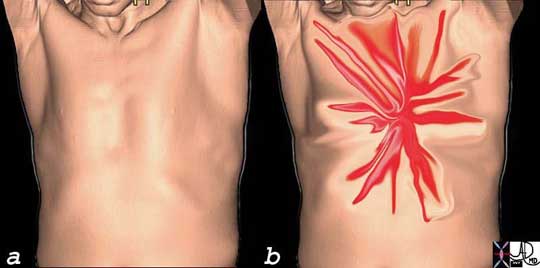
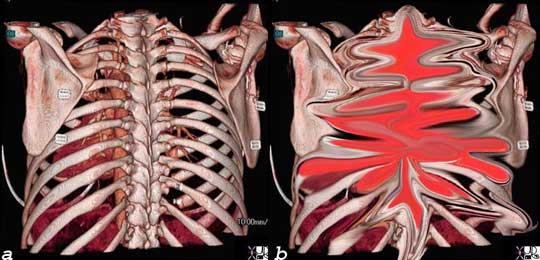
Fatal Acute Dissection This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood. Courtesy of: Henri Cuenoud, M.D. Aortic Dissection Aortic dissection is a sudden catastrophic disruption of the aortic wall caused by a shearing tear of the intima, and secondary involvement of the media by the advancing dissection and hematoma. The event characterized by a splitting of the arterial wall along the longitudinal plane of the aorta. The pain of aortic dissection is dramatic. It is classically hyper acute, sudden, severe, lancinating, excruciating, tearing, stabbing, throbbing, reaching its maximum intensity at the moment of onset. On the other hand, some patients may present with minimal or no symptoms. The duration of the pain is not measured in minutes and may simulate the pain of myocardial infarction. The pain may be felt in the anterior chest, the neck, and/or the back, sometimes reflecting the location of the dissection with ascending dissections noted with anterior chest pain, arch dissections with neck pain and descending thoracic dissections noted with intrascapular or back pain. Since dissections may involve the coronary arteries, and more commonly the right, myocardial ischemic pain may be present as well. It is historically interesting to note that in 1910 William Osler recognized that “spontaneous tear of the arterial coats is associated with atrocious pain, with symptoms, indeed, in the case of the aorta of angina pectoris and many instances have been mistaken for it”. The pain is caused by the stretching of the aortic wall, and hence its potential to have a throbbing character. It is not aggravated by position or body movement, nor relieved other than by analgesia, tincture of time, or repair. The impending sense of doom originally described as “angor animi” literally means anguish of the soul may accompany the pain. This sensation sometimes accompanies other life-threatening situations when there is massive outpouring of catecholamines, such as myocardial infarction and pulmonary embolism. AcuteAorticSyn.jpg Acute Severe Lancinating, Shearing, Chest Pain of Acute Aortic Syndrome Ashley Davidoff Lancinating, Shearing Back Pain of Acute Aortic Syndrome The pain of dissection may be felt either in the front of the chest and/or the back. Either way, the pain can have similar characteristics – i.e. sharp, thunderbolt-like, severe, and rapidly and almost instantaneously reaching maximum intensity coincident with the onset. Courtesy of: Ashley Davidoff, M.D.
spontaneous splitting the media of the aortic wall
longitudinal separation of the aortic intima and adventitia
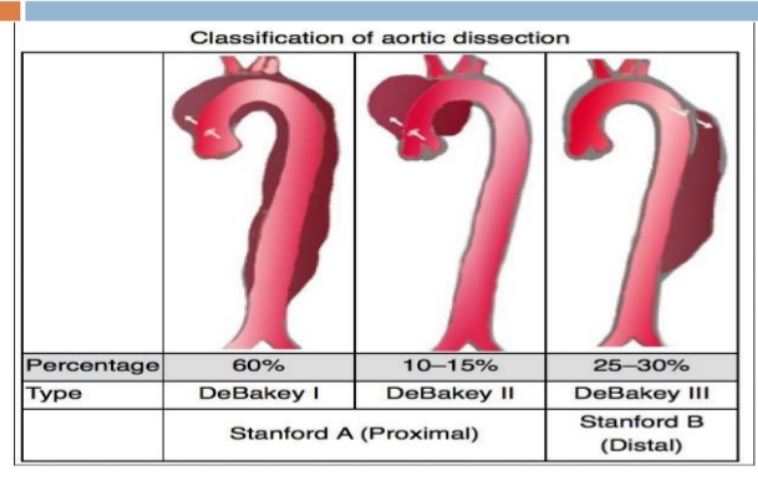
Stanford type A dissection 60%?70% of cases
involves the ascending thoracic aorta,
dissection flap may extend into the descending aorta.
untreated, type A dissections are associated with a mortality rate of over 50% within 48 hours
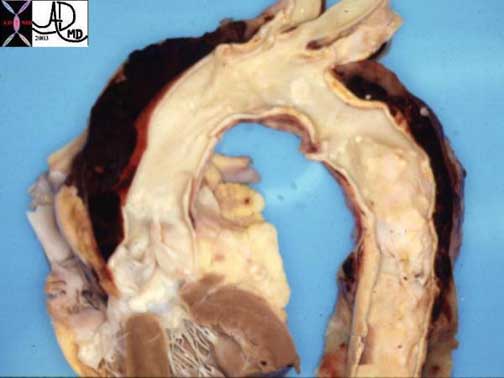
Fatal Acute Dissection
This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood.
Courtesy of: Henri Cuenoud, M.D.
