
Hi Hoon
Re “Sarcoidosis, a Scare, Chest Pain and an Octopus”
This is a story about a 59 year old woman who had sarcoidosis, who had a scare developed chest pain that sounded like acute coronary syndrome and was short of breath
Your part is to teach about Sarcoidosis on Chest CT and it is now posted on this page
Almost done streamlining your part
The key I think is to know and teach that sarcoidosis and the lymphatic system go hand in hand – Secondly that sarcoidosis loves to coalesce – granulomas become micronodules – which cluster and coalesce (good buzz words) and things get bigger and more dense downstream by the hila
Also the parallel of the pathogenesis is similar in the heart – See Pedro’s presentation
Thanks for your help
Let me know about any reservations
Thanks
AD
In a Nutshell
-
- Upper Lobe Predominance
- Follow Lymphatics (Go with the flow) starting at
- Pleural and Fissural then
- Centrilobular and Interlobular Septa
- Central lymphatics and then
- Central Lymph Nodes (Egg Shell)
- Nodules that Cluster
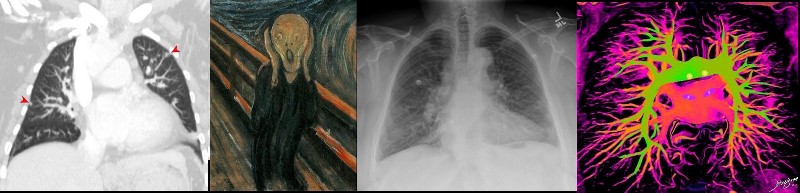
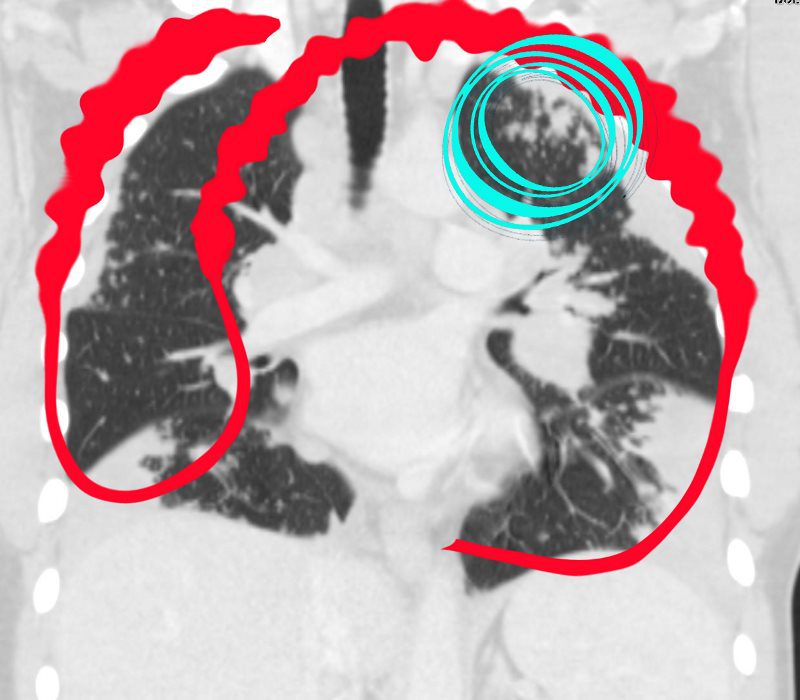
THE ?S? OF SARCOIDOSIS
Sarcoidosis is a nodular granulomatous disease which predominates in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The ?S? for sarcoidosis drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting superficially in the pleura involving the lymphatic system in the pleura, and then flowing downstream into the interlobular septa, bronchovascular bundles and lymph nodes

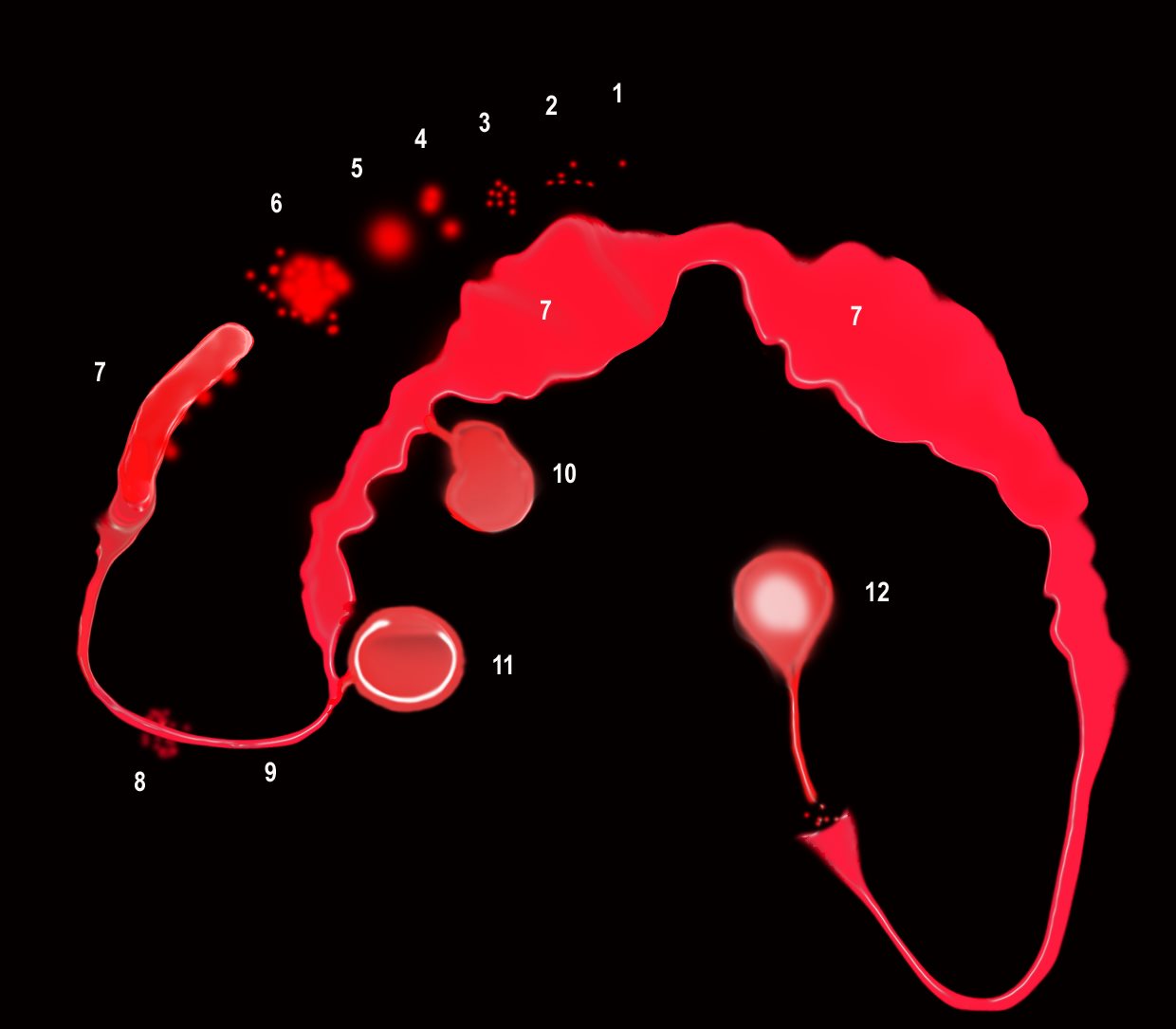
Pathogenesis of morphological changes along the “S” shaped sarcoidosis Curve
The Granulomas
-
- The granulomas start as micronodules in close association with the lymphatics (1) spread in the intralobular septa and centrilobular