
| Occlusion of the Aorta
The Common Vein Copyright 2008 Definition Occlusion of the aorta implies a total obstruction of bllod flow. It may be acute or chronic. Acute Aortic Occlusion Acute aortic occlusion is most commonly caused by an embolus, thrombosis on stenotic atherosclerotic disease or by extension of an aortic dissection. Acute occlusion on t atherosclerotic disease is also called Leriche’s syndrome. Other causes include iatrogenic occlusion due to catheter manipulation, hypercoaguable disease, and malignancy. The result is acute ischemia of the distal organs, most commonly the lower limbs, so that pain parasthesias, pallor, pulslessness and paralysis (5p’s) are clinical manifestations. Leriche’s syndrome is characterized by absence of femoral pulses, pain in the legs or buttocks, and impotence and is characteristically seen in young males. Diagnosis is usually suspected by the clinical presentation and is confirmed by ultrasound or CT scan.
Treatment is urgent and emergency embolectomy is usually the quickest and most effective method. Thrombolytics can also be employed if the clinical situation is not deemed emergent. Chronic Aortic Occlusion Chronic occlusion of the aorta is usually caused by progressive stenotic and atherosclerotic disease of the distal abdominal aorta. The slow progressive nature of the disease usually allows collateral supply from mesenteric intercostal and lumbar vessels to develop so that the result is relatively benign and may even be an incidental finding. The diagnosis may be suspected clinically by reduced femoral pulses but CTscan or MRI would confirm the clinical suspicion. compensation.  Ashley Davidoff MD TheCommonVein.net
In the asymptomatic patient no treatment is required, but bypass is indicated if there is concern about distal ischemia.
|


DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Occlusion of the Proximal Abdominal Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Occlusion of the Proximal Abdominal Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
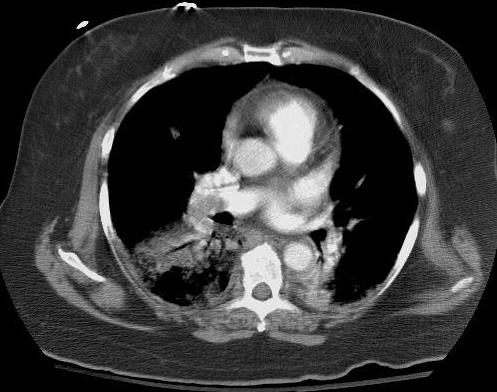
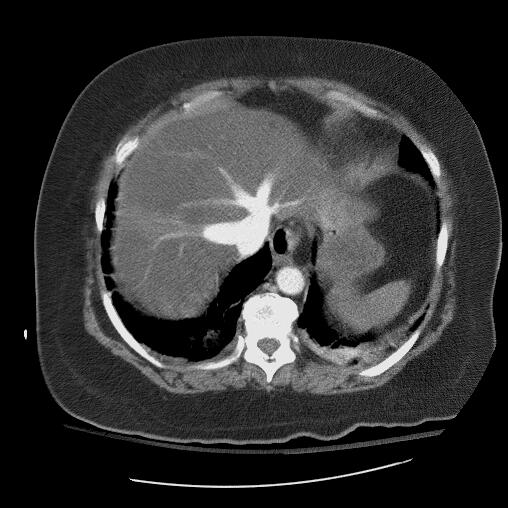
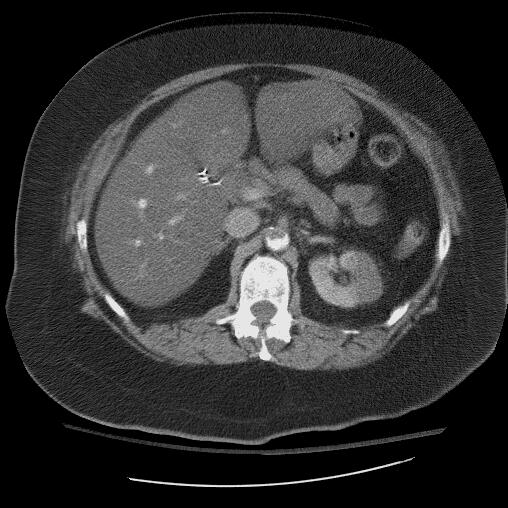
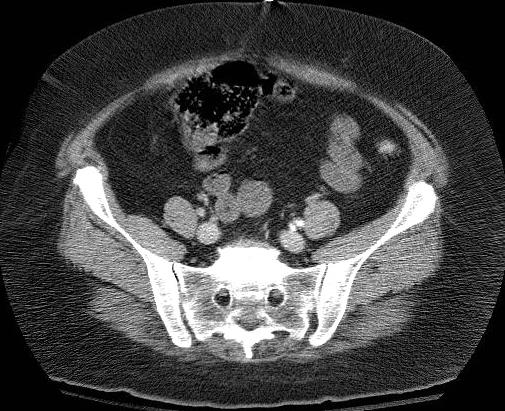
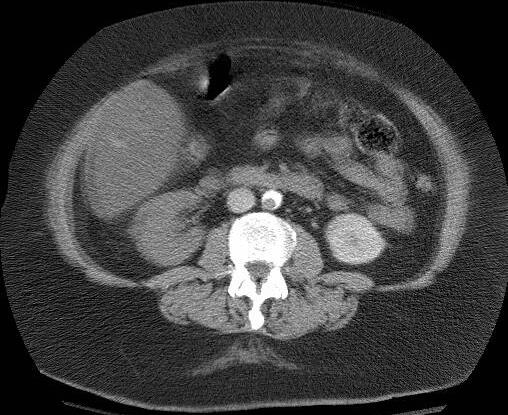
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Occlusion of the Aorta
The Common Vein Copyright 2008
Definition
Occlusion of the aorta implies a total obstruction of bllod flow. It may be acute or chronic.
