
|
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mms when empty and its length ranges from 2-10cms, but can be up to 20cms. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis. The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cms. of the ileocecal valve. If the tenia coli were easy to see on CTscan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix . These muscles are difficult to see on the CTscan.
Once the origin is identified, the body and tip of the appendix may end up posteriorly in a retrocecal position and can be superiorly directed in this position to the right, posterior or to the left of the cecum. On the other hand it may course inferiorly where it can also end up inferolaterally directly inferiorly or inferomedially. Occasionally it also found anteriorly. The appendix is retrocecal or retrocolic in about 65% of patients, pelvic in 30%, and inferior in about 4% and rarely anterior. (1%). The appendix is supplied by the appendicular artery, which is a branch of the anterior cecal artery which arises from the ileocolic artery. The appendicular artery can be found posterior to the terminal ileum where it finds its way into the mesoappendix before entering the substance of the appendix.
Each wall of the appendix can measure up to 3mms so that the total thickness (diameter) of the empty appendix should not be more than 6mms. If the wall cannot be separated from the contents then a diameter of up to 10mms is acceptable, (Benjaminov), though in practice even when the appendix does not reach these proportions the sense of the fluid filled distended appendix based on its shape and findings such as periappendiceal changes, and mucosal enhancement help clinch the diagnosis.
Applied Anatomy
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mms is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith. ( Lane )