Dissection of the Ascending Aorta
Flow stress on the Aorta Ashley Davidoff TheCommonVein.net
CXR
normal in 10%?40%
displacement of calcification of the aorta was reported in 15%
abnormal cardiac contour being noted in 25%
Waterbottle heart
Transthoracic echocardiography
Type A
sensitivity 80% -100%
Type B
30%?50% for dissections involving the descending aorta
TEE
can be performed in the ER
requires expertise
95%?100% specificity
distal ascending aorta
brachiocephalics and carotids
not be adequately evaluated
good for
aortic root dilatation,
aortic regurgitation,
coronary ostial patency,
pericardial effusions,
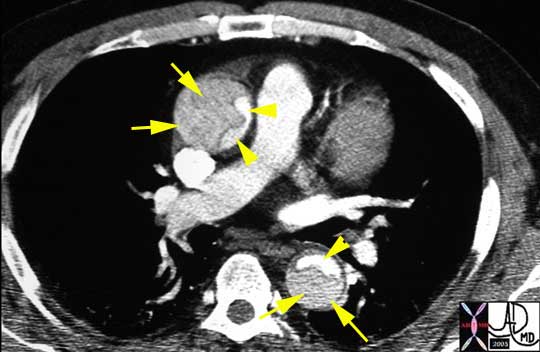
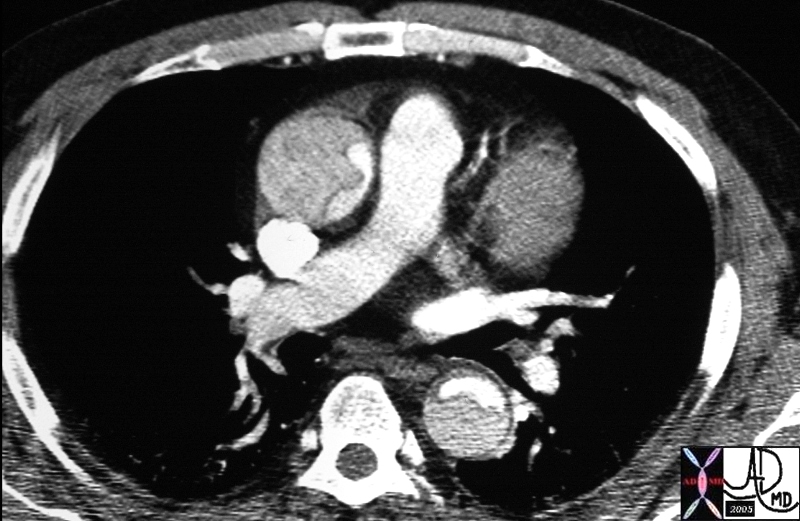
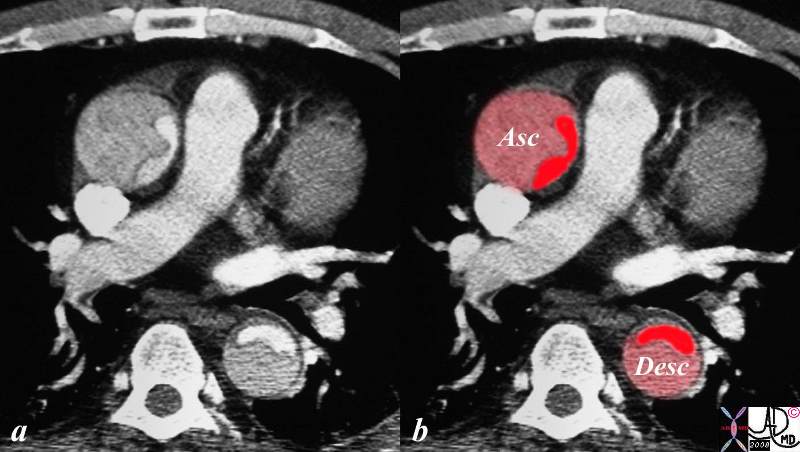
Type A Dissection The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density). The involvement of the ascending aorta makes it a type A dissection and therefore, treatment requires surgical repair. In this patient, however, the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery. Courtesy of: Ashley Davidoff, M.D.
Type A Aortic Dissection
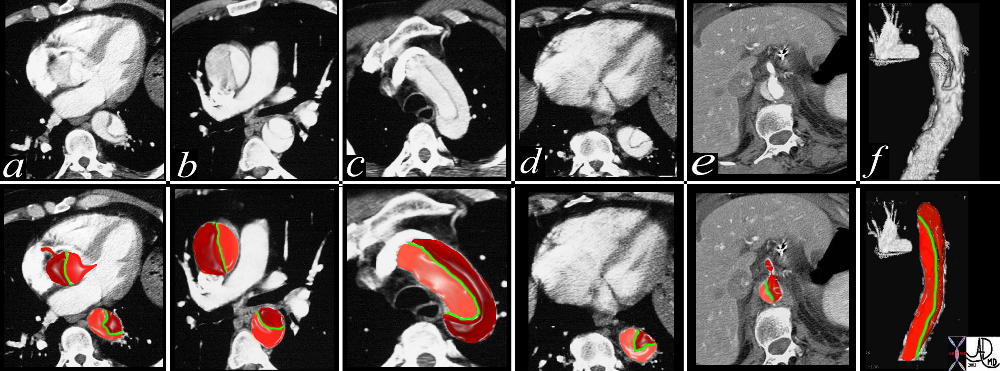
This combination of images from a CTscan through the thorax, reveals an aortic dissection starting at the level of the aortic valve and extending into the abdomen with involvement of the celiac axis. The true lumen is overlaid in pink while the false lumen is overlaid in a darker red. The green structure is the intimal flap. Flow in the false lumen is slightly delayed and slower as seen by the lower density of the contrasyt within it.
