

Re “Sarcoidosis, a Scare, Chest Pain and an Octopus”
This is a story about a 59 year old woman who had sarcoidosis, who had a scare developed chest pain that sounded like acute coronary syndrome and was short of breath
Your part is to teach about sarcoidosis of the heart in 4 minutes!
The content is now on your page below
I am still in the process of streamlining your part but in essence it
The key I think is to know and teach that sarcoidosis and the lymphatic system go hand in hand ? Secondly that sarcoidosis loves to coalesce ? granulomas become micronodules ? which cluster and coalesce (good buzz words) and things get bigger and more dense downstream and hence the subepicardial and superficial location of the disease
There is a parallel with the pathogenesis of sarcoidosis in the chest ? See Hoon’s presentation
Please see Hoons presentation on the lung that has similar principles regarding pathogenesis of the disease
Let me know about any reservations
Thanks
AD
In a Nutshell
-
- Can affect any chamber of the heart but most commonly LV
- Follow Lymphatics (Go with the flow) starting at
-
- patchy nodular mid multifocal and epi
- predominantly in the subepicardial areas,
- Also myocardial, and least common subendocardial
- most characteristic free wall and basal septum (conduction)
- patchy nodular mid multifocal and epi
-
- Follow Lymphatics (Go with the flow) starting at
- Can affect any chamber of the heart but most commonly LV
Cardiac sarcoidosis (CS)detected in 20-30% of patients with sarcoidosis (up to 55% in Japanese population) and more than 20% of the cases of sarcoidosis are clinically silent. Complete heart block, bundle branch block, ventricular tachycardia (VT), congestive heart failure (HF), and sudden death are common presentations in CS
- No portion of the heart is immune to infiltration by sarcoid granulomas. The granulomas may involve the
- myocardium,(most common)
- pericardium, and
- endocardium
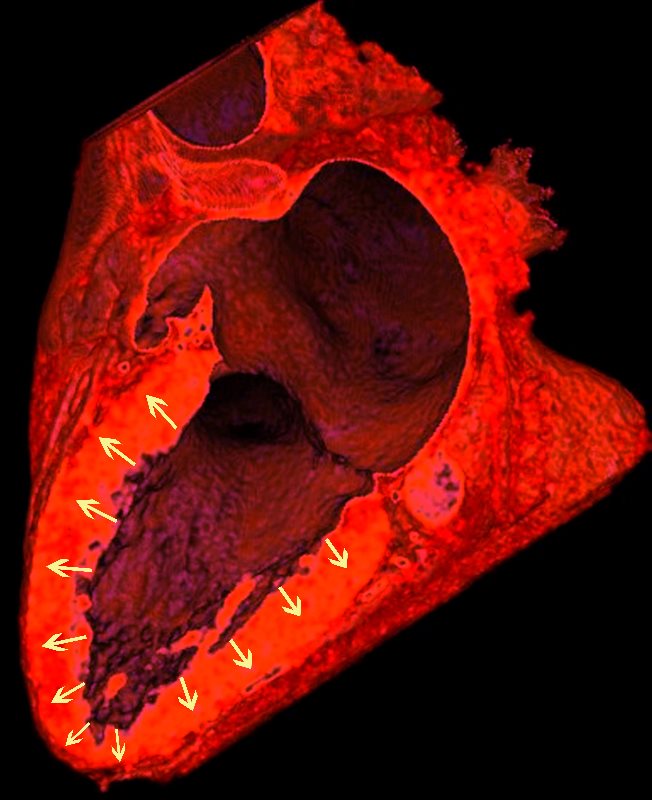
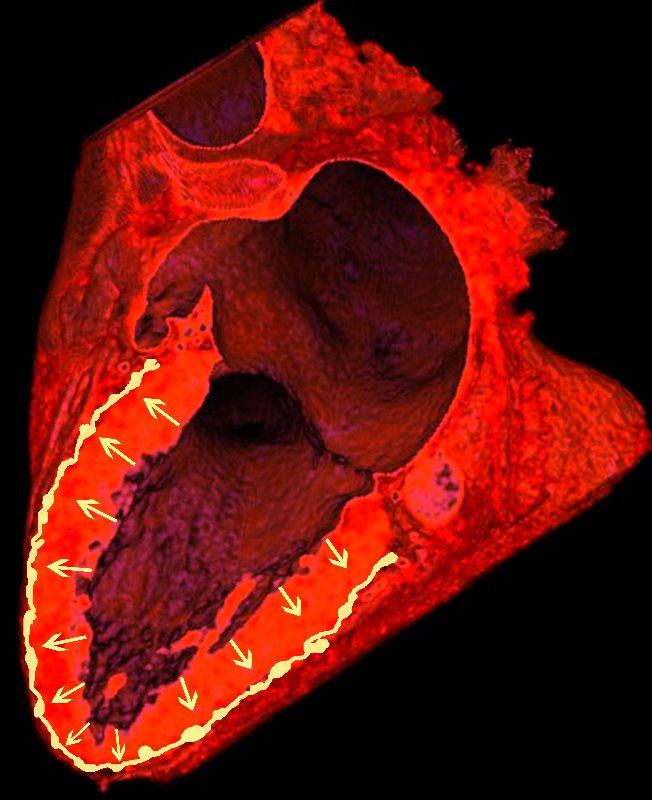
THE ?S? OF SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which has its epicenter in the lymphoid tissue of the heart starting att the “s”urface o the heart in the “s”ubepicardial layer .