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose. |

DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Appendicitis
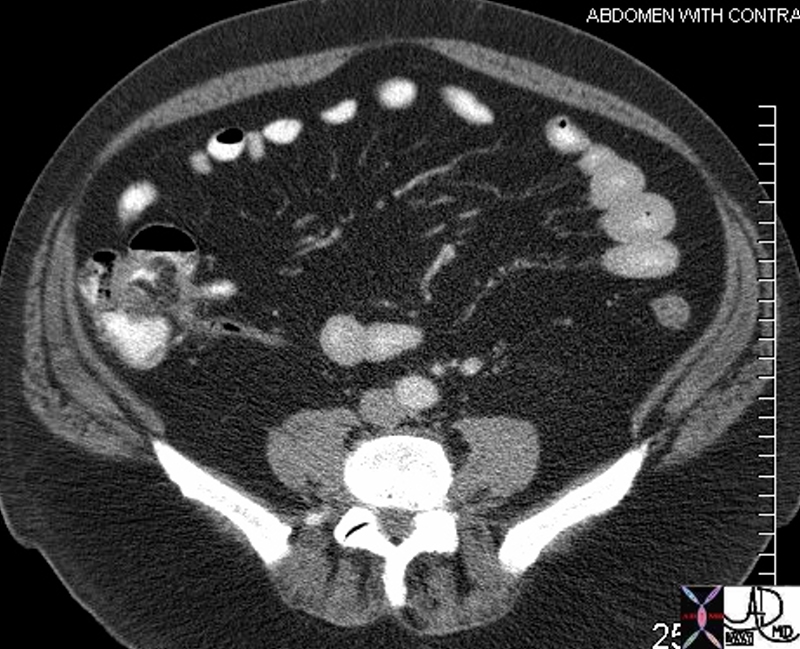
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Appendicitis
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendicitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendicitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute appendicitis
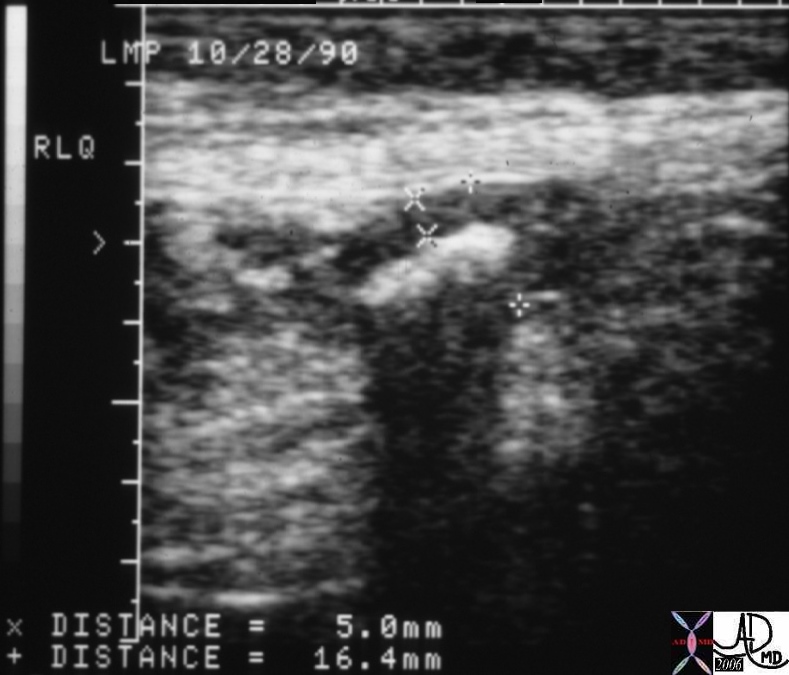
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute appendicitis
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute appendicitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute appendicitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Retrocecal appendix
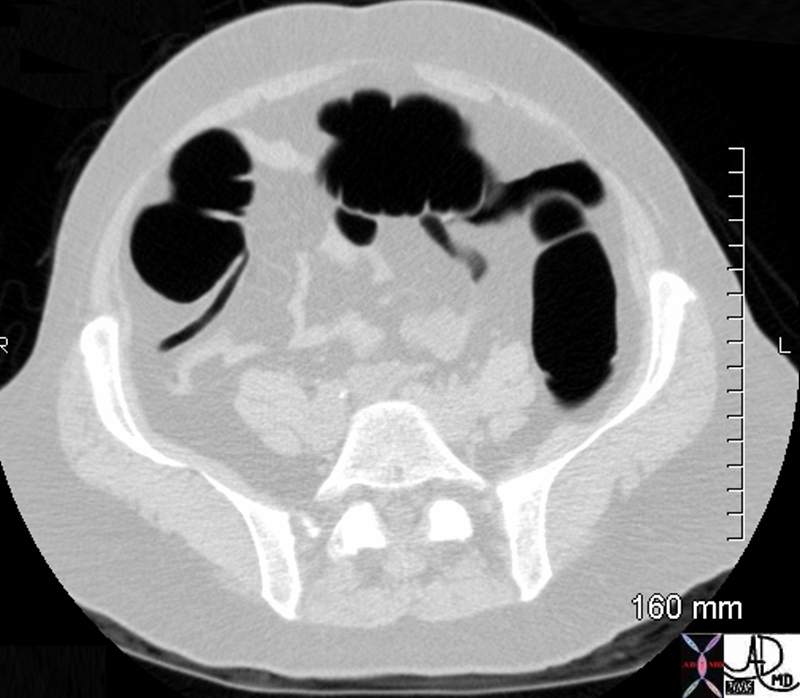
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Retrocecal appendix
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Retrocecal appendix
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Retrocecal appendix
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Appendix
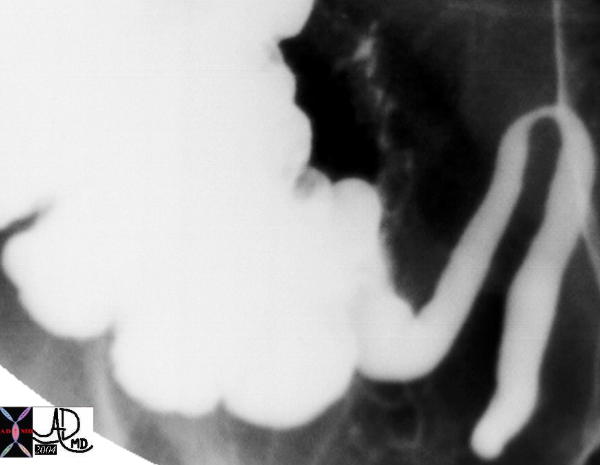
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Appendix
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Normal Appendix
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Normal Appendix
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Normal appendix and ileocecal valve.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Normal appendix and ileocecal valve.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mms when empty and its length ranges from 2-10cms, but can be up to 20cms. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis. The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cms. of the ileocecal valve. If the tenia coli were easy to see on CTscan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix . These muscles are difficult to see on the CTscan.
