
Hi Prashanth
SARCOIDOSIS, a SCARE, CHEST PAIN and an OCTOPUSRe “Sarcoidosis, a Scare, Chest Pain and an Octopus”
This is a story about a 59 year old woman who had sarcoidosis, who had a scare developed chest pain that sounded like acute coronary syndrome and was short of breath
Your part is to review our patient CXR CT MRI in 4 minutes!
Below is now the stream lined version of your part and the aim is for you to use the presentations of previous participants to decide whether the CXR is CHF or sarcoidosis, interpret the CT and angios, and then the MRI
Coming before you are;
Will who is doing CXR and Sarcoid
Michael CHF
Hoon – Chest sarcoidosis and CT
Pedro cardiac sarcoidosis and MRI
Maryam normal coronary anatomy
Let me know about any reservations or questions
Thanks
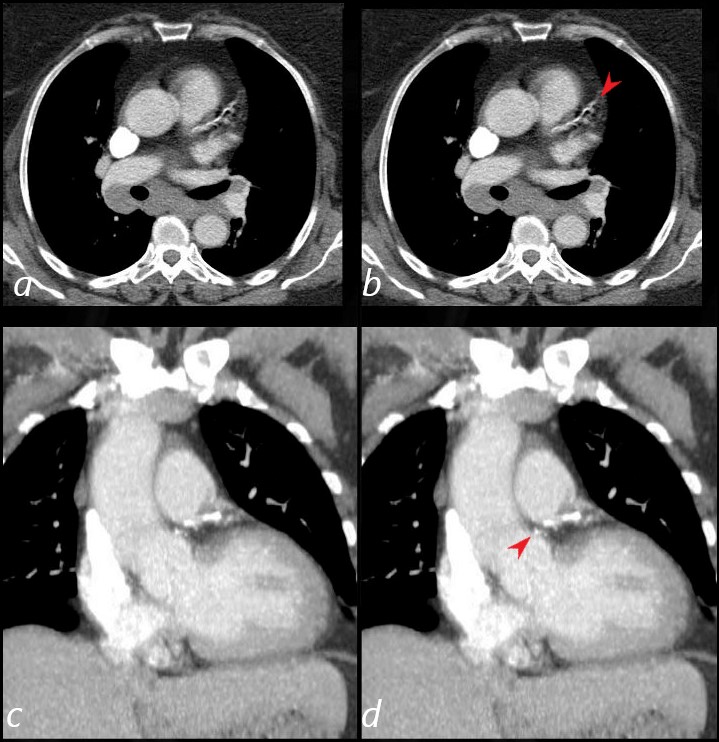
59-year-old female with a history of sarcoidosis (cutaneous, ocular and pulmonary).
Solid nodules along right major fissure and subpleural nodules anterior lingula in characteristic location
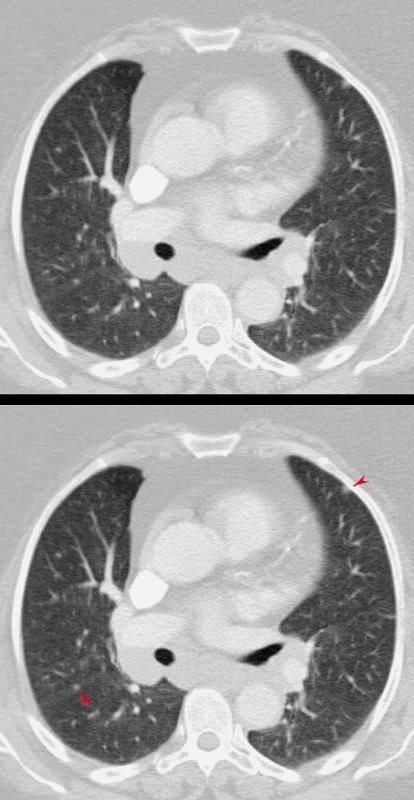 PLEURAL and FISSURAL BASED LUNG NODULES (red arrows)
PLEURAL and FISSURAL BASED LUNG NODULES (red arrows)
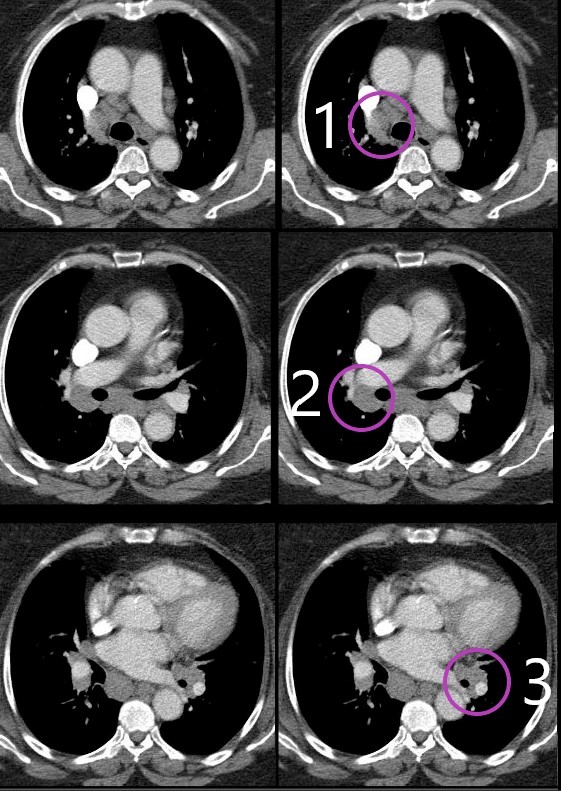
Chest CT showed multiple non calcified nodules.
