Assistant
Ankle Joint Definition
By: Gregory R. Waryasz, MD
The ankle joint of the musculoskeletal system is characterized by connecting the lower leg to the foot. It is also known as the talocrural articulation.
It is part of the lower extremity and consists of bone, skeletal muscle, cartilage, synovial tissue, and tendon.
Its unique structural is that it is a hinge-type joint. It is located between the distal tibia and fibula and the superior talus.
The bones are the tibia, fibula, and talus. The tibia?s medial malleolus and the fibula?s lateral malleolus make up the ankle mortise for articulation with the talus.
The ligaments are the anterior talofibular ligament, posterior talofibular ligament, calcaneofibular ligament, medial/deltoid ligament, and the syndesmotic ligaments.
The superior and inferior extensor retinaculum are located on the anterior surface of the ankle.
The blood supply is from the malleolar branches of the fibular, anterior tibial, and posterior tibial arteries.
The innervation is from the nerves supplying the muscles going across and that act at the joint according to Hilton?s Law. The ankle is supplied by the tibial and the deep fibular/peroneal nerve.
The ankle joint?s components as well as all other bones, muscles, and ligaments of the body are derived of mesodermal origin in the embryo.
The function of the ankle is to move the foot along with the subtalar joint. This allows for fluid gait. The ankle joint moves mainly with dorsiflexion and plantarflexion. There is also some ?wobble? including abduction, adduction, inversion, and eversion. Inversion and eversion are mostly from the subtalar joint. (talocalcaneneal joint).
Dorsiflexion of the ankle is produced by the muscles of the anterior compartment including the tibialis anterior, extensor digitorum longus, and extensor hallucis longus.
Plantarflexion of the ankle is accomplished by the posterior compartment muscles. These muscles are the gastrocnemius, soleus, flexor hallucis longus, flexor digitorum longus, and the tibialis posterior.
Common diseases of the ankle joint include arthritis, tendinitis, fractures, stress fractures, dislocation/subluxation, septic arthritis, osteomyelitis, Charcot joint, osteochondral lesions, clubfoot, calcaneovalgus foot, congenital vertical talus, anterior impingement syndrome, and osteoporosis.
Arthritis can be from osteoarthritis, post-traumatic arthritis, rheumatoid arthritis, juvenile idiopathic arthritis, or seronegative arthritis.
Fractures can occur with the femur, patella, fibula, or tibia.
Clubfoot (Talipes Equinovarus) is associated with shortened and contracted soft tissue structures that lead forefoot adduction (towards the midline), hindfoot varus (bowing/angled inward), and a talus in equinus (plantarflexion). It is seen in approximately 1 in 750 live births.
The calcaneovalgus foot is typically the result of positioning of the fetus in utero. The foot has a dorsiflexed hindfoot with eversion (turning outward) and abduction (away from the midline) of the hindfoot.
Congenital vertical talus is also known as “Rocker-Bottom” foot due to its rounded appearance. The shape of the foot is similar to a wheel. The condition is associated with neurologic and chromosomal disorders (including Edward’s Syndrome/Trisomy 18).
Charcot joint refers to neurogenic arthropathy. There is a nerve injury that leads to destruction of a joint. It can occur due to neurosyphilis, diabetes, syringomyelia, spinal cord injury, pernicious anemia, leprosy, and peripheral nerve injury.
Osteochondral defects can occur after trauma most commonly. Average age of patients with this condition is between 20-35 yrs.
Osteochondritis dissecans is an osteochondral defect with partial or complete separation of a bone fragment.
Anterior impingement syndrome of the ankle is a condition of either soft tissue or bony impingement. Soft tissue impingement can be due to chronic instability from ankle sprains. Bony impingement can result from an anterior tibiotalar spur, extreme dorsiflexion during activities such as ballet impinging the tibia on the talar neck, a natural sulcus, or the formation of exostoses (new bone formation).
Transient synovitis or toxic synovitis is joint pain after a recent viral illness or trauma. It is a self-limiting condition of children ages 3 to 8 years.
Lyme Arthritis is a condition common in the northeast USA where there is a rheumatologic reaction to Borrelia burgdoferi. It occurs after the patient is bitten by a tick.
Osteomyelitis is an infection of the bone typically caused by a bacteria.
Septic arthritis is an infection of the synovial tissue of the joint with pus in the joint cavity. The infection is capable of rapidly destroying the joint.
Commonly used diagnostic procedures include clinical history, physical exam, x-ray, CT, and MRI. Ultrasound can be used to help with diagnosis of effusion and synovial thickening.
It is usually treated with rest, NSAIDs, physical therapy, and surgery. Septic arthritis is treated with surgical washout and antibiotics. Arthritis and fractures can be treated with surgery including total knee replacement. Osteoporosis is treated with bisphosphonates, calcitonin, calcium, and vitamin D. Transient synovitis is treated with NSAIDs. Lyme Arthritis requires treatment with antibiotics. Clubfoot and calcaneovalgus deformities are treated non-operatively initially. Charcot joint is treated by total contact casting (TCC) and treating the underlying condition.
References
Davis MF, Davis PF, Ross DS. Expert Guide to Sports Medicine. ACP Series, 2005.