Acute Aortic Occlusion
Acute aortic occlusion is most commonly caused by an embolus, thrombosis on stenotic atherosclerotic disease or by extension of an aortic dissection. Acute occlusion on t atherosclerotic disease is also called Leriche’s syndrome. Other causes include iatrogenic occlusion due to catheter manipulation, hypercoaguable disease, and malignancy.
The result is acute ischemia of the distal organs, most commonly the lower limbs, so that pain parasthesias, pallor, pulslessness and paralysis (5p’s) are clinical manifestations.
Leriche’s syndrome is characterized by absence of femoral pulses, pain in the legs or buttocks, and impotence and is characteristically seen in young males.
Diagnosis is usually suspected by the clinical presentation and is confirmed by ultrasound or CT scan.
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
Treatment is urgent and emergency embolectomy is usually the quickest and most effective method. Thrombolytics can also be employed if the clinical situation is not deemed emergent.
Chronic Aortic Occlusion
Chronic occlusion of the aorta is usually caused by progressive stenotic and atherosclerotic disease of the distal abdominal aorta.
The slow progressive nature of the disease usually allows collateral supply from mesenteric intercostal and lumbar vessels to develop so that the result is relatively benign and may even be an incidental finding.
The diagnosis may be suspected clinically by reduced femoral pulses but CTscan or MRI would confirm the clinical suspicion. compensation.
Infrarenal abdominal aortic occlusionAshley Davidoff MD TheCommonVein.net
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
In the asymptomatic patient no treatment is required, but bypass is indicated if there is concern about distal ischemia.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] =>
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Occlusion of the Aorta
The Common Vein Copyright 2008
Definition
Occlusion of the aorta implies a total obstruction of bllod flow. It may be acute or chronic.
Acute Aortic Occlusion
Acute aortic occlusion is most commonly caused by an embolus, thrombosis on stenotic atherosclerotic disease or by extension of an aortic dissection. Acute occlusion on t atherosclerotic disease is also called Leriche’s syndrome. Other causes include iatrogenic occlusion due to catheter manipulation, hypercoaguable disease, and malignancy.
The result is acute ischemia of the distal organs, most commonly the lower limbs, so that pain parasthesias, pallor, pulslessness and paralysis (5p’s) are clinical manifestations.
Leriche’s syndrome is characterized by absence of femoral pulses, pain in the legs or buttocks, and impotence and is characteristically seen in young males.
Diagnosis is usually suspected by the clinical presentation and is confirmed by ultrasound or CT scan.
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
Treatment is urgent and emergency embolectomy is usually the quickest and most effective method. Thrombolytics can also be employed if the clinical situation is not deemed emergent.
Chronic Aortic Occlusion
Chronic occlusion of the aorta is usually caused by progressive stenotic and atherosclerotic disease of the distal abdominal aorta.
The slow progressive nature of the disease usually allows collateral supply from mesenteric intercostal and lumbar vessels to develop so that the result is relatively benign and may even be an incidental finding.
The diagnosis may be suspected clinically by reduced femoral pulses but CTscan or MRI would confirm the clinical suspicion. compensation.
Infrarenal abdominal aortic occlusionAshley Davidoff MD TheCommonVein.net
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
In the asymptomatic patient no treatment is required, but bypass is indicated if there is concern about distal ischemia.