Copyright 2012 Courtesy Ashley Davidoff MD. 19412c02 code CVS artery AO aorta dissection fx crescent
Type A Aortic Dissection extending into the iliac arteries Ashley Davidoff MD TheCommonVein.net
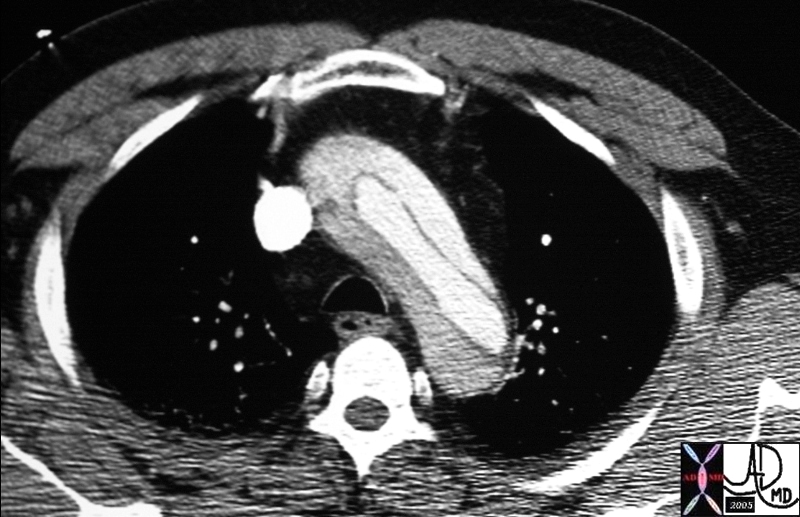
Arch Dissection – Narrowed True Lumen
thorax thoracic aorta arch aorta fx dissection dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20449
36865c
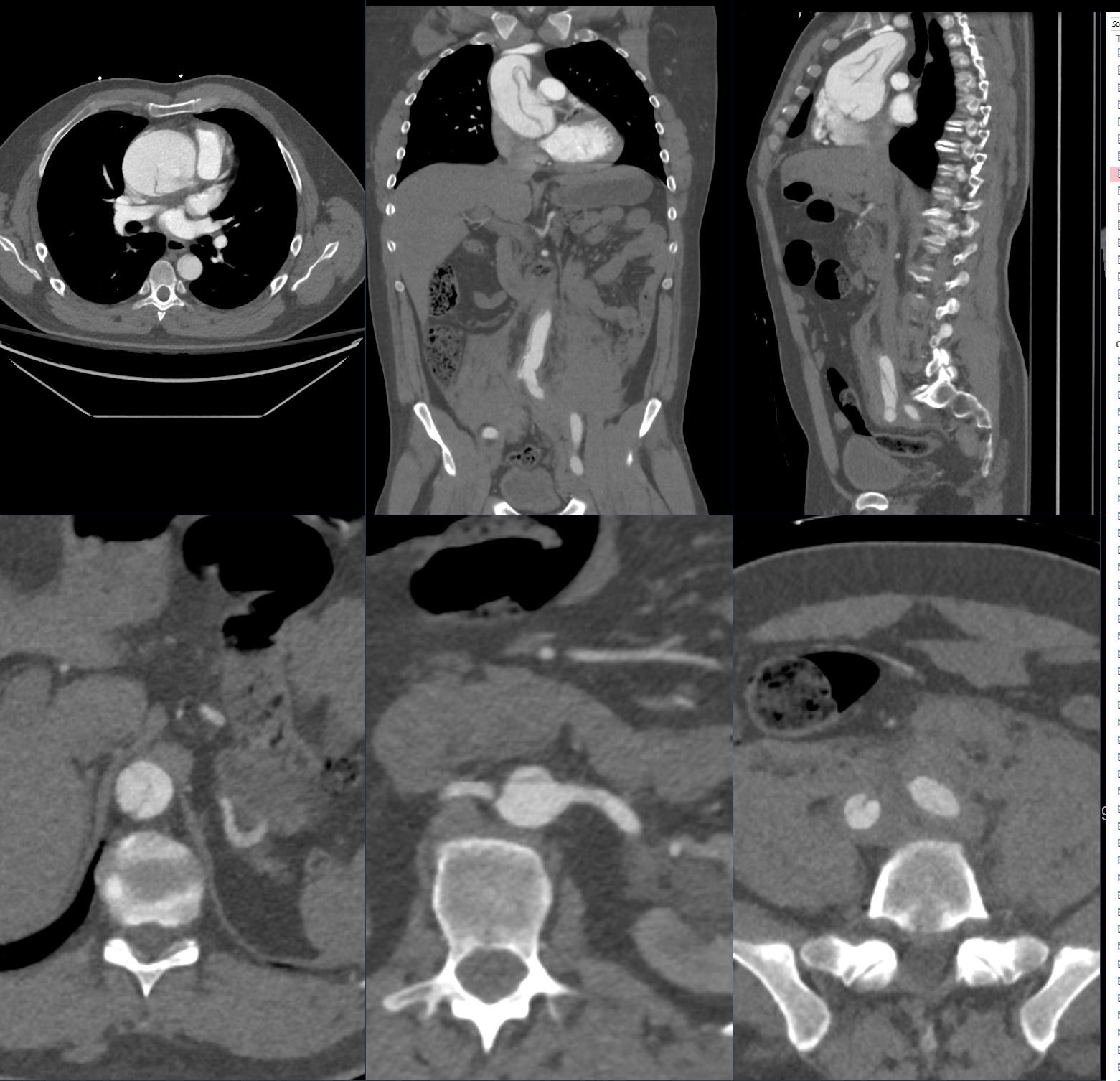
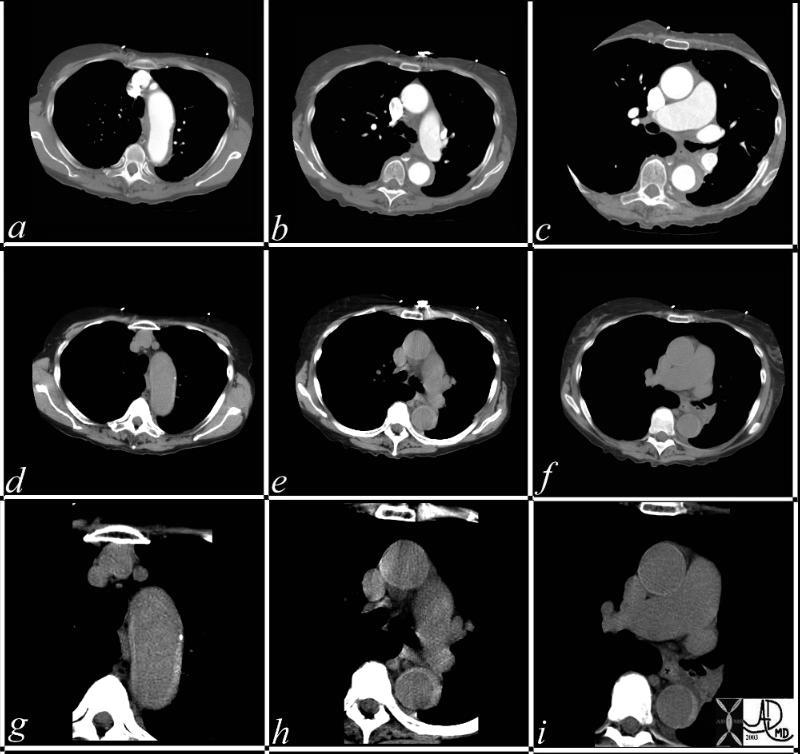
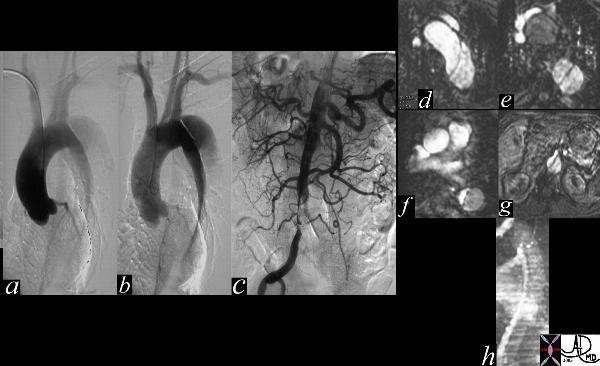
This series of CT scans were taken 1 day apart. The patient presented with chest pain and the soft tissue changes around contrast filled aorta (a,b,c) suggested a chronic dissection, or an acute thrombosed dissection. 1 day later the non-contrast CT clearly reveals an acute thrombosed dissection (d,e,f) that started in the arch and extended along the descending thoracic aorta. The last series (g,h,i) enhance the non contrats study. A non contrast CT followed by contrast injection, is an important tchnique to optimally characterise acute changes in this clincal setting.