bronchioles (2) cluster and conglomerate to form macro nodules (4,5) sometimes manifesting as the galaxy sign (6). As they progress centrally the granulomatous changes extend along fissure and bronchovascular bundles (8,9) manifest as thickening and or nodularity. The granulomatous disease continues to cluster and conglomerate becoming mass like along the pathway (7), most commonly centrally as the lymphatics become confluent in the hila (7)
- The lymph nodes in the mediastinum become significantly enlarged and fleshy (10). They often calcify (12) sometimes on the calcify on the rim of the node (eggshell calcification (11)
Nodules in the Secondary Lobules
132090.8.jpg
Ashley Davidoff MD
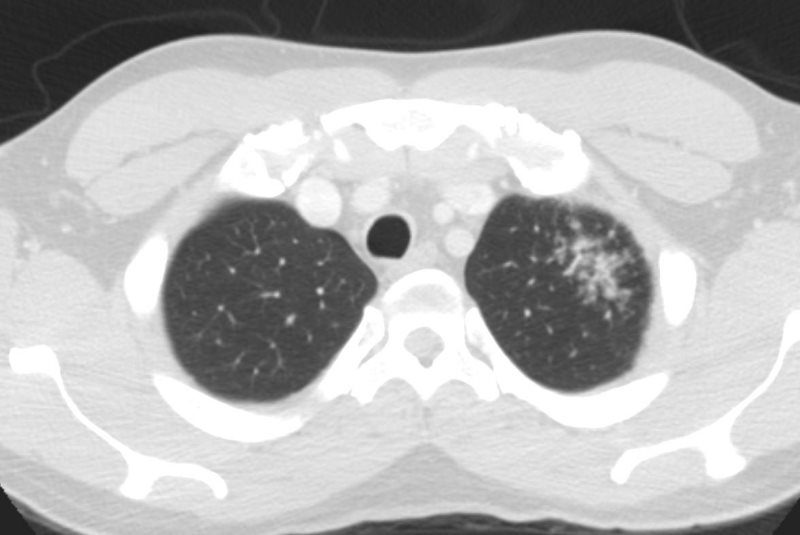
Pleura and Subpleural Disease Thickening and Nodularity
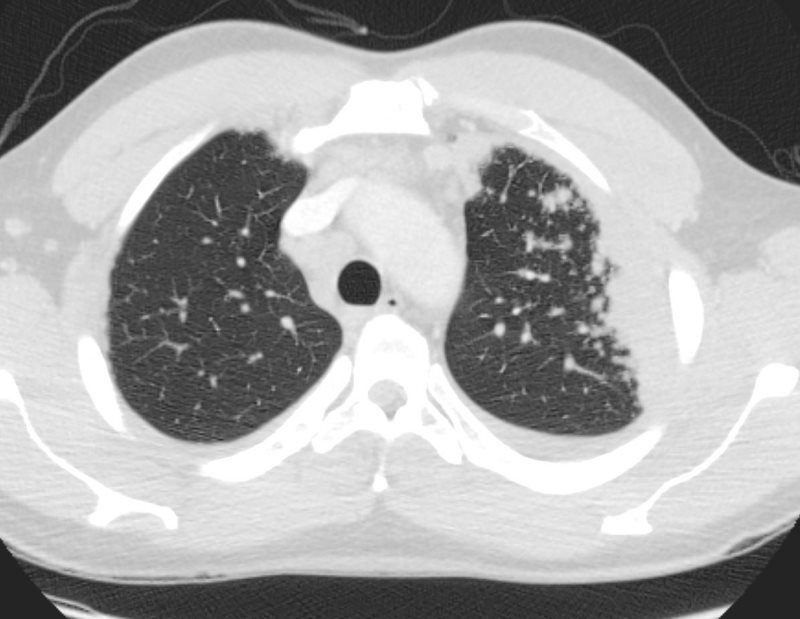 CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE LEFT UPPER LOBE
CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE LEFT UPPER LOBE
Ashley Davidoff MD
Fissural Involvement

Ashley Davidoff MD
Micronodules, Nodules, Coalescence and the Galaxy Sign
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD
Ashley Davidoff MD

Thickening around the Airways
When the nodularity, clustering and or mass formation involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
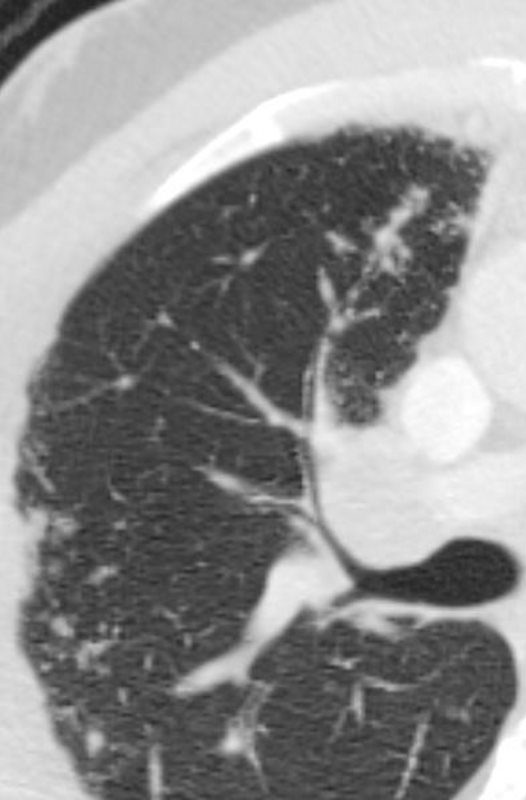 CT WITH SUBPLEURAL AND BRONCHOVASCULAR NODULES IN THE RIGHT UPPER LOBE
CT WITH SUBPLEURAL AND BRONCHOVASCULAR NODULES IN THE RIGHT UPPER LOBE
Ashley Davidoff MD
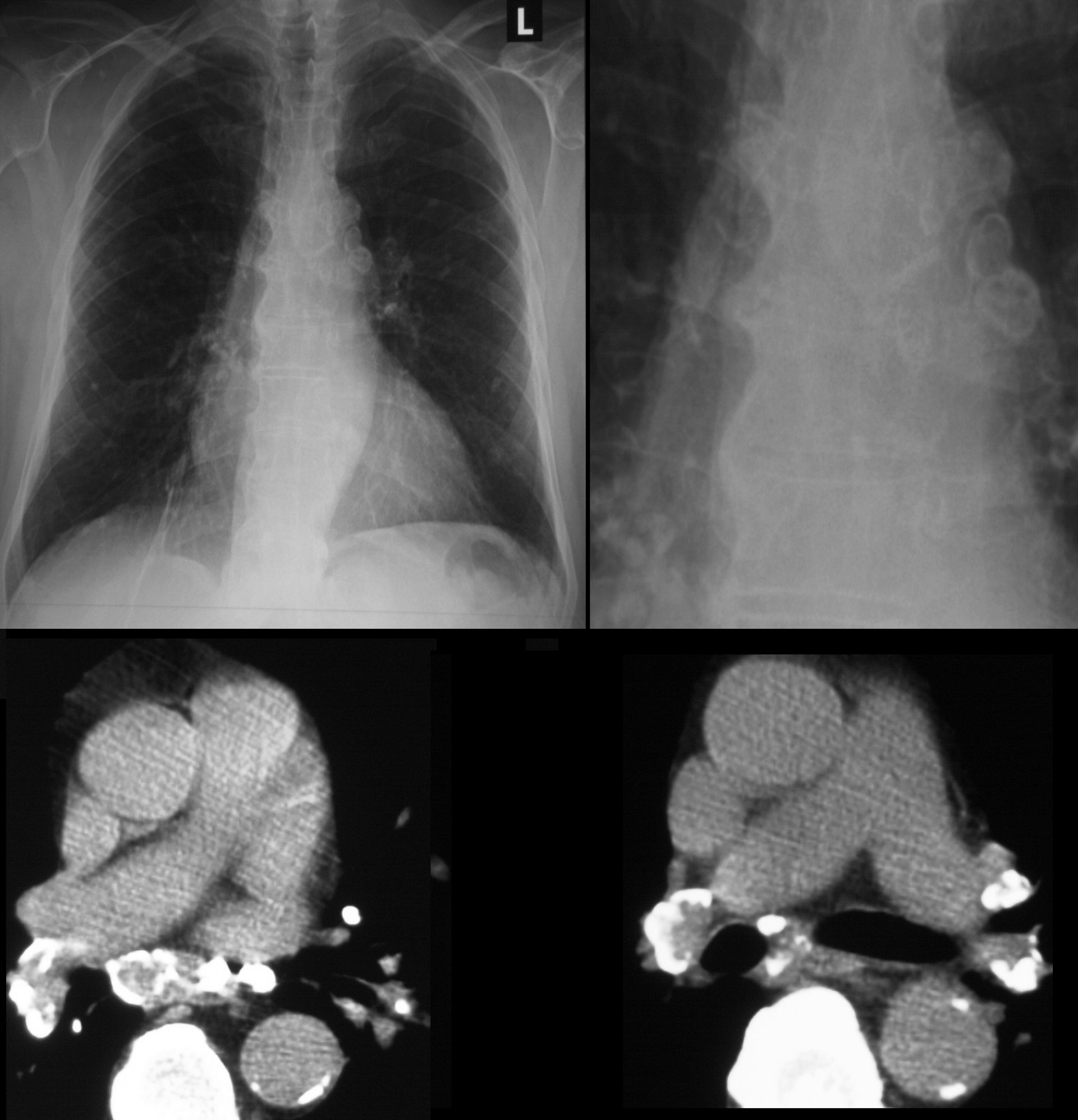
Lymphadenopathy
 CT with MEDIASTINAL AND HILAR ADENOPATHY
CT with MEDIASTINAL AND HILAR ADENOPATHY
Pawnbroker?s Sign
Ashley Davidoff MD
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT OF SARCOIDOSIS
GIF FILENext Pedro Staziaki,