the other peritoneal fat that surrounds the bowel. When there is ascites, the mobile fat is displaced by the fluid and the fat attached to the bowel wall becomes apparent. In the case below the appendices epiploica of the sigmoid colon are floating in the ascetic fluid.
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
Since the appendices are mobile on a stalk and since there is continual peristalsis of the bowel, it is possible that they can twist on themselves and infarct resulting in an entity called appendagitis ? inflammation of the appendage. It is important to make this diagnosis since it is treated conservatively while uncomplicated diverticulitis that has a similar clinical presentation and a not too dissimilar radiological presentation would be treated with antibiotics. Appendagitis is characterized by a bull?s eye appearance with the fatty central area being the appendage, with a surrounding rind of inflammation and associated stranding of the pericolic fat. It is truly an ?aunt Minnie?, meaning that once seen never forgotten with the findings very characteristic of the condition.
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
While diverticulitis is more common than appendagitis the most common site for this entity is the sigmoid colon though it can affect any part of the colon. The following case of acute diverticulitis in the descending colon has been chosen in order to contrast it with the case of appendagitis above.
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
Posterior abdominal wall hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
Colonic fistula
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] =>
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cms in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease the most common being acute pancreatitis.
It receives its blood supply from the left colic artery and drains into the left colic vein.
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon.
Applied Anatomy
Crohn?s disease
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
Lymphoma
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes however the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma.. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus when we identify a large mass in the intestinal system, that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
Appendagitis
In the opening passages of this module we described the fatty beads that hang on the outside of the colon called the appendices epiploica. We cannot usually identify the appendices epiploica since we cannot distinguish them from the other peritoneal fat that surrounds the bowel. When there is ascites, the mobile fat is displaced by the fluid and the fat attached to the bowel wall becomes apparent. In the case below the appendices epiploica of the sigmoid colon are floating in the ascetic fluid.
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
Since the appendices are mobile on a stalk and since there is continual peristalsis of the bowel, it is possible that they can twist on themselves and infarct resulting in an entity called appendagitis ? inflammation of the appendage. It is important to make this diagnosis since it is treated conservatively while uncomplicated diverticulitis that has a similar clinical presentation and a not too dissimilar radiological presentation would be treated with antibiotics. Appendagitis is characterized by a bull?s eye appearance with the fatty central area being the appendage, with a surrounding rind of inflammation and associated stranding of the pericolic fat. It is truly an ?aunt Minnie?, meaning that once seen never forgotten with the findings very characteristic of the condition.
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
While diverticulitis is more common than appendagitis the most common site for this entity is the sigmoid colon though it can affect any part of the colon. The following case of acute diverticulitis in the descending colon has been chosen in order to contrast it with the case of appendagitis above.
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
Posterior abdominal wall hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
Colonic fistula
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Fistula to posterior pararenal space
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Fistula to posterior pararenal space
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Fistula to posterior pararenal space
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Fistula to posterior pararenal space
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Lumbar hernia following nephrectomy
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lumbar hernia following nephrectomy
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute diverticulitis of the descending colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute diverticulitis of the descending colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendagitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendagitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendices epiploica on descending colon – ascites
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendices epiploica on descending colon – ascites
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Lymphoma of the descending colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Lymphoma of the descending colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Chronic Crohn?s disease of the colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Chronic Crohn?s disease of the colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Crohn?s disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Crohn?s disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Cobblestone changes in Crohn?s disease
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Cobblestone changes in Crohn?s disease
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Submucosal granuloma of Crohn?s disease in the colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Submucosal granuloma of Crohn?s disease in the colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 46611 colon ascending colon descending colon normal anatomy size Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 46611 colon ascending colon descending colon normal anatomy size Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Smallest part of the Colon
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Smallest part of the Colon
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Descending colon ? normal
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Descending colon ? normal
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 65
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cms in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease the most common being acute pancreatitis.
It receives its blood supply from the left colic artery and drains into the left colic vein.
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon.
Applied Anatomy
Crohn?s disease
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
Lymphoma
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes however the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma.. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus when we identify a large mass in the intestinal system, that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
Appendagitis
In the opening passages of this module we described the fatty beads that hang on the outside of the colon called the appendices epiploica. We cannot usually identify the appendices epiploica since we cannot distinguish them from the other peritoneal fat that surrounds the bowel. When there is ascites, the mobile fat is displaced by the fluid and the fat attached to the bowel wall becomes apparent. In the case below the appendices epiploica of the sigmoid colon are floating in the ascetic fluid.
