

Hi Ashwin
Sorry for the delay
We should distinguish pathologically between biventricular infiltration and hypertrophy
Biventricular hypertrophy is really rare event
Biventricular thickening /infiltration is also uncommon but should be what we think about when both ventricles are thick
- So first question to address
- Normal thickness of LV in diastole (number to remember is 1.2 but upper limits 1.4cms)
- Normal thickness of RV in diastole (hard to measure but 3-5mms)
- next question
- What are the infiltrative cardiomyopathies that can cause biventricular infiltration
- Most important to remember are
- amyloidosis
- sarcoidosis
- Less commonly
- Hemochromatosis
- Fabry disease,
- Danon disease, and
- Friedreich?s ataxia.
- How do they affect function
- primarily affect diastolic function and
- less commonly systolic function
Examples of Biventricular Thickening/Infiltration?
Our case with SLE, Sjogrens Raynauds
Two other more common causes of biventricular infiltration and thickening
-
- Amyloidosis of the heart
- Sarcoidosis of the heart
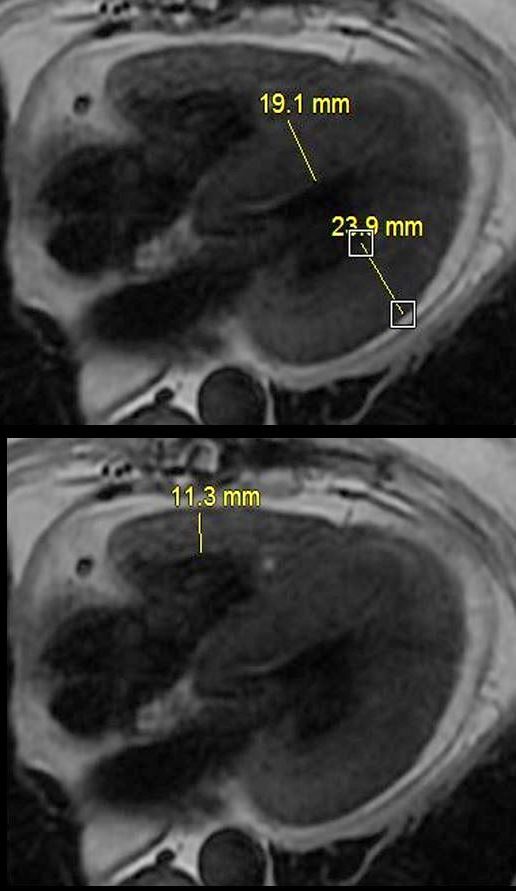
Left Ventricular Septal and Free Wall Thickening Atrial Septal Thickening
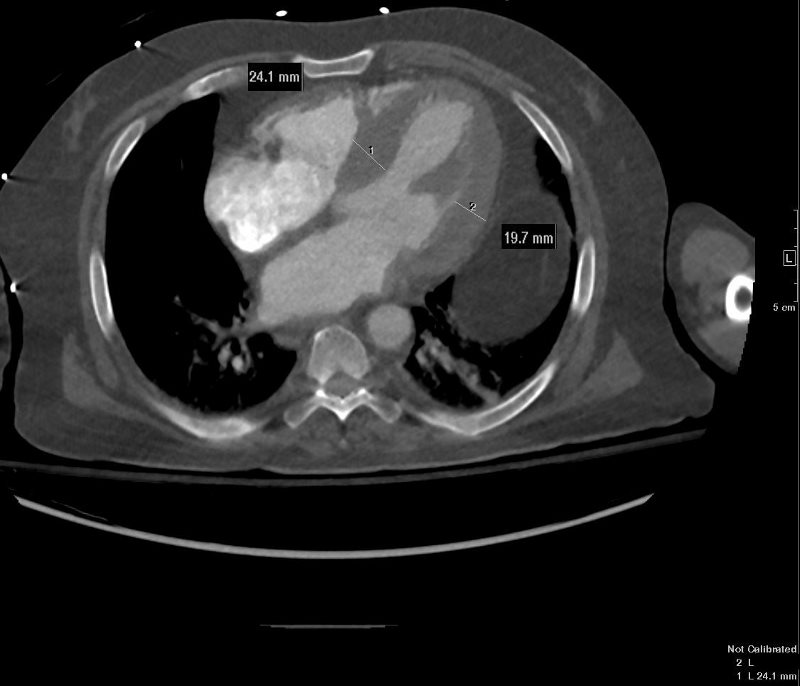 CARDIAC AMYLOIDOSIS with LV THICKENING – INFILTRATION VS LVH
CARDIAC AMYLOIDOSIS with LV THICKENING – INFILTRATION VS LVH
{kind=link}
Non gated axial CT through the opening of the mitral valve suggests early diastole confirms concentric thickening. The septum measures 24.1mms while the free wall measures 19.7mms. Upper limits normal is 14mms.