Right Sided Centrilobular Nodules and Left Major Fissure Nodule
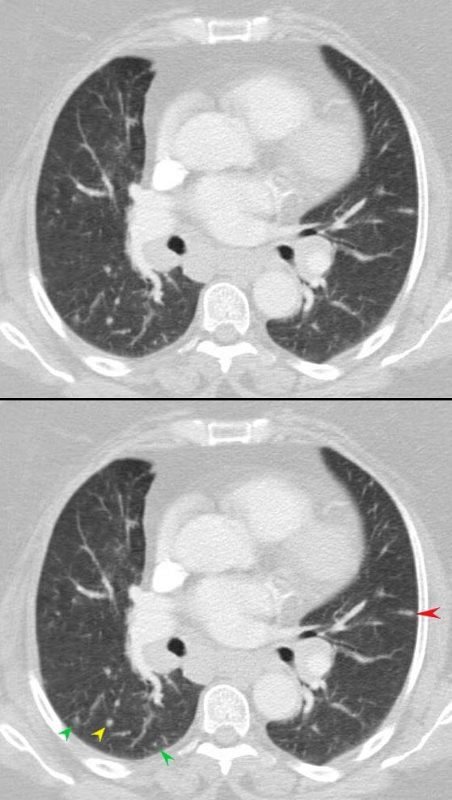 CENTRILOBULAR NODULE (green arrow) PARENCHYMAL NODULE (yellow) and FISSURAL NODULE (red arrow)
CENTRILOBULAR NODULE (green arrow) PARENCHYMAL NODULE (yellow) and FISSURAL NODULE (red arrow)
Pawnbrokers Sign – 1,2,3 Sign
Bilateral hilar adenopathy is most common and usually symmetric (50 percent of cases) or the right may be slightly more prominent . Unilateral adenopathy is uncommon (<5 percent of cases).
CAD
 CORONARY CALCIFICATION including L MAIN
CORONARY CALCIFICATION including L MAIN
Her current presentation;
1 hour of substernal chest pain, associated with dyspnea, precipitated by an encounter with the police who needed to search her house.
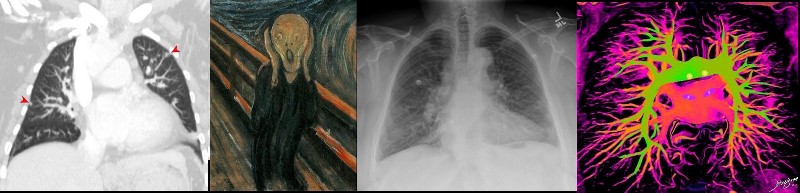
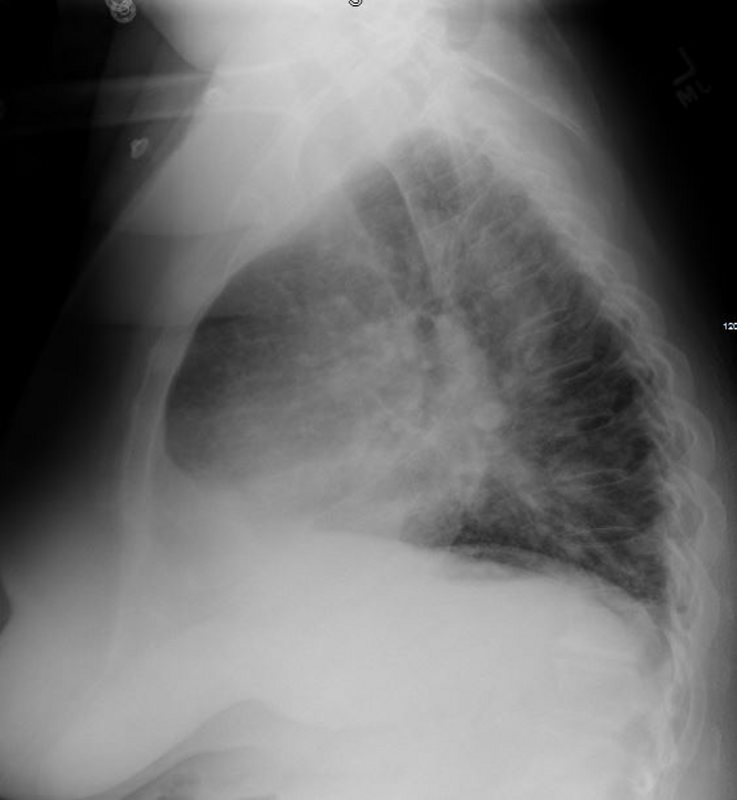
CXR
CHF or Stage II Sarcoidosis?