The ?S? for sarcoidosis drawn on the heart starting superficially in the subepicardial layer and then flowing with the lymphovacsular bundle all in close association with the nervous system of the heart
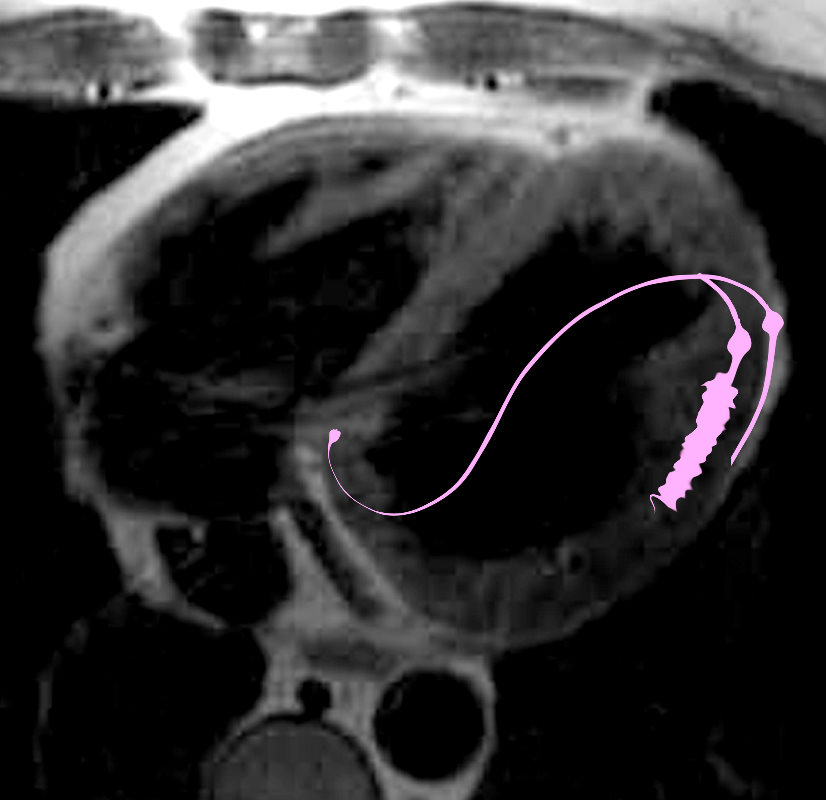
NORMAL LYMPHATIC DRAINAGE
Lymphatics run from the subendocardium through the myocardium to the subendocardial layer where they accumulate in subendocardial plexuses
{kind=link}
{kind=link}
{kind=link}
The subendocardial plexuses drain into lymphatics which accompany the coronary arteries which then drain into mediastinal nodes
{kind=link}

The lymph drains from the subendocardium through the myocardium where it collects in subendocardial plexuses and then into lymphatic vessels which travel along with the LAD
Ashley Davidoff MD
SARCOIDOSIS
LV
The ?S? of Sarcoidosis
- Starting superficially in subepicardial regions of
- lateral free wall as well as
- medial basal septum
- but also mid myocardial with
- linear patchy and nodular forms.
Biventricular involvement is common
{kind=link}
The hallmark of cardiac sarcoidosis is LGE involving subepicardial regions of lateral free wall as well as medial basal septum but also mid myocardial with linear patchy and nodular forms.