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
Since the appendices are mobile on a stalk and since there is continual peristalsis of the bowel, it is possible that they can twist on themselves and infarct resulting in an entity called appendagitis ? inflammation of the appendage. It is important to make this diagnosis since it is treated conservatively while uncomplicated diverticulitis that has a similar clinical presentation and a not too dissimilar radiological presentation would be treated with antibiotics. Appendagitis is characterized by a bull?s eye appearance with the fatty central area being the appendage, with a surrounding rind of inflammation and associated stranding of the pericolic fat. It is truly an ?aunt Minnie?, meaning that once seen never forgotten with the findings very characteristic of the condition.
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
While diverticulitis is more common than appendagitis the most common site for this entity is the sigmoid colon though it can affect any part of the colon. The following case of acute diverticulitis in the descending colon has been chosen in order to contrast it with the case of appendagitis above.
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
Posterior abdominal wall hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
Colonic fistula
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The descending colon originates after the splenic flexure and ends at the origin of the sigmoid colon in the pelvis. By the time the stool reaches this region most of the water and retrievable products have been absorbed and the descending colon acts as a storage station. The length of the descending colon is between 10 and about 25 cm and is between 3 and 4cms in diameter. When empty it may have the same dimensions as the small bowel. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall giving it very little mobility. It takes a straight and narrow path and is given no freedom to move about the abdomen. In this location it lies in the retroperitoneum and therefore is relatively protected from intraperitoneal processes but open to the spread of retroperitoneal disease the most common being acute pancreatitis.
It receives its blood supply from the left colic artery and drains into the left colic vein.
Descending colon ? normal
Two images from a double contrast barium enema show the proximal descending colon in the first image and the distal descending colon in the second. Note that the folds do not traverse the entire diameter of the colon.
Courtesy Ashley Davidoff MD
20409b01 20410b01
Smallest part of the Colon
46611 colon ascending colon descending colon normal anatomy size Davidoff MD
Structural Differences Between the Ascending and Descending Colon as Shown by CT colonography
75365 ascending colon descending colon size character shape folds normal anatomy Ct colonography Virtual colonoscopy CTscan Courtesy Ashley Davidoff MD Scott Tsai MD
The following cases reflect diseases that can occur anywhere in the colon, but in these instances affected the descending colon.
Applied Anatomy
Crohn?s disease
Crohn?s disease is usually thought of as an inflammatory disease of the small bowel but it can affect any part of the gastrointestinal tract, and not uncommonly affects the large bowel. In the large bowel it is referred to as Crohn?s colitis or granulomatous colitis. It is called ?granulomatous? because the most specific feature of Crohn?s disease for the pathologist, whether it occurs in the large or small bowel, is the finding of a granuloma or chronic inflammatory nodule in the submucosa.
Submucosal granuloma of Crohn?s disease in the colon
This microscopic specimen is from the large bowel of a 46 year old female patient with granulomatous colitis. The granuloma demonstrated above consists of a collection of inflammatory cells (blue dots), fibrous tissue (pink strands) and a characteristic giant cell seen almost in the centre of the granuloma with pink cytoplasm and multiple blue nuclii.
Courtesy Barbara Banner MD
00670
It is important to remember that Crohn?s disease is a disease that affects all layers of the bowel wall so that in the acute stage the finding of pericolic fat involvement would be an important differentiating feature from ulcerative colitis which is a disease that usually only affects the mucosa. In the acute phases of Crohn?s there may be extensive ulceration of the mucosa so that only islands of tissue remain between the extensive ulceration. This appearance has reminded pathologists and radiologists of a cobblestone street and hence the descriptive term for this entity.
Cobblestone changes in Crohn?s disease
This pathological specimen reflects cobblestone changes in the terminal ileum in a patient with Crohn?s disease. The ?nodules? that you see are islands of normal mucosa between areas of extensive ulceration.
Courtesy Ted Gulkin MD
02477
Crohn?s disease
The transverse colon, splenic flexure and descending colon from this single contrast barium enema show a nodular mucosa which radiologists and pathologists have called cobblestone appearance.
Courtesy Ashley Davidoff MD
01921b
In the chronic phase of Crohn?s disease, fibrosis results causing shortening, loss of pliability, thickening of the wall and narrowing of the lumen. This leads to the rubber hose or lead pipe appearance.
Chronic Crohn?s disease of the colon
Longstanding Crohn?s disease in this 59 year old female patient has resulted in fibrosis with wall thickening, rigidity, luminal narrowing, and shortening of the bowel. These findings are demonstrated in the distal descending colon in this coronal reformat. ?Rubber hose? and ?lead pipe? have been descriptive phrases used by pathologists and radiologists for this appearance which can occur in ulcerative colitis as well.
