Aortic dissection is a sudden catastrophic disruption of the aortic wall caused by a shearing tear of the intima, and seconday involvement of the media by the advancing dissection and hematoma. hHe event characterised by a splitting of the arterial wall along the the longitudinal plane of the aorta.
Causative Factors
There is usually associated disease of the media in the form of cystic medial necrosis or the aging process. Familial entities such as Marfan’s syndrome, Ehlos Danlos, are associated with a significant increase of risk for aortic dissection. Entities that increase wall stress such as congenital bicuspid aortic valve, coarctation and hypertension are other factors that contribute to an increase in the incidence of the dissection. Pregnancy in the third trimester also has an increase incidence in dissection presumably due to the changes that occur to collagenous ligaments in pregnancy. About 50% of aortic dissections that occur in women under 40 are in women who are pregnant. Aortic dissection affects men more than women (2:1) with peak incidence in 6th and 7th decades.
Classification
Debakey Classification Type I – ascending aorta, extends beyond the arch Type II – confined to the ascending aorta Type III – originating in the descending aorta and usually propagates distally Type IIIa – confined to thorax Type IIIb – extends beyond diaphragm Type III dissections rarely extend retrograde to the arch
Pathology
95% of dissections occur within a few cms of the aortic valve in the ascending aorta or just distal to the left subclavian artery. There have been two classification systems with the Stanford system being more universally used. DeBakey: I ascending aorta extending to the arch +/- descending aorta (30%) II ascending aorta only (20%) III descending aorta involving the thoracic aorta (50%) Stanford: A involvement of ascending aorta B aortic arch + distal aorta
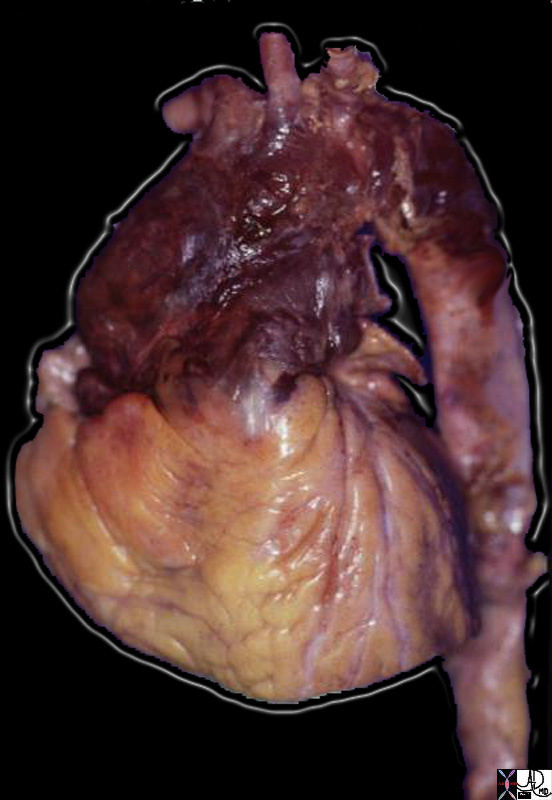
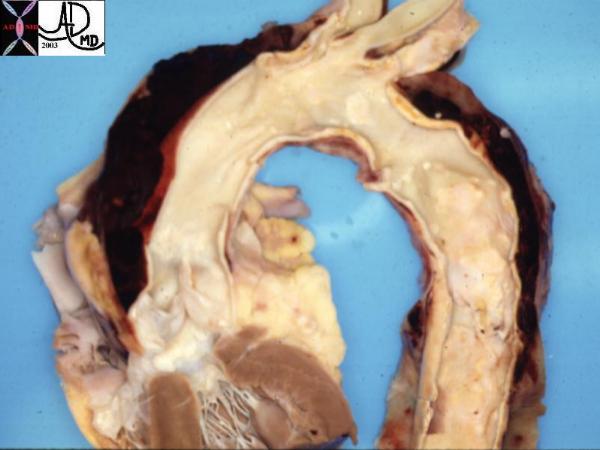
This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy Henri Cuenoid MD 13421 code CVS thorax AO aorta dissection grosspathology
Diagnosis
Aortic Dissection
Aortic dissection is a sudden catastrophic disruption of the aortic wall caused by a shearing tear of the intima and secondary involvement of the media by the advancing dissection and hematoma. The event is characterized by a splitting of the arterial wall along the longitudinal plane of the aorta.