Copyright 2012 Courtesy Ashley Davidoff MD 36865c
Stanford type B dissection
involves the descending thoracic aorta
distal to the left subclavian artery
30%?40% of cases
medical treatment of hypertension,
unless complications
extension of the dissection –
end-organ ischemia
persistent pain
requires surgery
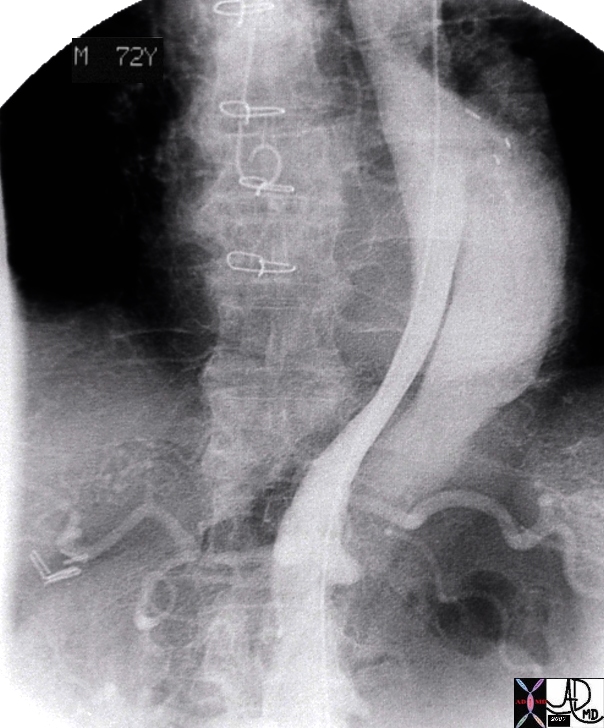
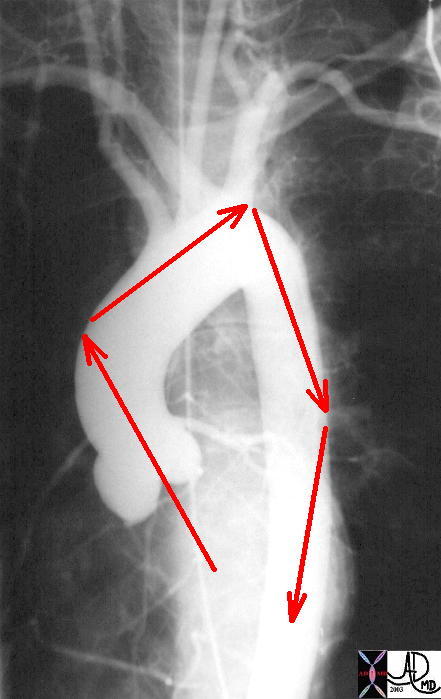
Descending Thoracic Aortic Dissection The digital angiogram in the LAO projection shows an intimal dissection starting just after the left subclavian artery. The true lumen is medial and smaller than the laterally and leftward placed larger false lumen. 35204 Courtesy Laura Feldman MD. code CVS artery aorta thorax thoracic descending dissection angiogram code aorta artery dissection flap. Courtesy of Laura Feldman MD. 35204
Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection.