Cardiac Amyloidosis with Right Ventricular Infiltration CARDIAC AMYLOIDOSIS
CARDIAC AMYLOIDOSIS
{kind=link}
Non gated sagittal CT through the RVOT shows RVH (right ventricular thickening) wall measuring between 6-7mm involving both the RV inflow as well as the outflow See Case 006
Delayed gadolinium in Short Axis Shows Diffuse Dominantly Subendocardial and Myocardial LGE in both LV and RV
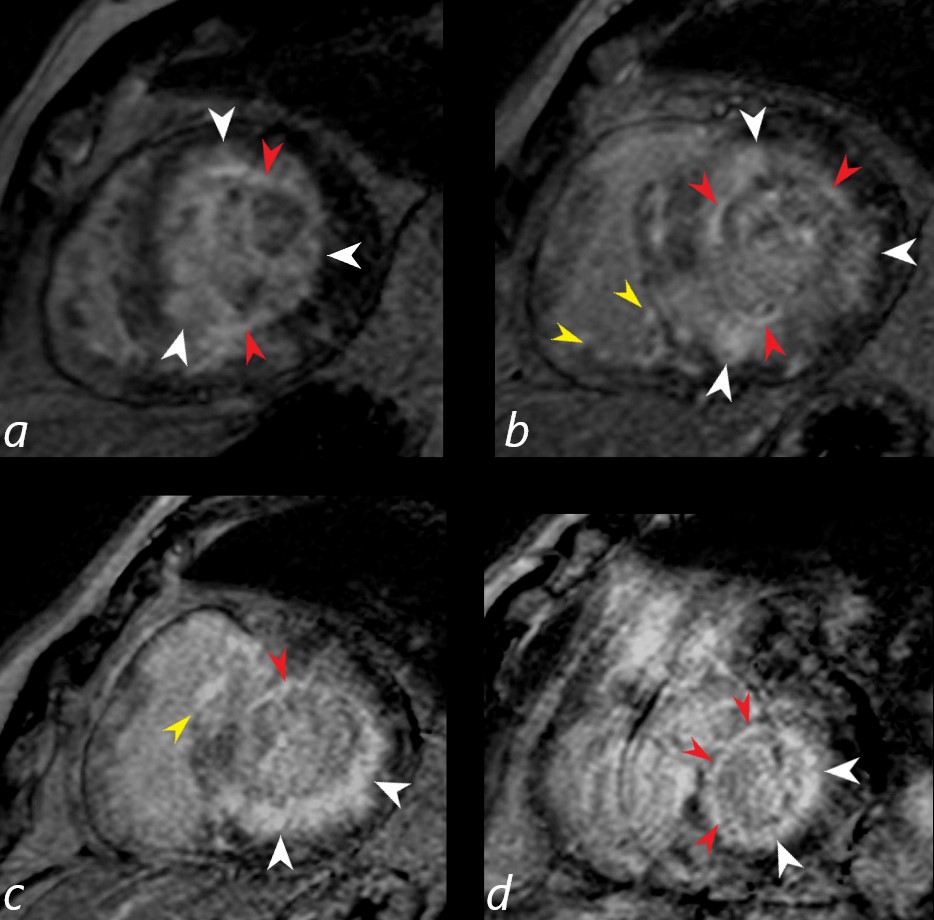
Gated short axis delayed gadolinium sequence through the base LV during diastole and shows subendocardial LGE (red arrowheads in a,b,c, and d, diffuse mid myocardial LGE (white arrowheads) (a,b,c,d) and subepicardial LGE in the RV (yellow arrowheads (b,c)
Ashley Davidoff MD See Case 006
- Key Issues for Cardiac Amyloid
- Difficult to null
Sarcoid Cardiomyopathy with Thickening of Both Ventricles Due to Biventricular Infiltration and Subepicardial LGE
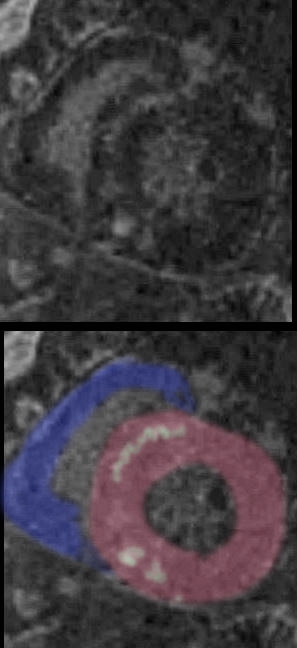
Key Issues for Sarcoidosis
- Similar affinity for lymphatics as in sarcoid of the lungs
- Lymphatics of the heart are subepicardial
- LGE characteristically subepicardial
- Also patchy, multifocal nodular mid myocardial
- most characteristic
- free wall and
- medial basal septum (conduction abnormalities)
- Lymphatics of the heart are subepicardial
25-30% cardiac involvement
-
Other Infiltrative Disease with Biventricular Infiltration and Thickening
-
- hemochromatosis
- Less commonly
- Fabry disease,
- Danon disease, and
- Friedreich?s ataxia.