Aortic dissections usually occur as a result of hypertension and are formed after the intima of the aorta ruptures, leading to entry of blood into the aortic wall. Initiating tears are most frequent in the ascending aorta, though the ascending aorta is not the most commonly involved portion of the aorta regarding dissecting aneurysms. The proximal portion of the descending thoracic aorta is the second most common location of a primary intimal tear but because most ascending aortic dissections extend to involve the descending portion and because few primary tears in the descending aorta extend retrograde to the ascending aorta, the descending aorta is the most commonly involved portion of the aorta with dissecting aneurysms.
There is usually associated disease of the media in the form of cystic medial necrosis or the aging process. Familial entities such as Marfan syndrome and Ehlos Danlos syndrome are associated with a significant increase of risk for aortic dissection. Entities that increase wall stress such as congenital bicuspid aortic valve, coarctation and hypertension are other factors that contribute to an increase in the incidence of the dissection. Pregnancy in the third trimester also has an increase incidence in dissection presumably due to the changes that occur to collagenous ligaments in pregnancy. About 50% of aortic dissections that occur in women under 40 are in women who are pregnant. Aortic dissection affects men more than women (2:1) with peak incidence in 6th and 7th decades.
Ninety five percent of dissections occur within a few centimeters of the aortic valve in the ascending aorta or just distal to the left subclavian artery.
There have been two classification systems with the Stanford system being more universally used.
Stanford Classification:
A- Involvement of ascending aorta
B ? Involvement of aortic arch and distal aorta
Debakey Classification
Type I ? ascending aorta, extends beyond the arch (30%)
Type II ? ascending aorta only (20%)
Type III ? descending aorta involving the thoracic aorta (50%)
Descending Thoracic Aortic Dissection Stanford B
The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftward placed larger false lumen (arrows). The double barrel is seen in the descending aorta. Courtesy of: Laura Feldman, M.D.
Therapy is aimed at halting progression of the dissection. Initially, blood pressure should be reduced to <100-120 mm Hg with an intravenous (IV) agents, such as nitroprusside or trimethaphan.
Treatment options are based on the position of the dissection. If the dissection involves the ascending aorta, then emergency surgery is indicated because of the propensity for occlusion of the coronary artery, associated dysfunction of the aortic valve, and rupture into the pericardium.
If only the descending aorta is involved and there are no signs of distal ischemia, then medical management is indicated.
Ascending Aortic Dissection
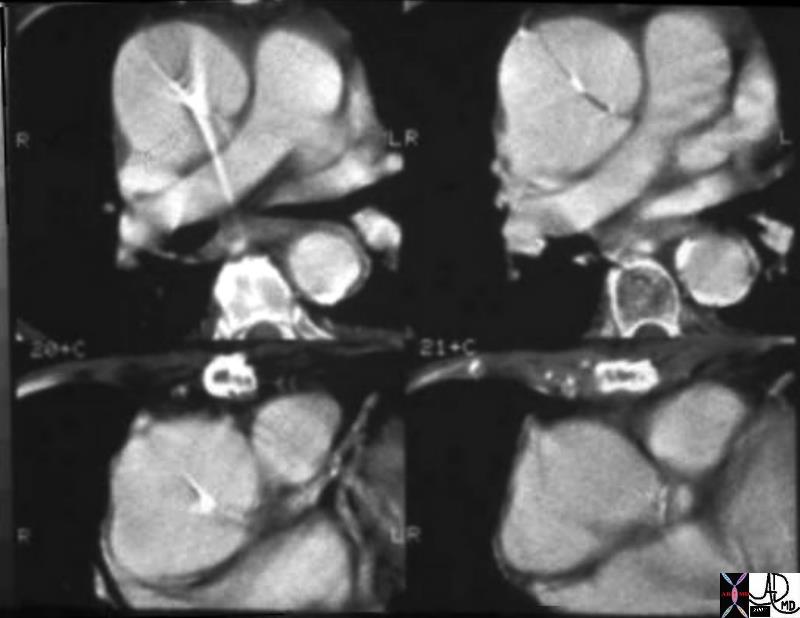
06648 thoracic aorta thorax ascending aortic dissection Type A dissection CTscan Courtesy Ashley Davidoff MD
Descending Thoracic Aortic Dissection
The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftwardly placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap.