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CHF and CXR or Sarcoidosis and CXR as per prior discussion
Is the LA Enlarged?

Ashley Davidoff MD
Is it an LA with a 10 mmHg, 20 mmHg or 30 mmHg pressure
1 – Is the PA>Bronchus in the middle or upper lobe vessels or is there redistribution ?
2- Is there fuzziness to the vessels?
3- Is there alveolar edema?
Impression
LAE and suspect LVEDP between 20-30 mmHg
Could this be Sarcoid ?
Carinal angle widened could be from adenopathy
Redistribution seems real
Lumpy Bumpy Hila with known adenopathy
CT showed no ILD
Is the LV enlarged?
 LVE – > 50% of hemidiaphragm occupied by the LV
LVE – > 50% of hemidiaphragm occupied by the LV
Echo showed EF of 50% and apical hypokinesis.
EKG showed ST elevation in V4 and V5.
Mildly elevated Troponins
CT had shown LAD atherosclerotic calcifications
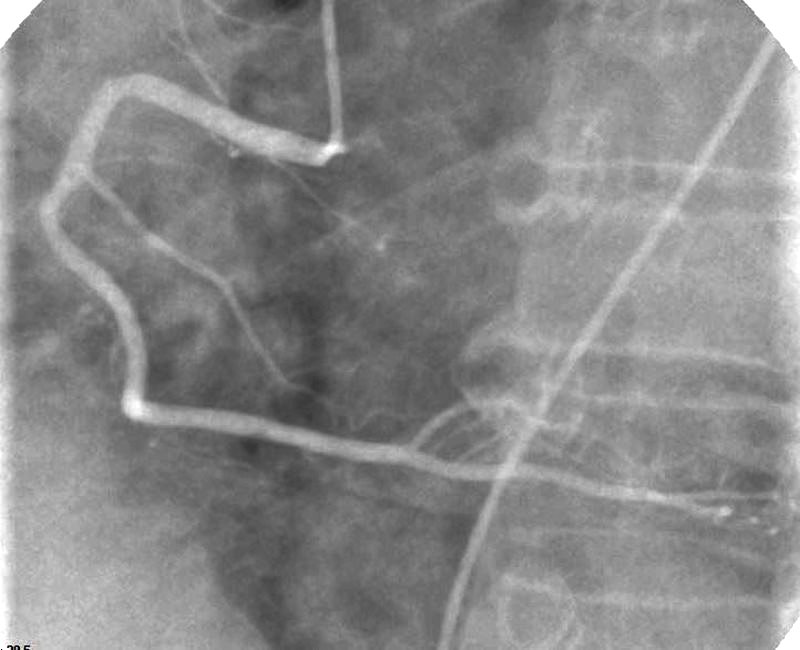
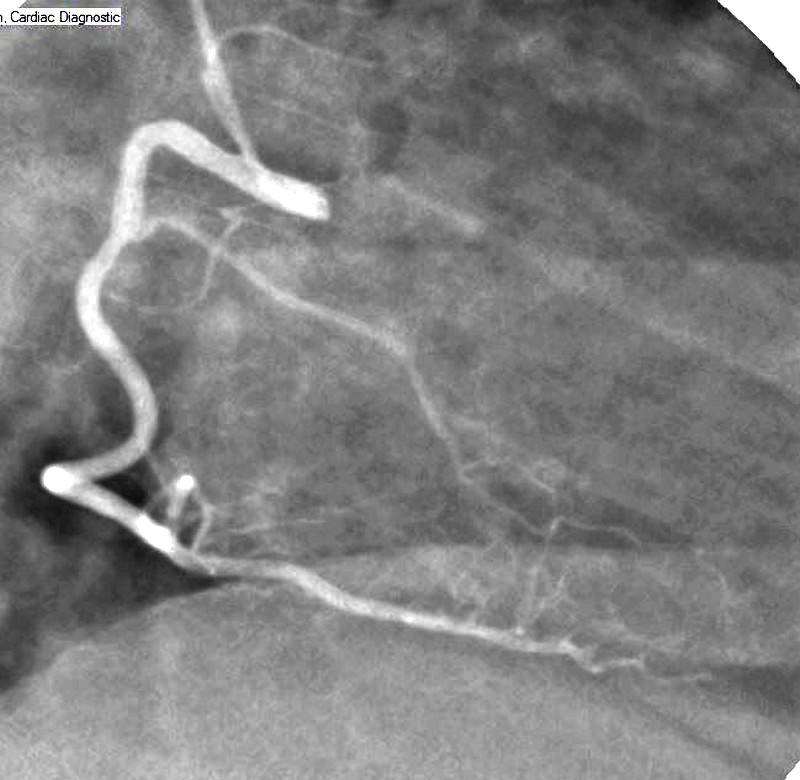
Cath
Elevated troponin necessitated cardiac cath which showed normal coronaries.
LAD identified by the septal arteries coursing toward the diaphragm
SA nodal off the proximal circumflex (60%)