-
AD will discuss the following diagrams
“A” is for congo red Amyloid
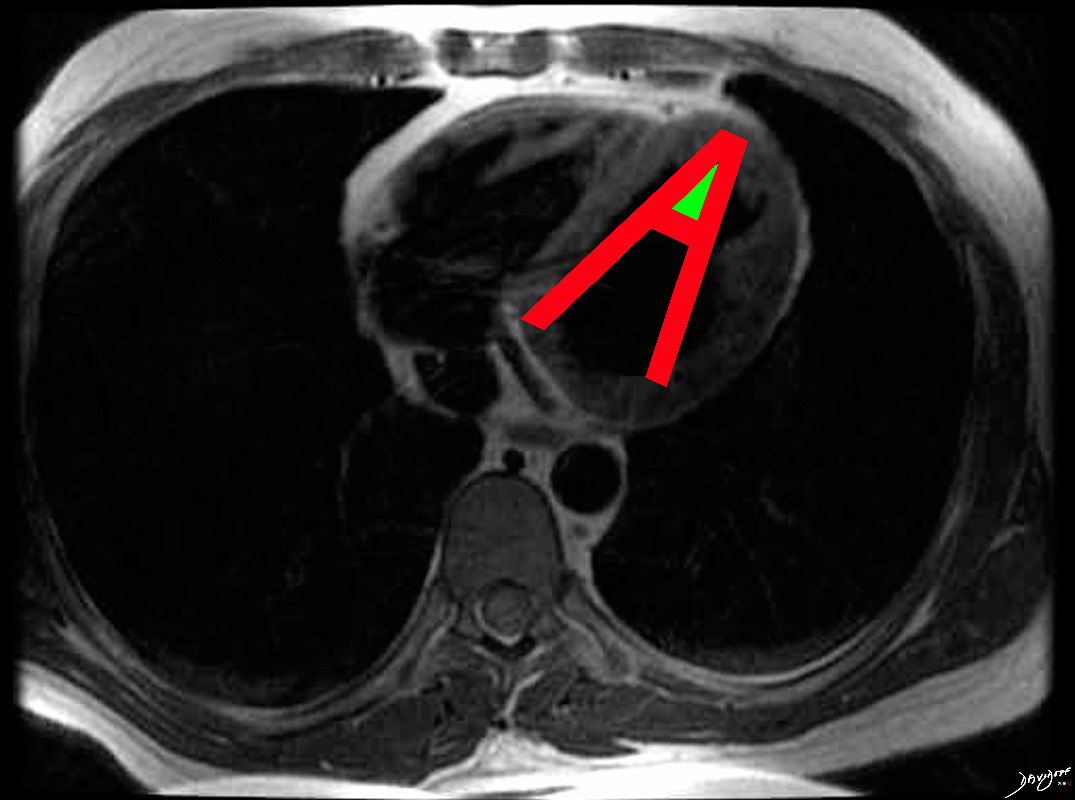
The hallmark of cardiac amyloidosis is LGE involving subendocardial regions with apical sparing and sometimes the atria
Ashley Davidoff MD
Re Other Chamber Involvement with Wall Thickening and Enlargement
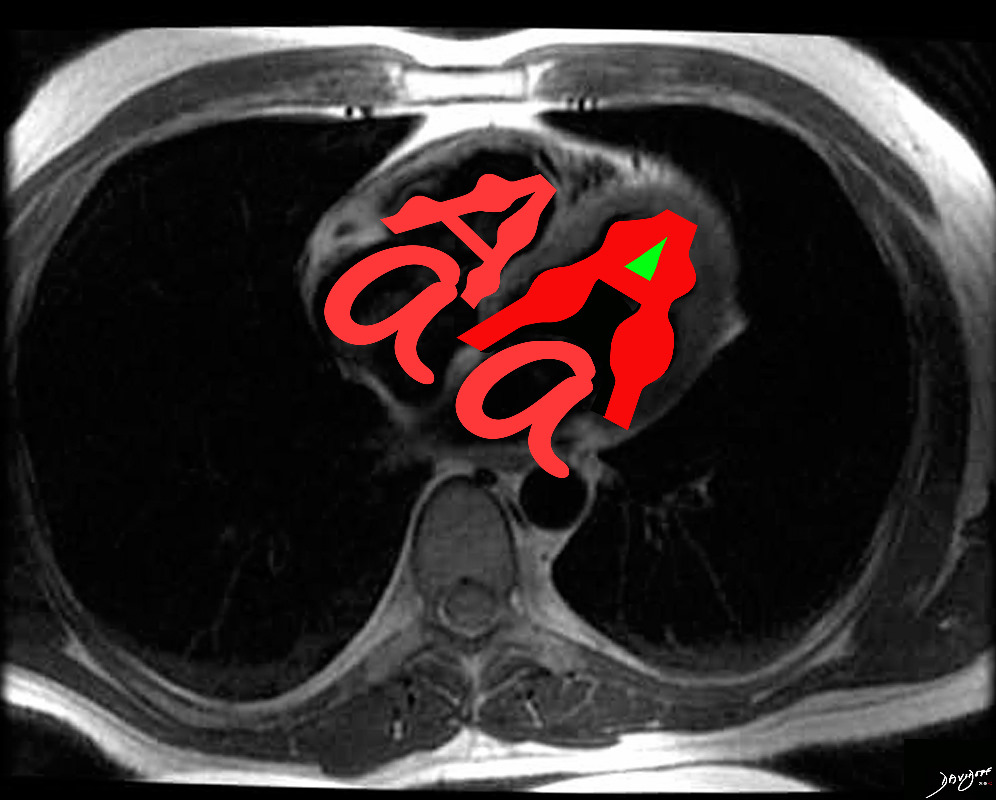
In cardiac amyloidosis increased LV thickness is common , but may involve RV and atrial septum with bilateral atrial enlargement.