Descending Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection. Courtesy Philips Medical Systems 33167
Descending Thoracic Aorta – Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection. Courtesy Philips Medical Systems 33166
Clinical
The clinical presentation is usually dramatic with hypercute “shearing” or “ripping “chest or back pain. Proximal Anterior chest pain is usually associated with tears of the ascending aorta, while dissection of the descending aorta usually give interscapular pain. Most patients are hypertensive. Findings on examination include aortic insufficiency (50%), pulse deficits (50% – commonly involve the brachiocephalic vessels) or neurologic manifestations Distal dissections may reveal pulse deficits of the left subclavian or femoral vessels
Diagnostic Tools
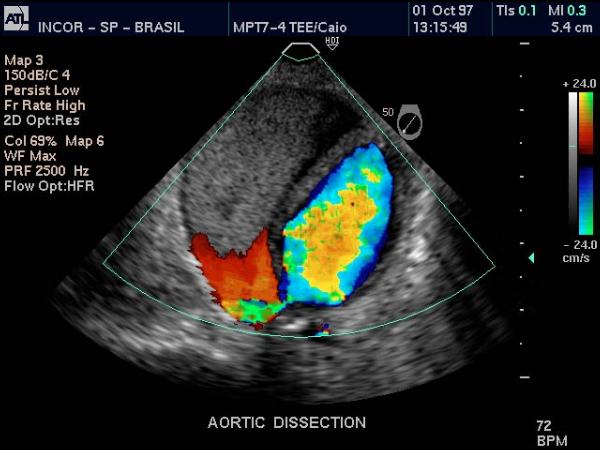
The radiologic diagnosis is often suspected on the plain film with the widened mediastinum and more specifically a blunted aortic knob or thickening of the wall of the knob more than 5 mm past the calcified aortic intima (Ring sign). CT, MRI and trans-esophageal echocardiography are all used with highsensitivity and specificty. TEE sensitivity/specificity of 99/98% Aortic angiography is an invasive procedure but may be best at delineating the extent of dissection
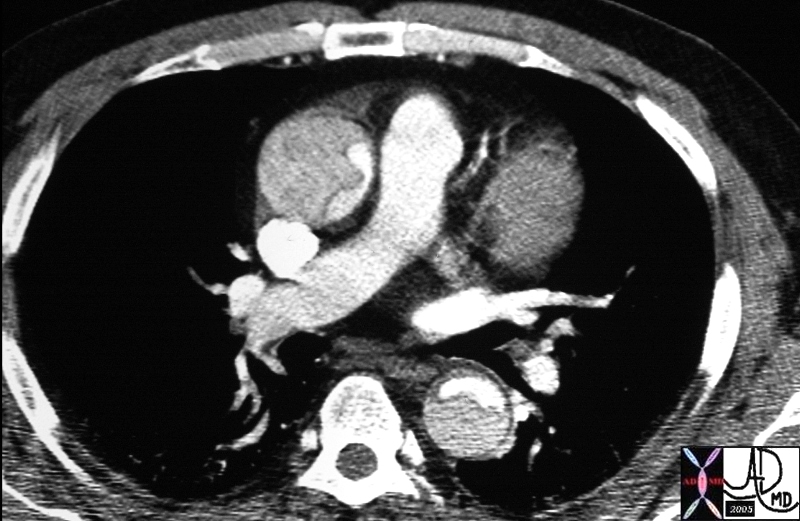
Dissection Involving the Ascending and Descending Aorta
20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB
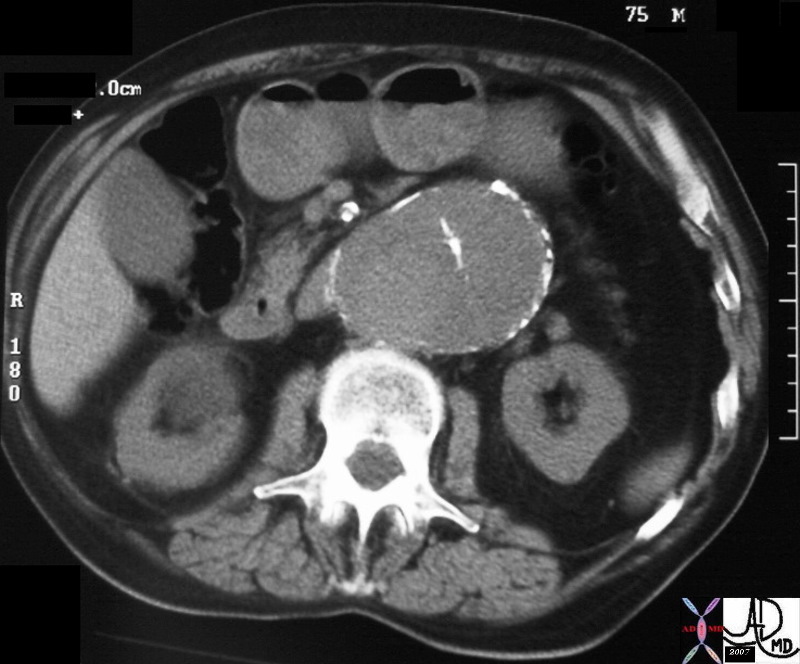
Type B dissection involving descending thoracic and abdominal aorta
31262 hx 75 male with abdominal pain abdomen abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan Davidoff MD
Rupture
Ruture of the Ascending Aorta
81F presents with acute shearing back pain and hypotension thorax thoracic aorta ascending aorta fx focal dissection rupture pericardium mediastinum fluid blood pericardial effusion hemopericardium azygous vein fx reflux dx aortic dissection with pericardial tamponade imaging radiology CTscan
Courtesy Ashley Davidoff MD 22343bduos500 hx
Treatment
Therapy is aimed at halting progression of the dissection Initially blood pressure should be reduced to <100-120 mm Hg with an IV agents such as nitroprusside or trimethaphan A decrease in the dV/dt (LV ejection velocity) should be done with beta-blockers Definitive treatment can be medical or surgical Surgical results are superior in acute proximal dissections (80% survival) and medical therapy may be advantageous in uncomplicated distal dissections (80% survival) For acute distal dissections complicated by vital organ compromise, rupture, aortic regurgitation or extension into the ascending aorta, surgery is also warranted Stable, isolated arch dissections and stable chronic dissections can be treated medically