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
Once the origin is identified, the body and tip of the appendix may end up posteriorly in a retrocecal position and can be superiorly directed in this position to the right, posterior or to the left of the cecum. On the other hand it may course inferiorly where it can also end up inferolaterally directly inferiorly or inferomedially. Occasionally it also found anteriorly. The appendix is retrocecal or retrocolic in about 65% of patients, pelvic in 30%, and inferior in about 4% and rarely anterior. (1%). The appendix is supplied by the appendicular artery, which is a branch of the anterior cecal artery which arises from the ileocolic artery. The appendicular artery can be found posterior to the terminal ileum where it finds its way into the mesoappendix before entering the substance of the appendix.
Normal Appendix
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
Retrocecal appendix
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
Each wall of the appendix can measure up to 3mms so that the total thickness (diameter) of the empty appendix should not be more than 6mms. If the wall cannot be separated from the contents then a diameter of up to 10mms is acceptable, (Benjaminov), though in practice even when the appendix does not reach these proportions the sense of the fluid filled distended appendix based on its shape and findings such as periappendiceal changes, and mucosal enhancement help clinch the diagnosis.
Applied Anatomy
Acute appendicitis
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mms is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith. ( Lane )
Appendicitis
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] =>
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mms when empty and its length ranges from 2-10cms, but can be up to 20cms. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis. The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cms. of the ileocecal valve. If the tenia coli were easy to see on CTscan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix . These muscles are difficult to see on the CTscan.
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
Once the origin is identified, the body and tip of the appendix may end up posteriorly in a retrocecal position and can be superiorly directed in this position to the right, posterior or to the left of the cecum. On the other hand it may course inferiorly where it can also end up inferolaterally directly inferiorly or inferomedially. Occasionally it also found anteriorly. The appendix is retrocecal or retrocolic in about 65% of patients, pelvic in 30%, and inferior in about 4% and rarely anterior. (1%). The appendix is supplied by the appendicular artery, which is a branch of the anterior cecal artery which arises from the ileocolic artery. The appendicular artery can be found posterior to the terminal ileum where it finds its way into the mesoappendix before entering the substance of the appendix.
Normal Appendix
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
Retrocecal appendix
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
Each wall of the appendix can measure up to 3mms so that the total thickness (diameter) of the empty appendix should not be more than 6mms. If the wall cannot be separated from the contents then a diameter of up to 10mms is acceptable, (Benjaminov), though in practice even when the appendix does not reach these proportions the sense of the fluid filled distended appendix based on its shape and findings such as periappendiceal changes, and mucosal enhancement help clinch the diagnosis.
Applied Anatomy
Acute appendicitis
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mms is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith. ( Lane )
Appendicitis
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Appendicitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Appendicitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Acute appendicitis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Acute appendicitis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Retrocecal appendix
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Retrocecal appendix
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Normal Appendix
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Normal Appendix
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Normal appendix and ileocecal valve.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Normal appendix and ileocecal valve.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 24
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mms when empty and its length ranges from 2-10cms, but can be up to 20cms. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis. The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cms. of the ileocecal valve. If the tenia coli were easy to see on CTscan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix . These muscles are difficult to see on the CTscan.
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
Once the origin is identified, the body and tip of the appendix may end up posteriorly in a retrocecal position and can be superiorly directed in this position to the right, posterior or to the left of the cecum. On the other hand it may course inferiorly where it can also end up inferolaterally directly inferiorly or inferomedially. Occasionally it also found anteriorly. The appendix is retrocecal or retrocolic in about 65% of patients, pelvic in 30%, and inferior in about 4% and rarely anterior. (1%). The appendix is supplied by the appendicular artery, which is a branch of the anterior cecal artery which arises from the ileocolic artery. The appendicular artery can be found posterior to the terminal ileum where it finds its way into the mesoappendix before entering the substance of the appendix.
Normal Appendix
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
Retrocecal appendix
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
Each wall of the appendix can measure up to 3mms so that the total thickness (diameter) of the empty appendix should not be more than 6mms. If the wall cannot be separated from the contents then a diameter of up to 10mms is acceptable, (Benjaminov), though in practice even when the appendix does not reach these proportions the sense of the fluid filled distended appendix based on its shape and findings such as periappendiceal changes, and mucosal enhancement help clinch the diagnosis.