Biventricular involvement is common
Ashley Davidoff MD
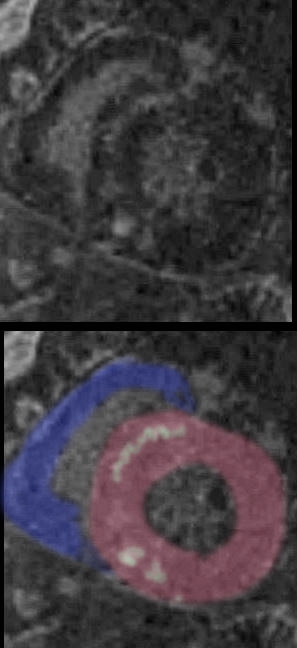
The most common involvement observed on MRI is the subepicardial layer (green) -manifesting nodular, patchy regions of LGE
 NODULAR AND LINEAR SUBEPICARDIAL INVOLVEMENT
NODULAR AND LINEAR SUBEPICARDIAL INVOLVEMENT
The hallmark of cardiac sarcoidosis is LGE involving subepicardial regions of lateral free wall as well as medial basal septum but also mid myocardial with linear patchy and nodular forms.
Biventricular involvement is common
Ashley Davidoff MD
{kind=link}
Mid Myocardial – Nodular Patchy
{kind=link}

Ashley Davidoff MD
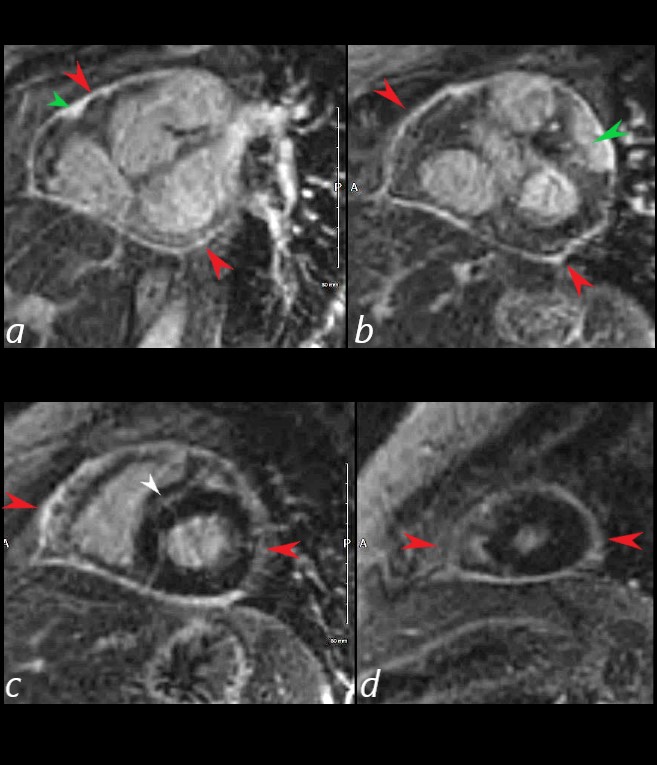
Clinical Examples
69 year old male presented with history of cardiomyopathy and atrial fibrillation The findings on MRI are highly suggestive of sarcoidosis. There are multicentric foci of LGE in linear and nodular form in the mid myocardial and subepicardial layers and likely in the pericardium and myocardium of the right ventricle.