Courtesy Ashley Davidoff MD
45323
Lymphoma
Lymphoma is a disease that can present with involvement of the lymph nodes in a regional manner, so that it may present for example with involvement of the nodes of the neck as the presenting site. As the disease becomes more advanced, lymph nodes in other parts of the body such as mediastinum and then nodes on the other side of the diaphragm become involved. The involvement of regional nodes is the classical form of lymphoma. Sometimes however the lymphoid tissue in the submucosa is the site of origin of the disease and this may therefore occur anywhere where lymphoid tissue resides. In the gastrointestinal system the submucosa is the site where lymphoid tissue resides and its function is to protect the body from bacteria and other potentially harmful substances that may enter from the food or fluids we ingest. These lymphocytes can become neoplastic and develop into a localized form of lymphoma.. Generally lymphoma does not incite much inflammatory reaction and since it is usually a soft mass, it only occludes structures when it is extremely bulky. Thus when we identify a large mass in the intestinal system, that does not obstruct and is not associated with significant pericolic changes in the fat, lymphoma is a prime consideration.
Lymphoma of the descending colon
The descending colon in this image shows severe thickening of the wall with the lumen still fairly well maintained and very little pericoloc stranding. The usual expected donut appearance of the colon is not present in this case telling us we are dealing with a different animal. This animal normally lives in the submucosa and when it runs amuck it is called lymphoma.
Courtesy Ashley Davidoff MD
20213
Appendagitis
In the opening passages of this module we described the fatty beads that hang on the outside of the colon called the appendices epiploica. We cannot usually identify the appendices epiploica since we cannot distinguish them from the other peritoneal fat that surrounds the bowel. When there is ascites, the mobile fat is displaced by the fluid and the fat attached to the bowel wall becomes apparent. In the case below the appendices epiploica of the sigmoid colon are floating in the ascetic fluid.
Appendices epiploica on descending colon – ascites
In this patient with ascites the appendices epiploica seem to be floating in the fluid off the anterior wall of the descending colon. Their mobility predisposes them to torsion and volvulus – an uncommon but important radiological entity called appendagitis.
Courtesy Ashley Davidoff MD
44721
Since the appendices are mobile on a stalk and since there is continual peristalsis of the bowel, it is possible that they can twist on themselves and infarct resulting in an entity called appendagitis ? inflammation of the appendage. It is important to make this diagnosis since it is treated conservatively while uncomplicated diverticulitis that has a similar clinical presentation and a not too dissimilar radiological presentation would be treated with antibiotics. Appendagitis is characterized by a bull?s eye appearance with the fatty central area being the appendage, with a surrounding rind of inflammation and associated stranding of the pericolic fat. It is truly an ?aunt Minnie?, meaning that once seen never forgotten with the findings very characteristic of the condition.
Appendagitis
The bulls eye appearance of appendagitis is typified in this case with a central area of fat representing the appendage (yellow) surrounded by a rim of inflammation (bright red) and associated induration of pericolic fat (pale red).
Courtesy Ashley Davidoff MD
39033 39033b01
While diverticulitis is more common than appendagitis the most common site for this entity is the sigmoid colon though it can affect any part of the colon. The following case of acute diverticulitis in the descending colon has been chosen in order to contrast it with the case of appendagitis above.
Acute diverticulitis of the descending colon
This CTscan of the descending colon shows significant induration of the pericolic fat, centered around a small diverticulum. The findings are classical of uncomplicated diverticulitis and the patient requires antibiotics without surgical intervention.
Courtesy Ashley Davidoff MD
28579
Posterior abdominal wall hernias
Since the descending colon is fixed in the retroperitoneum it is not usually a part of the colon that herniates, nor does it usually undergo neither volvulus nor torsion. Occasionally it may protrude into a lumbar hernia or through a surgical defect of the posterior abdominal wall such as might occur in patients who have had a nephrectomy.
Lumbar hernia following nephrectomy
The surgery for nephrectomy is via the retroperitoneum and thus the approach is through the flank. The nephrectomy in this patient has resulted in weakness of the flank muscles, and herniation of the descending colon. The small bowel has not only taken up residence in the previous bed of the left kidney but has assumed its structural identity. Is it not remarkable how closely the loop of small bowel resembles the kidney and its vessels?
Courtesy Ashley Davidoff MD
25198
Colonic fistula
Fistula to posterior pararenal space
This patient rcently had a left nephrectomy for renal cell carcinoma and inadvertant colotomy resulted in an abscess in te posterior pararenal space which is seen as gastrograffin accumulation in the right upper quadtnt Courtesy Ashley Davidoff MD
45709
Fistula to posterior pararenal space
This patient recently had a left nephrectomy for renal cell carcinoma and inadvertent colotomy resulted in an abscess in the posterior pararenal space. Contrast has been introduced into the abscess cavity by an indwelling catheter and it is seen as gastrograffin accumulation in the right upper quadrant within the psoas confines, extending into the soft tissues of the lateral abdominal wall and into the colon. The posterior relation of the kidney to the colon, requires extreme caution by the surgeon to protect the organs from each other during surgical h both being in the retroperitoneum makes surgery Courtesy Ashley Davidoff MD
25198
)