Courtesy Philips Medical Systems 33167
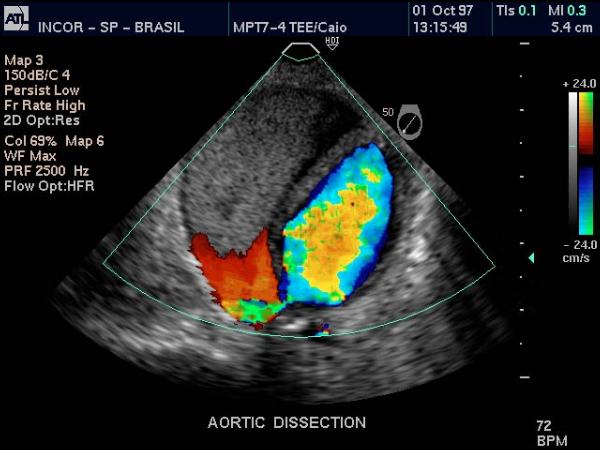
Color Flow Doppler – Descending Thoracic Aorta Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166
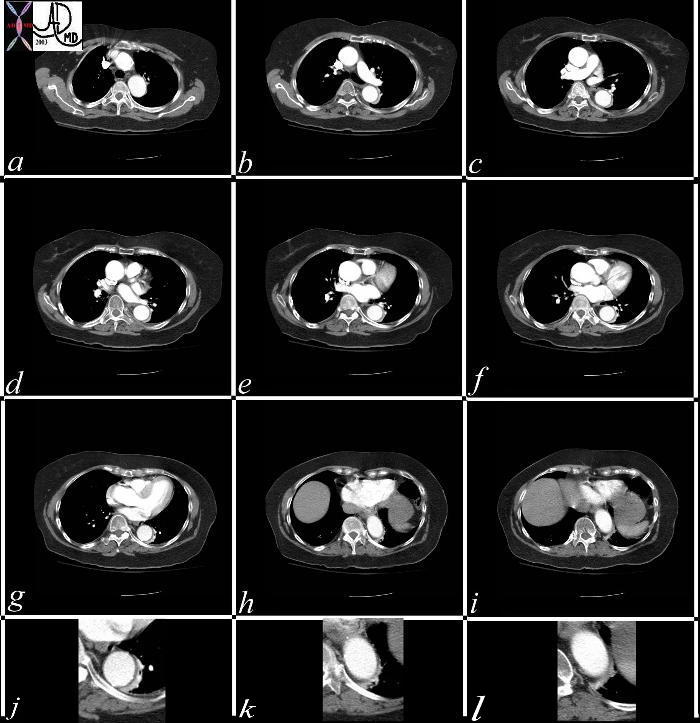
Atelectasis Masquerading as a Dissection
This series of CT scans from the arch to the abdominal inlet shows a curvilinear density around the aorta on its left lateral edge that masquerades as a dissection The last three images (g,h,i) and their magnified counterparts below them (j,k,l) shows air bronchograms opacified vessels within the crescentic density, and deviation from the contour of the aorta, confirming the atelectatic nature of the crescent.
Copyright 2012 Courtesy Ashley Davidoff MD 37071c
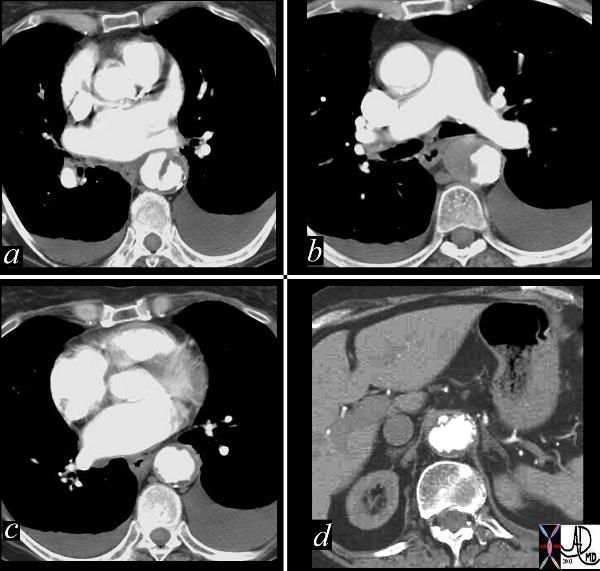
Dissection Caused by Ulcerating Plaque Complicated by Mural Hematoma
This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease.