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless? Textbook of Orthopaedics: Ankle Joint Menu (http://www.wheelessonline.com/ortho/ooa1/10.htm)

46714b02 |
| 46714b02 bone foot feet heel ankle joint calcaneus talus navicular cuneiform cuboids tarsals tarsal bones tibia fibula lateral X-ray plain film Davidoff MD labelled |

 71844c02.800 71844c02.800 |
| 71844c02.800 bone ankle tibia fibula medial maleolus lateral malleolus talus calcaneus tarsal bones os trigonum plain X-Ray Courtesy Ashley Davidoff MD |
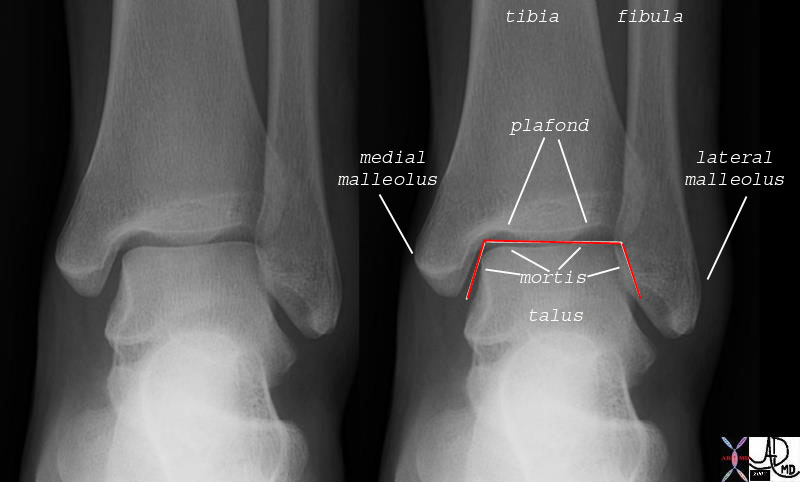
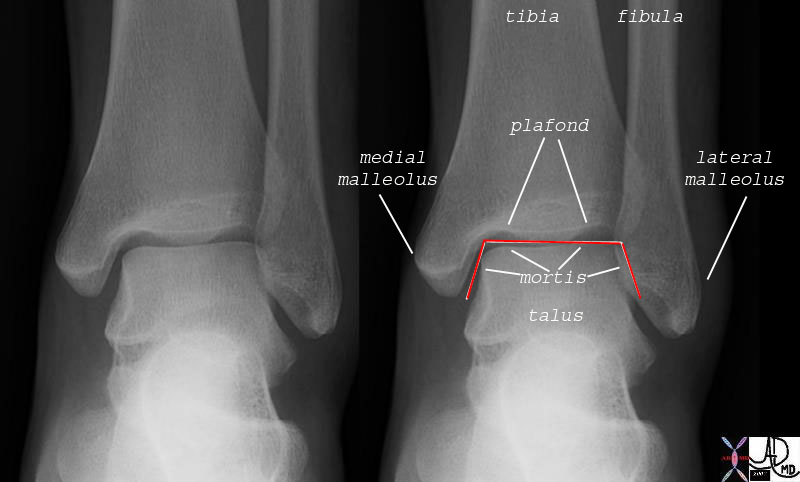 71842c02 71842c02 |
| 71842c02 bone ankle joint tibia fibula lateral malleolus medial malleolus tibitalar joint plafond mortis plain X-ray A-P Courtesy Ashley DAvidoff MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
71842c02
71842c02 bone ankle joint tibia fibula lateral malleolus medial malleolus tibitalar joint plafond mortis plain X-ray A-P Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
71842c02
71842c02 bone ankle joint tibia fibula lateral malleolus medial malleolus tibitalar joint plafond mortis plain X-ray A-P Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71842c02 bone ankle joint tibia fibula lateral malleolus medial malleolus tibitalar joint plafond mortis plain X-ray A-P Courtesy Ashley DAvidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71842c02 bone ankle joint tibia fibula lateral malleolus medial malleolus tibitalar joint plafond mortis plain X-ray A-P Courtesy Ashley DAvidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71842c02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71842c02
)
https://beta.thecommonvein.net/wp-content/uploads/2023/06/71842c02.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
71844c02.800
71844c02.800 bone ankle tibia fibula medial maleolus lateral malleolus talus calcaneus tarsal bones os trigonum plain X-Ray Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
71844c02.800
71844c02.800 bone ankle tibia fibula medial maleolus lateral malleolus talus calcaneus tarsal bones os trigonum plain X-Ray Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71844c02.800 bone ankle tibia fibula medial maleolus lateral malleolus talus calcaneus tarsal bones os trigonum plain X-Ray Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71844c02.800 bone ankle tibia fibula medial maleolus lateral malleolus talus calcaneus tarsal bones os trigonum plain X-Ray Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 71844c02.800
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 71844c02.800
)
https://beta.thecommonvein.net/wp-content/uploads/2023/06/71844c02.800.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
46714b02
46714b02 bone foot feet heel ankle joint calcaneus talus navicular cuneiform cuboids tarsals tarsal bones tibia fibula lateral X-ray plain film Davidoff MD labelled
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
46714b02
46714b02 bone foot feet heel ankle joint calcaneus talus navicular cuneiform cuboids tarsals tarsal bones tibia fibula lateral X-ray plain film Davidoff MD labelled
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 46714b02 bone foot feet heel ankle joint calcaneus talus navicular cuneiform cuboids tarsals tarsal bones tibia fibula lateral X-ray plain film Davidoff MD labelled
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 46714b02 bone foot feet heel ankle joint calcaneus talus navicular cuneiform cuboids tarsals tarsal bones tibia fibula lateral X-ray plain film Davidoff MD labelled
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
46714b02
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
46714b02
)