Ando M, Okita Y, Tagusari O: Surgery in three-channeled aortic dissection. A 31-patient review. Jpn J Thorac Cardiovasc Surg 2000 Jun; 48(6): 339-43[Medline].
Armstrong WF, Bach DS, Carey LM: Clinical and echocardiographic findings in patients with suspected acute aortic dissection. Am Heart J 1998 Dec; 136(6): 1051-60[Medline].
Bloch MJ, Trost DW, Sos TA: Type B aortic dissection complicating renal artery angioplasty and stent placement. J Vasc Interv Radiol 2001 Apr; 12(4): 517-20[Medline].
Bogaert J, Meyns B, Rademakers FE: Follow-up of aortic dissection: contribution of MR angiography for evaluation of the abdominal aorta and its branches. Eur Radiol 1997; 7(5): 695-702[Medline].
Chang WT, Kao HL, Liau CS: Aortic stenting on a type B aortic dissection with visceral and limb ischemia. Catheter Cardiovasc Interv 2001 Jan; 52(1): 112-5[Medline].
Coady MA, Rizzo JA, Hammond GL: Penetrating ulcer of the thoracic aorta: what is it? How do we recognize it? How do we manage it? J Vasc Surg 1998 Jun; 27(6): 1006-15; discussion 1015-6[Medline].
Connell DA, Thomson KR, Gibson RN: Stent placement in coeliac and superior mesenteric arteries to restore vascular perfusion following aortic dissection. Australas Radiol 1995 Feb; 39(1): 68-70[Medline].
Gendal ES, Mendelson DS, Janus CL: Magnetic resonance imaging of isolated abdominal aortic dissection. Clin Imaging 1989 Sep; 13(3): 217-9[Medline].
Goldman AP, Kotler MN, Scanlon MH: The complementary role of magnetic resonance imaging, Doppler echocardiography, and computed tomography in the diagnosis of dissecting thoracic aneurysms. Am Heart J 1986 May; 111(5): 970-81[Medline].
Hagan PG, Nienaber CA, Isselbacher EM: The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 2000 Feb 16; 283(7): 897-903[Medline].
Ho VB, Prince MR: Thoracic MR aortography: imaging techniques and strategies. Radiographics 1998 Mar-Apr; 18(2): 287-309[Medline].
House-Fancher MA: Aortic dissection: pathophysiology, diagnosis, and acute care management. AACN Clin Issues 1995 Nov; 6(4): 602-13; quiz 683-4[Medline].
Inoue K, Sato M, Iwase T: Clinical endovascular placement of branched graft for type B aortic dissection. J Thorac Cardiovasc Surg 1996 Oct; 112(4): 1111-3[Medline].