There was associated global hypokinesis of the LV with an EF of 40%, and increase in the LV mass of 120gms/ sq m
LGE – Subepicardial Nodular Patchy
{kind=link}
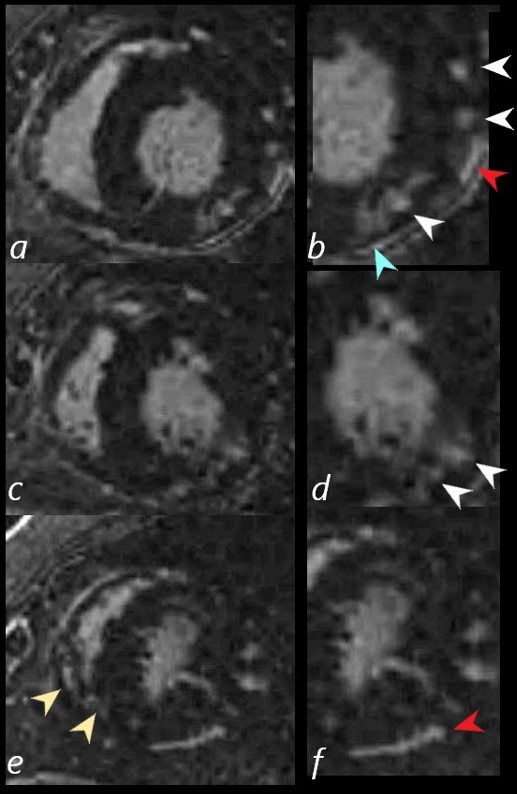
There are multicentric foci of LGE nodular form in the mid myocardial region (white arrowheads) linear LGE in the subepicardial layers (red arrowheads, b and f) in the pericardium (teal blue arrowhead) and myocardium of the right ventricle (yellow arrowhead e).Ashley Davidoff MD
{kind=link}
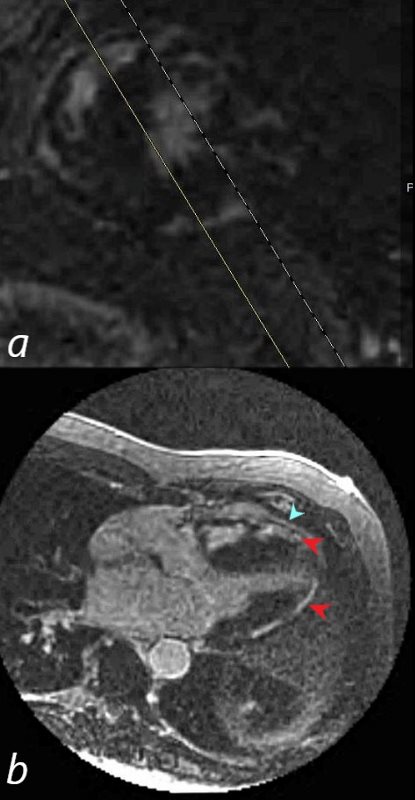
69-year-old male presented with history of cardiomyopathy and atrial fibrillation
In this series the long axis 3 chambered view reveals intense continuous sub epicardial disease (red arrowheads) and pericardial LE (teal blue arrowhead)
Ashley Davidoff MD
Medial Basal Septal – near the Conduction System – Nodular Patchy (green)

Ashley Davidoff MD
Heart Block and CHF
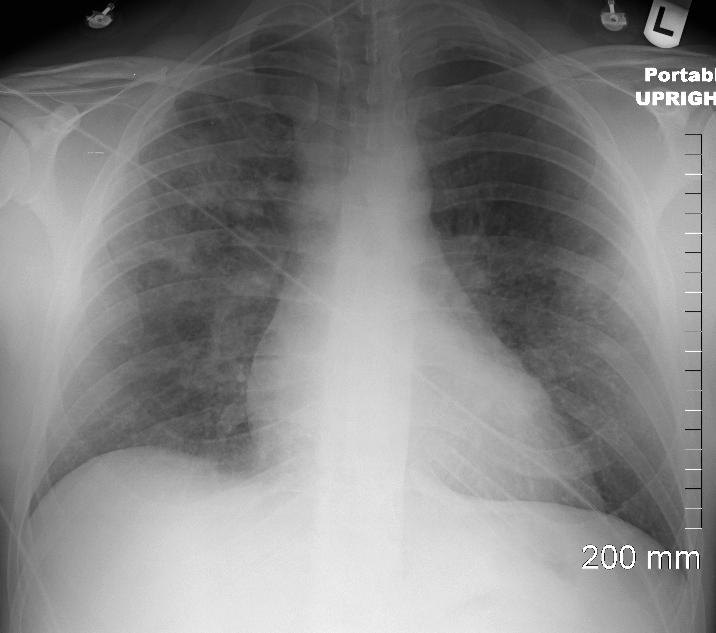
34-year-old male who was diagnosed with pulmonary sarcoidosis 1 year before, presents with progressive dyspnea over 6 months, previously able to run 5 miles per day and currently limited to walking short distances. Clinical evaluation revealed that he was in complete heart block with a heart rate of 35 /min. EKG showed a rate of 40 with AV dissociation with alternating junctional and ventricular escape rhythms.
CXR showed upper lobe predominance interstitial changes, slightly more prominent on the right side. There was evidence of CHF with enlargement of the LA (widening of the carinal angle) and cephalization of the vessels
An echocardiogram was normal with normal ejection fraction.
MRI revealed normal cardiac function, mild left atrial enlargement, and diffuse almost circumferential subendocardial enhancement of the LV, most prominent in the lateral wall. There was also a linear focus in the mid myocardium in the anterior region medially near the septum
A dual lead pacemaker was placed and follow up CXR showed improved CHF an persistent interstitial findings dominant in the upper lobes consistent with sarcoidosis.