Ashley Davidoff MD
and Sarcoidosis
Disease Location and Form
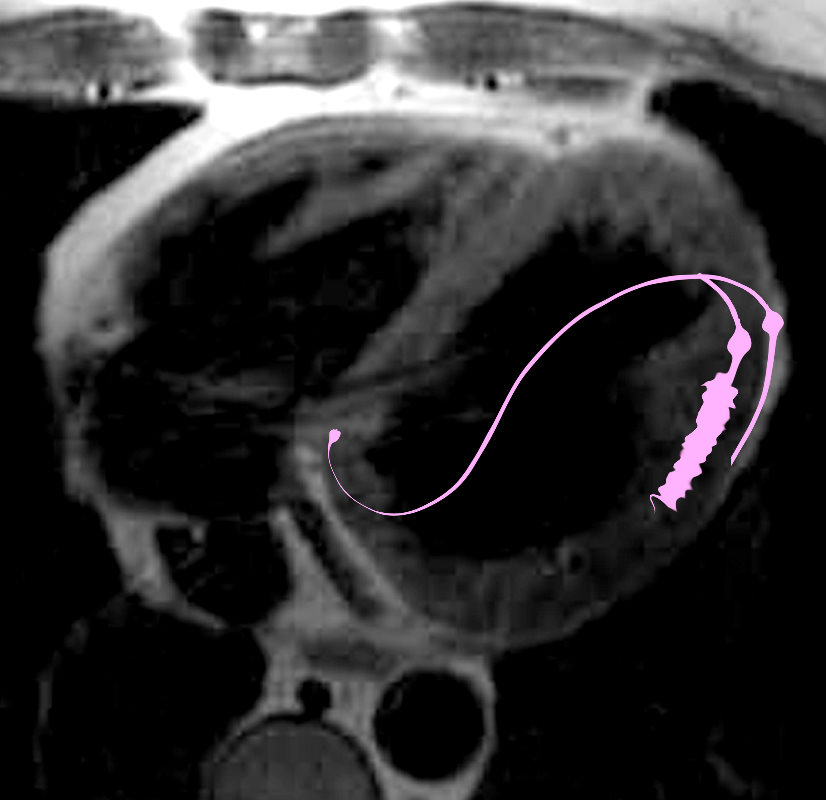
The hallmark of cardiac sarcoidosis is LGE involving subepicardial regions of lateral free wall as well as medial basal septum but also mid myocardial with linear patchy and nodular forms.
Biventricular involvement is common

Sarcoidosis involves both ventricles and may cause bi-ventricular thickening
Ashley Davidoff MD
Next John Lee, Diastolic Heart Failure aka HF with Preserved EF