Joao I, Duarte JA, Cotrim C: Acute type A aortic dissection involving the left main coronary artery and the aortic valve–a case report. Rev Port Cardiol 2001 Mar; 20(3): 333-8[Medline].
Juvonen T, Ergin MA, Galla JD: Risk factors for rupture of chronic type B dissections. J Thorac Cardiovasc Surg 1999 Apr; 117(4): 776-86[Medline].
Kadir S: Arteriography of the thoracic aorta. In: Diagnostic Angiography. Philadelphia, Pa: Saunders WB; 1986: 124-71.
Kaminaga T, Yamada N, Takamiya M: Sequential MR signal change of the thrombus in the false lumen of thrombosed aortic dissection. Magn Reson Imaging 1995; 13(6): 773-9[Medline].
Kaneda T, Lemura J, Zhang Z: A case of Standford type B aortic dissection involving a right-sided aortic arch with mirror-image branching and right-sided descending aorta. Thorac Cardiovasc Surg 2001 Feb; 49(1): 51-3[Medline].
Lansman SL, McCullough JN, Nguyen KH: Subtypes of acute aortic dissection. Ann Thorac Surg 1999 Jun; 67(6): 1975-8; discussion 1979-80[Medline].
Madu EC, Shala B, Baugh D: Crack-cocaine-associated aortic dissection in early pregnancy–a case report. Angiology 1999 Feb; 50(2): 163-8[Medline].
Maffei S, Baroni M, Terrazzi M: Ambulatory follow-up of aortic dissection: comparison between computed tomography and biplane transesophageal echocardiography. Int J Card Imaging 1996 Jun; 12(2): 105-11[Medline].
Mast HL, Gordon DH, Kantor AM: Pitfalls in diagnosis of aortic dissection by angiography: algorithmic approach utilizing CT and MRI. Comput Med Imaging Graph 1991 Nov-Dec; 15(6): 431-40[Medline].
Mastrogiovanni G, Masiello P, Leone R: Emergency surgical management of acute aortic dissection: role of transesophageal echocardiography. G Ital Cardiol 1999 Oct; 29(10): 1137-41[Medline].
McClarren-Curry C, Shaughnessy K: Acute thoracic aortic dissection: can your nurses defuse a time bomb? Nurs Manage 1999 Dec; 30(12): 32-4, 36[Medline].
Meszaros I, Morocz J, Szlavi J: Epidemiology and clinicopathology of aortic dissection. Chest 2000 May; 117(5): 1271-8[Medline].
Miller JS, Lemaire SA, Coselli JS: Evaluating aortic dissection: when is coronary angiography indicated? Heart 2000 Jun; 83(6): 615-6[Medline].
Nitatori T, Yokoyama K, Nakamura A: Clinical application of single shot GRE-EPI as non-enhanced MRA (EPI- MRA) for aortic aneurysm and dissection. Radiat Med 1999 Sep-Oct; 17(5): 393-7[Medline].
Penco M, Paparoni S, Dagianti A: Usefulness of transesophageal echocardiography in the assessment of aortic dissection. Am J Cardiol 2000 Aug 17; 86(4 Suppl 1): 53-56.
Picard E, Marty-Ane CH, Vernhet H: Endovascular management of traumatic infrarenal abdominal aortic dissection. Ann Vasc Surg 1998 Nov; 12(6): 515-21[Medline].
Reber D, Aebert H, Manke M: Percutaneous fenestration of the aortic dissection membrane in malperfusion syndrome. Eur J Cardiothorac Surg 1999 Jan; 15(1): 91-4[Medline].
Sakuma H, Bourne MW, O’Sullivan M: Evaluation of thoracic aortic dissection using breath-holding cine MRI. J Comput Assist Tomogr 1996 Jan-Feb; 20(1): 45-50[Medline].
San Roman JA, Vilacosta I, Fernandez-Aviles F: [Aortic dissection: clinical evaluation, comparison of diagnostic techniques and treatment election]. Rev Esp Cardiol 1996; 49 Suppl 4: 2-12[Medline].
Sarasin FP, Louis-Simonet M, Gaspoz JM: Detecting acute thoracic aortic dissection in the emergency department: time constraints and choice of the optimal diagnostic test. Ann Emerg Med 1996 Sep; 28(3): 278-88[Medline].