True Lumen Compressed and Supplying Right Renal Artery
artery aorta fx dissection dx dissection angiography
Copyright 2012 Courtesy Ashley Davidoff MD 17474
True Lumen Compressed on Left
Slow Flow in False Lumen
abdomen artery + abdominal aorta + fx crescentic crescent shaped false lumen fx dissection + dx iatrogenic + imaging radiology CTscan radiologists and detectives
Copyright 2012 Courtesy Ashley DAvidoff MD 19408
Type B Dissection
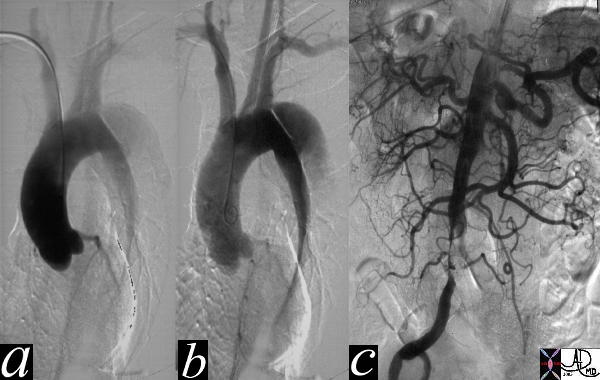
The thoracic angiogram reveals an aortic dissection which starts just after the left subclaian artery. The true lumen is the narrowed medial lumen which is denser than the larger lateral false lumen. (a,b) In (c) the A-P view reveals a patent proximal abdominal aorta, but the distal narrowing and occlusion of the the left iliac artery suggests that the dissection has progressed distally. In the image 35124c the cross sectional images of the abdominal aorta reveal that the true lumen of the distal aorta is in fact quite narrowed.
Courtesy Laura Feldman MD. 35116c
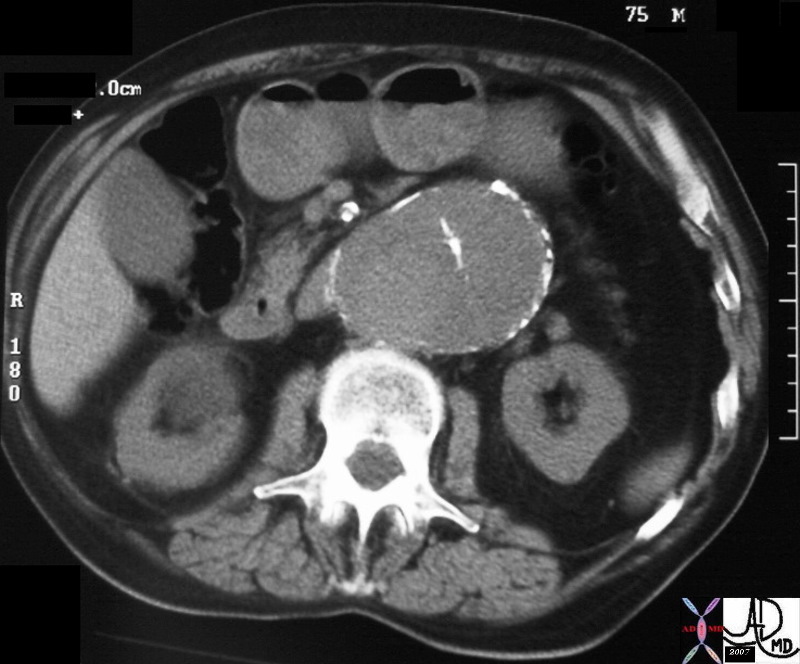
Chronic Aortic Dissection
hx 75 male with abdominal pain abdomren abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 31262
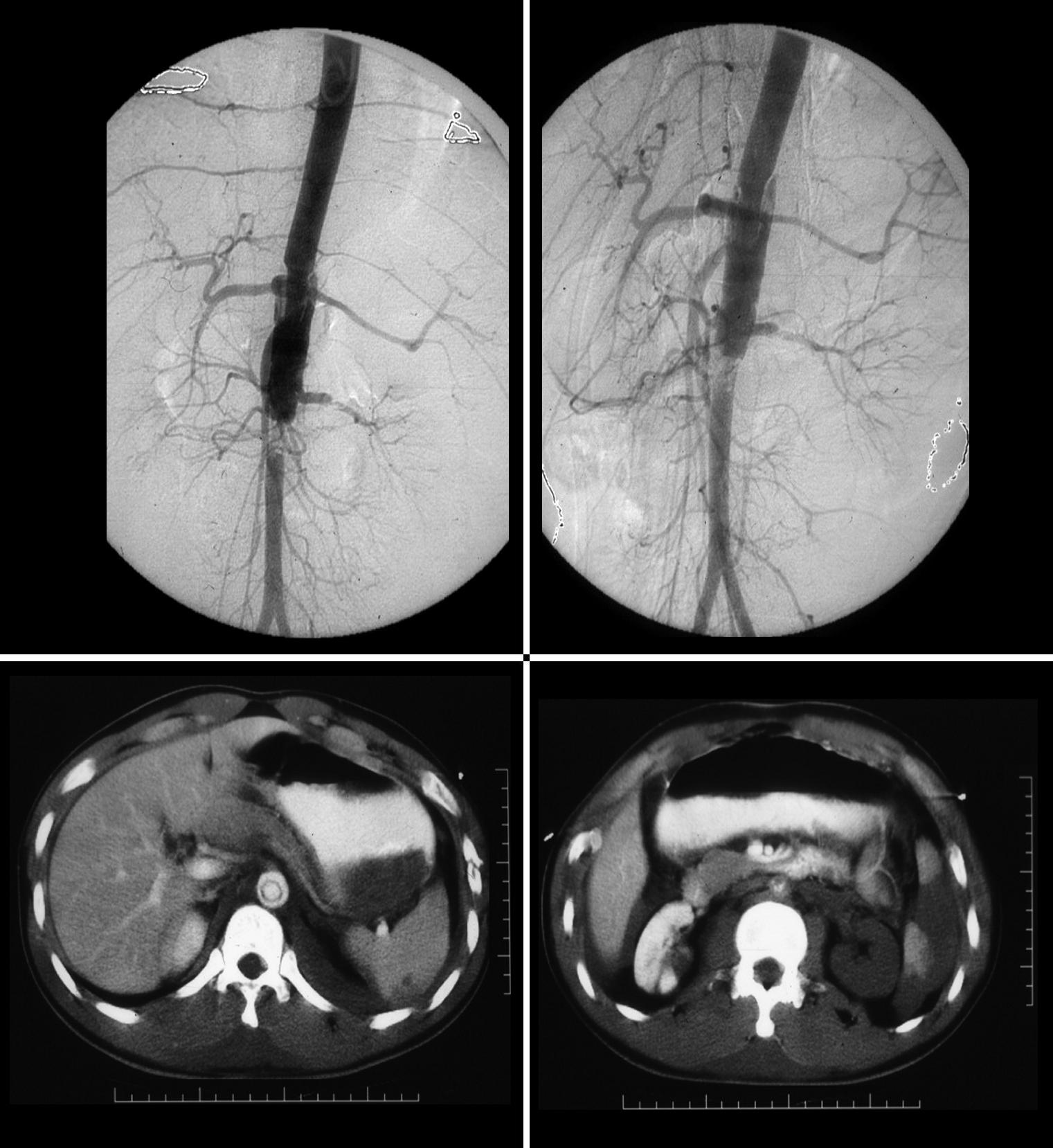
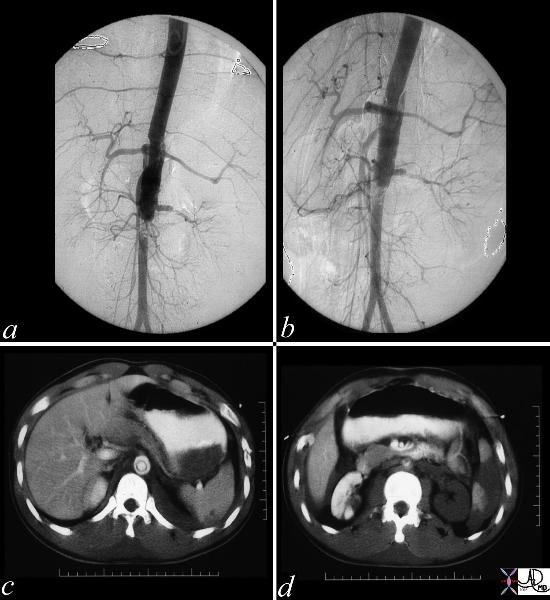
Acute Traumatic Dissection
These images represent a traumatic dissection of the abdominal aorta caused by a compression injury to the abdomen. The angiograms in a and b shows what appears to be a complex tear of the aorta with a dissection and then a subtotal obstruction of the aorta distally. The CTscan shows (c) thedissection to better effect, with a subtotal narrowing of the aorta distally. Not also the injury of the left renal artery on the angiogram as well as the lack of perfusion of the left kidney on the CT scan.
The clinical presentation is usually dramatic with hyperacute “shearing” or “ripping “chest or back pain. Proximal Anterior chest pain is usually associated with tears of the ascending aorta, while dissection of the descending aorta usually gives interscapular pain. Most patients are hypertensive. Findings on examination include aortic insufficiency (50%), pulse deficits (50% – commonly involve the brachiocephalic vessels) or neurologic manifestations Distal dissections may reveal pulse deficits of the left subclavian or femoral vessels
Diagnostic Tools
The radiologic diagnosis is often suspected on the plain film with the widened mediastinum and more specifically a blunted aortic knob or thickening of the wall of the knob more than 5 mm past the calcified aortic intima (Ring sign). CT, MRI and trans-esophageal echocardiography are all used with high sensitivity and specificity. TEE sensitivity/specificity of 99/98% Aortic angiography is an invasive procedure but may be best at delineating the extent of dissection
Dissection Involving the Ascending and Descending Aorta
descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20448
Dissection Involving the Ascending and Descending Aorta
The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The patient presented with classsical sever chest pain that radiated to the back. The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
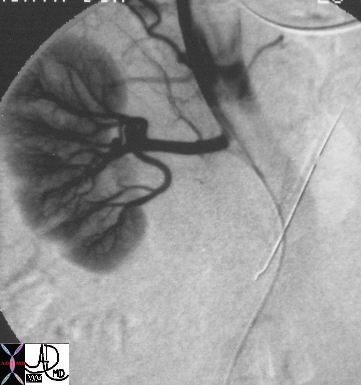