Follow up CXR 7 years later showed a normal CXR. The pacemaker had been removed and the interstitial process had resolved
Ashley Davidoff MD
Improved CHF following Pacemaker Placement

Ashley Davidoff MD
Pericardial Involvement Distinctly Uncommon – Sarcoidosis in general is a “dry” disease Despite involvement of heart tissue close to the pericardium and for that matter pleura, effusions are very uncommon
{kind=link}
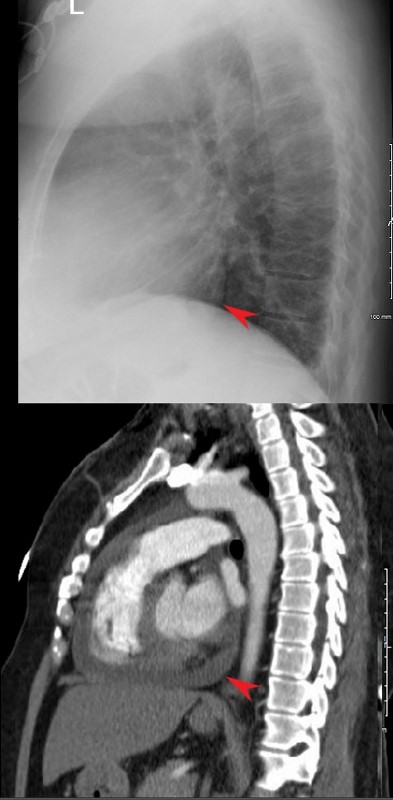
RECURRENT PERICARDIAL EFFUSION CXR,CT CORRELATION
The lateral examination soft pericardial effusion layering dependently and posteriorly.Ashley Davidoff MD
{kind=link}
The short axis LGE sequence starting at the base of the heart (a, b) progressing through the body (c) and apex (d) shows focal LGE in the RVOT(a, green arrowhead) and in the LV (b green arrowhead) extensive pericardial enhancement (a,b,c,d ? red arrowheads, and in the septum (white arrowhead c).
54-year-old female with peripheral adenopathy who had an inguinal node biopsied 6 years prior showing sarcoidosis.Chest examinations at the time showed little evidence of sarcoid except for a few small nodules. She has a history of hypertension COPD; sleep apnea, on CPAP; diabetes mellitus, on metformin; lumpectomy x2; GERD; and vertigo
4 years ago she presented with SOB and was noted to have a pericardial effusion by echo without tamponade
The pericardial effusion was drained with negative cytology and negative for TB. CT at the time following the drainage showed a thickened pericardium with pericardial drain in place
She represented 1 year later with symptoms of worsening intermittent chest pain, and shortness of breath exacerbated with exertion. An echocardiogram, showed recurrent increasing pericardial effusion confirmed by CT. She was placed on steroids but did not tolerate the steroids.
Later in that year she underwent surgery for pericardial window and VATS biopsy of her left lower lobe. Her pericardium was noted to be thickened
Pathology revealed Non-necrotizing granulomatous inflammation involving pulmonary interstitium and occasional airways; AFB, GMS, and PAS stains were negative for micro-organisms.
The left pericardial biopsy showed diffuse and extensive non-necrotizing granulomatous inflammation and AFB, GMS, and PAS stains were negative for micro-organisms.
CT scan at the end of that year (131555) showed thickened pericardium.
An MRI at the time showed diffuse thickening of the pericardium with enhancement as well as nodular mid myocardial changes at the hinge points and the inferolateral aspects. Subendocardial changes were also noted.
Repeat MRI the next year showed similar findings
Ashley Davidoff MD
Biventricular Infiltration

Sarcoidosis involves both ventricles and may cause bi-ventricular thickening
Ashley Davidoff MDNext Maryam Vejdani Jahromi, ?
{kind=link}
69 year old male presented with history of cardiomyopathy and atrial fibrillation
The LGE on the short axis shows biventricular thickening of the RV and LV
There are other findings on the MRI that are highly suggestive of sarcoidosis. There are multicentric foci of LGE in linear and nodular form in the mid myocardial and subepicardial layers and likely in the pericardium and myocardium of the right ventricle.
There was associated global hypokinesis of the LV with an EF of 40%, and increase in the LV mass of 120gms/ sq m
Ashley Davidoff MD
next Maryam Vejdani Jahromi