Torossov M, Singh A, Fein SA: Clinical presentation, diagnosis, and hospital outcome of patients with documented aortic dissection: the Albany Medical Center experience, 1986 to 1996. Am Heart J 1999 Jan; 137(1): 154-61[Medline].
Vogt BA, Birk PE, Panzarino V: Aortic dissection in young patients with chronic hypertension. Am J Kidney Dis 1999 Feb; 33(2): 374-8[Medline].
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ruture of the Ascending Aorta
81F presents with acute shearing back pain and hypotension thorax thoracic aorta ascending aorta fx focal dissection rupture pericardium mediastinum fluid blood pericardial effusion hemopericardium azygous vein fx reflux dx aortic dissection with pericardial tamponade imaging radiology CTscan
Courtesy Ashley Davidoff MD 22343bduos500 hx
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ruture of the Ascending Aorta
81F presents with acute shearing back pain and hypotension thorax thoracic aorta ascending aorta fx focal dissection rupture pericardium mediastinum fluid blood pericardial effusion hemopericardium azygous vein fx reflux dx aortic dissection with pericardial tamponade imaging radiology CTscan
Courtesy Ashley Davidoff MD 22343bduos500 hx
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 81F presents with acute shearing back pain and hypotension thorax thoracic aorta ascending aorta fx focal dissection rupture pericardium mediastinum fluid blood pericardial effusion hemopericardium azygous vein fx reflux dx aortic dissection with pericardial tamponade imaging radiology CTscan
Courtesy Ashley Davidoff MD 22343bduos500 hx
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 81F presents with acute shearing back pain and hypotension thorax thoracic aorta ascending aorta fx focal dissection rupture pericardium mediastinum fluid blood pericardial effusion hemopericardium azygous vein fx reflux dx aortic dissection with pericardial tamponade imaging radiology CTscan
Courtesy Ashley Davidoff MD 22343bduos500 hx
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Ruture of the Ascending Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Ruture of the Ascending Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Aortic Dissection
31262 hx 75 male with abdominal pain abdomen abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Aortic Dissection
31262 hx 75 male with abdominal pain abdomen abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 31262 hx 75 male with abdominal pain abdomen abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 31262 hx 75 male with abdominal pain abdomen abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Aortic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Aortic Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Type B dissection involving descending thoracic and abdominal aorta
24588 thorax abdomen fx dissection true lumen false lumen occluded renal artery angiogram angiography Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Type B dissection involving descending thoracic and abdominal aorta
24588 thorax abdomen fx dissection true lumen false lumen occluded renal artery angiogram angiography Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Descending Thoracic Aorta – Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection. Courtesy Philips Medical Systems 33166
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Descending Thoracic Aorta – Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection. Courtesy Philips Medical Systems 33166
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection. Courtesy Philips Medical Systems 33166
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection. Courtesy Philips Medical Systems 33166
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Descending Thoracic Aorta – Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Descending Thoracic Aorta – Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Descending Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection. Courtesy Philips Medical Systems 33167
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Descending Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection. Courtesy Philips Medical Systems 33167
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection. Courtesy Philips Medical Systems 33167
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection. Courtesy Philips Medical Systems 33167
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Descending Thoracic Aorta – Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Descending Thoracic Aorta – Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Descending Thoracic Aortic Dissection
The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftwardly placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Descending Thoracic Aortic Dissection
The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftwardly placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftwardly placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftwardly placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Descending Thoracic Aortic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Descending Thoracic Aortic Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ascending Aortic Dissection
06648 thoracic aorta thorax ascending aortic dissection Type A dissection CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ascending Aortic Dissection
06648 thoracic aorta thorax ascending aortic dissection Type A dissection CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 06648 thoracic aorta thorax ascending aortic dissection Type A dissection CTscan Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 06648 thoracic aorta thorax ascending aortic dissection Type A dissection CTscan Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Ascending Aortic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Ascending Aortic Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dissection
This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy Henri Cuenoid MD 13421 code CVS thorax AO aorta dissection grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dissection
This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy Henri Cuenoid MD 13421 code CVS thorax AO aorta dissection grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] =>
[lastElementChild] =>
[childElementCount] => 0
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy Henri Cuenoid MD 13421 code CVS thorax AO aorta dissection grosspathology
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy Henri Cuenoid MD 13421 code CVS thorax AO aorta dissection grosspathology
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Dissection
)

 Dissection
Dissection
 Ascending Aortic Dissection
Ascending Aortic Dissection