Right dominant system

Ashley Davidoff MD
RAO LAD septal and diagonals arteries – Normal

Ashley Davidoff MD
LAO – Infundibular artery to RVOT, small anterior RV vessel, acute marginal, PDA and posterior LV branches
 LAO – NORMAL RCA
LAO – NORMAL RCA
RAO Infundibular (RVOT) , acute marginal, PDA septal vessels and posterior LV branches
Ashley Davidoff MD
Classical Takotsubo Heart

TAKO TSUBO = CRAB TRAP
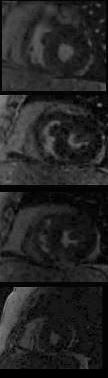
T2 Apical Edema
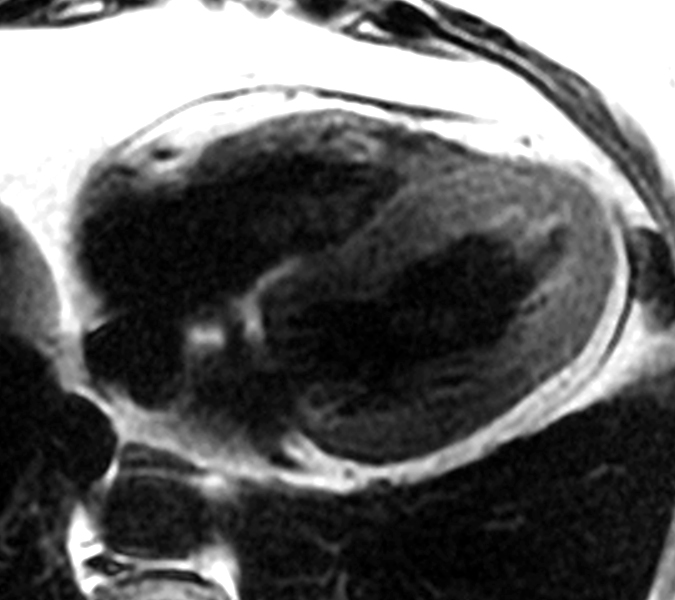
TAKOTSUBO CARDIOMYOPATHY –
Ashley Davidoff MD
Mild Apical Hypokinesis and Midventricular Hyperkinesis
LGE
Suboptimal study but no obvious ischemic disease
Ashley Davidoff MD
Thus this lady has a diagnosis of sarcoidosis (ocular skin and likely pulmonary)and Takotsubo cardiomyopathy precipitated by an acute emotional stress when the police visited her home looking for men in her basement.

She presented with acute coronary syndrome, ST segment changes on EKG, mildly elevated troponins, CHF on CXR, with normal coronary arteriography and LV gram characteristic of Takotsubo cardiomyopathy