Spontaneous Dissection and Rupture of the Hepatic Artery 50 year old male presents with abdominal pain to the ER liver left hepatic artery fx focal aneurysmal dilatation of the proximal left hepatic artery fx focal narrowing of the mid portion at site of dissection dx spontaneous dissection of the left hepatic artery complicated by intraperitoneal rupture., treated by coil embolisation The common and right hepatic artery arose from the SMA Copyright 2012 Courtesy Ashley Davidoff MD 45278b
Links and References
McMahon M et al Review of Aortic Dissection Radiographics 2010 Murillo H et al Aortic Dissection and other Acute Aortic Syndromes Radiographics 2021
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Type B dissection involving descending thoracic and abdominal aorta
thorax abdomen fx dissection true lumen false lumen occluded renal artery angiogram angiography
Copyright 2012 Courtesy Ashley Davidoff MD 24588b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Type B dissection involving descending thoracic and abdominal aorta
thorax abdomen fx dissection true lumen false lumen occluded renal artery angiogram angiography
Copyright 2012 Courtesy Ashley Davidoff MD 24588b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Type B dissection involving descending thoracic and abdominal aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Type B dissection involving descending thoracic and abdominal aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The patient presented with classsical sever chest pain that radiated to the back. The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
Copyright 2012 Courtesy Ashley Davidoff MD 20448c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The patient presented with classsical sever chest pain that radiated to the back. The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
Copyright 2012 Courtesy Ashley Davidoff MD 20448c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The patient presented with classsical sever chest pain that radiated to the back. The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
Copyright 2012 Courtesy Ashley Davidoff MD 20448c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The patient presented with classsical sever chest pain that radiated to the back. The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
Copyright 2012 Courtesy Ashley Davidoff MD 20448c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20448
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20448
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20448
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20448
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Dissection Involving the Ascending and Descending Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Dissection Involving the Ascending and Descending Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Traumatic Dissection
These images represent a traumatic dissection of the abdominal aorta caused by a compression injury to the abdomen. The angiograms in a and b shows what appears to be a complex tear of the aorta with a dissection and then a subtotal obstruction of the aorta distally. The CTscan shows (c) thedissection to better effect, with a subtotal narrowing of the aorta distally. Not also the injury of the left renal artery on the angiogram as well as the lack of perfusion of the left kidney on the CT scan.