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Occlusion of the Proximal Abdominal Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Occlusion of the Proximal Abdominal Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 6
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 20
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Occlusion of the Aorta
The Common Vein Copyright 2008
Definition
Occlusion of the aorta implies a total obstruction of bllod flow. It may be acute or chronic.
Acute Aortic Occlusion
Acute aortic occlusion is most commonly caused by an embolus, thrombosis on stenotic atherosclerotic disease or by extension of an aortic dissection. Acute occlusion on t atherosclerotic disease is also called Leriche’s syndrome. Other causes include iatrogenic occlusion due to catheter manipulation, hypercoaguable disease, and malignancy.
The result is acute ischemia of the distal organs, most commonly the lower limbs, so that pain parasthesias, pallor, pulslessness and paralysis (5p’s) are clinical manifestations.
Leriche’s syndrome is characterized by absence of femoral pulses, pain in the legs or buttocks, and impotence and is characteristically seen in young males.
Diagnosis is usually suspected by the clinical presentation and is confirmed by ultrasound or CT scan.
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
Treatment is urgent and emergency embolectomy is usually the quickest and most effective method. Thrombolytics can also be employed if the clinical situation is not deemed emergent.
Chronic Aortic Occlusion
Chronic occlusion of the aorta is usually caused by progressive stenotic and atherosclerotic disease of the distal abdominal aorta.
The slow progressive nature of the disease usually allows collateral supply from mesenteric intercostal and lumbar vessels to develop so that the result is relatively benign and may even be an incidental finding.
The diagnosis may be suspected clinically by reduced femoral pulses but CTscan or MRI would confirm the clinical suspicion. compensation.
Infrarenal abdominal aortic occlusionAshley Davidoff MD TheCommonVein.net
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
In the asymptomatic patient no treatment is required, but bypass is indicated if there is concern about distal ischemia.
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Occlusion of the Aorta
The Common Vein Copyright 2008
Definition
Occlusion of the aorta implies a total obstruction of bllod flow. It may be acute or chronic.
Acute Aortic Occlusion
Acute aortic occlusion is most commonly caused by an embolus, thrombosis on stenotic atherosclerotic disease or by extension of an aortic dissection. Acute occlusion on t atherosclerotic disease is also called Leriche’s syndrome. Other causes include iatrogenic occlusion due to catheter manipulation, hypercoaguable disease, and malignancy.
The result is acute ischemia of the distal organs, most commonly the lower limbs, so that pain parasthesias, pallor, pulslessness and paralysis (5p’s) are clinical manifestations.
Leriche’s syndrome is characterized by absence of femoral pulses, pain in the legs or buttocks, and impotence and is characteristically seen in young males.
Diagnosis is usually suspected by the clinical presentation and is confirmed by ultrasound or CT scan.
Non Occlusive Thrombus in the Aorta Caused by a Paradoxical Embolus
This patient suffered both pulmonary and systemic embolization simultaneously. Thrombus from her lower limbs embolized to her pulmonary circulation, she developed pulmonary hypertension with elevated right atrial pressures, and subsequently shunted both blood and embolic material fro her right atrium through a patent foramen ovale to the left atrium. She was fortunate not to embolize to her carotid circulation but she did embolize to her right kidney, aorta and iliac vessels.
43675 kidney fx hypodense hypoperfusion fx non perfusion kidney infarction aorta fx filling defect crescent dx pulmonary embolism PE secondary pulmonary hypertension and TR embolus via PFO imaging radiology CTscan Courtesy Ashley Davidoff MD 43666 43670 43672 43675 43680 43683 5star
Treatment is urgent and emergency embolectomy is usually the quickest and most effective method. Thrombolytics can also be employed if the clinical situation is not deemed emergent.
Chronic Aortic Occlusion
Chronic occlusion of the aorta is usually caused by progressive stenotic and atherosclerotic disease of the distal abdominal aorta.
The slow progressive nature of the disease usually allows collateral supply from mesenteric intercostal and lumbar vessels to develop so that the result is relatively benign and may even be an incidental finding.
The diagnosis may be suspected clinically by reduced femoral pulses but CTscan or MRI would confirm the clinical suspicion. compensation.
Infrarenal abdominal aortic occlusionAshley Davidoff MD TheCommonVein.net
Chronic Occlusion of the Proximal Abdominal Aorta
The MRA shows a chronic occlusion of the abdominal aorta just below the origin of the SMA. Multiple collateral are employed to bypass the obstruction and help supply the distal vessels.
14646.800 Courtesy Ashley Davidoff MD
In the asymptomatic patient no treatment is required, but bypass is indicated if there is concern about distal ischemia.
)