Applied Anatomy
Acute appendicitis
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mms is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith. ( Lane )
Appendicitis
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The appendix is a long narrow, blind ended tube that is also called the vermiform appendix because it has a worm like appearance (vermiform means worm-like in Latin). Its overall diameter is between 3-6mms when empty and its length ranges from 2-10cms, but can be up to 20cms. In the human appendix, the submucosa does contain lymphoid tissue and therefore the appendix is assumed to have a minor function within the immune system, though it has no role in digestion. It has a very narrow lumen and if this lumen becomes blocked from fecal material or due to lymphoid hyperplasia in the wall, secondary obstruction, dilatation, ischemia and infection results in the clinical entity of appendicitis. Weakening of the wall can be complicated by rupture with consequences of abscess formation or generalized peritonitis. The position of the appendix is variable and it can sometimes be very difficult to identify by CT, particularly when the normal appendix is not surrounded by fat and is instead surrounded by other loops of small and large bowel, or when the cecum itself is in an abnormal position. When the appendix is not obvious on initial perusal it is worthwhile using the more easily identified ileocecal valve with its fat laden lips as a guide, and then looking posteromedially and inferiorly for the appendix which usually lies within 2.5cms. of the ileocecal valve. If the tenia coli were easy to see on CTscan, finding the appendix in any situation would be a cinch since these longitudinal muscles all arise from around the appendix . These muscles are difficult to see on the CTscan.
Normal appendix and ileocecal valve.
This CT image shows the relative positioning of the contrast filled terminal ileum with its fat filled ileocecal valve , (anteriorly) and origin of the elongated air filled appendix (not seen in entirety ? posteriorly). The medial positioning of the ileum and posteromedial positioning of the origin of the appendix is characteristic but subject to variation.
Courtesy Ashley Davidoff MD
.44739
Once the origin is identified, the body and tip of the appendix may end up posteriorly in a retrocecal position and can be superiorly directed in this position to the right, posterior or to the left of the cecum. On the other hand it may course inferiorly where it can also end up inferolaterally directly inferiorly or inferomedially. Occasionally it also found anteriorly. The appendix is retrocecal or retrocolic in about 65% of patients, pelvic in 30%, and inferior in about 4% and rarely anterior. (1%). The appendix is supplied by the appendicular artery, which is a branch of the anterior cecal artery which arises from the ileocolic artery. The appendicular artery can be found posterior to the terminal ileum where it finds its way into the mesoappendix before entering the substance of the appendix.
Normal Appendix
This image reflects a large vermiform appendix filled from a single contrast barium enema. Its inferomedial origin is characteristic while the body and tip have an unpredictable course as seen in this image.
Courtesy Ashley Davidoff MD
20411
Retrocecal appendix
This transverse image from a virtual colonoscopy is a beautiful demonstration of an air filled worm like, retrocecal appendix.
Courtesy Ashley Davidoff MD
44756
Each wall of the appendix can measure up to 3mms so that the total thickness (diameter) of the empty appendix should not be more than 6mms. If the wall cannot be separated from the contents then a diameter of up to 10mms is acceptable, (Benjaminov), though in practice even when the appendix does not reach these proportions the sense of the fluid filled distended appendix based on its shape and findings such as periappendiceal changes, and mucosal enhancement help clinch the diagnosis.
Applied Anatomy
Acute appendicitis
This 50year old female presented with acute RLQ pain. The ultrasound demonstrates a wall that is 5mm thick and an overall luminal size of 16.4mms. Shadowing from luminal contents originated from an appendicolith. Additional findings of probe tenderness and non compressibility made the diagnosis pathognomonic for acute appendicitis.
Courtesy Ashley Davidoff MD
01074
CT scanning is highly sensitive and specific for the entity of appendicitis. Periappendiceal stranding is the most specific sign occurring in 100% of patients with the disease, while thickening of greater than 6mms is also sensitive (93%) and specific (100%) (Rao). The finding of appendicoliths on the other hand does not necessarily imply acute appendicitis, but is often associated with the acute condition. A stone stuck in the distal right ureter can sometimes masquerade as an appendicolith. ( Lane )
Appendicitis
The classical findings of appendicitis are characterized by an appendix that is distended with fluid measuring greater than 6mm, (red overlay) enhancing mucosa, mass effect by periappendiceal edema on the cecum (green), and induration of the mesoappendix.(yellow)
Courtesy Ashley Davidoff MD
44763 44763 b01
In humans the appendix is a vestigial structure, while in obligate herbivores the appendix is large, allowing it to participate in the fermentation process of cellulose.
)