Copyright 2012 Courtesy Ashley Davidoff MD. 14734c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Traumatic Dissection
These images represent a traumatic dissection of the abdominal aorta caused by a compression injury to the abdomen. The angiograms in a and b shows what appears to be a complex tear of the aorta with a dissection and then a subtotal obstruction of the aorta distally. The CTscan shows (c) thedissection to better effect, with a subtotal narrowing of the aorta distally. Not also the injury of the left renal artery on the angiogram as well as the lack of perfusion of the left kidney on the CT scan.
Copyright 2012 Courtesy Ashley Davidoff MD. 14734c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
These images represent a traumatic dissection of the abdominal aorta caused by a compression injury to the abdomen. The angiograms in a and b shows what appears to be a complex tear of the aorta with a dissection and then a subtotal obstruction of the aorta distally. The CTscan shows (c) thedissection to better effect, with a subtotal narrowing of the aorta distally. Not also the injury of the left renal artery on the angiogram as well as the lack of perfusion of the left kidney on the CT scan.
Copyright 2012 Courtesy Ashley Davidoff MD. 14734c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
These images represent a traumatic dissection of the abdominal aorta caused by a compression injury to the abdomen. The angiograms in a and b shows what appears to be a complex tear of the aorta with a dissection and then a subtotal obstruction of the aorta distally. The CTscan shows (c) thedissection to better effect, with a subtotal narrowing of the aorta distally. Not also the injury of the left renal artery on the angiogram as well as the lack of perfusion of the left kidney on the CT scan.
Copyright 2012 Courtesy Ashley Davidoff MD. 14734c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Traumatic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Traumatic Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Chronic Aortic Dissection
hx 75 male with abdominal pain abdomren abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 31262
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Chronic Aortic Dissection
hx 75 male with abdominal pain abdomren abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 31262
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
hx 75 male with abdominal pain abdomren abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 31262
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
hx 75 male with abdominal pain abdomren abdominal AAA aneurysm fx mural calcification thrombosed aortic dissection chronic dissection CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 31262
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Chronic Aortic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Chronic Aortic Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Type B Dissection
The thoracic angiogram reveals an aortic dissection which starts just after the left subclaian artery. The true lumen is the narrowed medial lumen which is denser than the larger lateral false lumen. (a,b) In (c) the A-P view reveals a patent proximal abdominal aorta, but the distal narrowing and occlusion of the the left iliac artery suggests that the dissection has progressed distally. In the image 35124c the cross sectional images of the abdominal aorta reveal that the true lumen of the distal aorta is in fact quite narrowed.
Courtesy Laura Feldman MD. 35116c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Type B Dissection
The thoracic angiogram reveals an aortic dissection which starts just after the left subclaian artery. The true lumen is the narrowed medial lumen which is denser than the larger lateral false lumen. (a,b) In (c) the A-P view reveals a patent proximal abdominal aorta, but the distal narrowing and occlusion of the the left iliac artery suggests that the dissection has progressed distally. In the image 35124c the cross sectional images of the abdominal aorta reveal that the true lumen of the distal aorta is in fact quite narrowed.
Courtesy Laura Feldman MD. 35116c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The thoracic angiogram reveals an aortic dissection which starts just after the left subclaian artery. The true lumen is the narrowed medial lumen which is denser than the larger lateral false lumen. (a,b) In (c) the A-P view reveals a patent proximal abdominal aorta, but the distal narrowing and occlusion of the the left iliac artery suggests that the dissection has progressed distally. In the image 35124c the cross sectional images of the abdominal aorta reveal that the true lumen of the distal aorta is in fact quite narrowed.
Courtesy Laura Feldman MD. 35116c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The thoracic angiogram reveals an aortic dissection which starts just after the left subclaian artery. The true lumen is the narrowed medial lumen which is denser than the larger lateral false lumen. (a,b) In (c) the A-P view reveals a patent proximal abdominal aorta, but the distal narrowing and occlusion of the the left iliac artery suggests that the dissection has progressed distally. In the image 35124c the cross sectional images of the abdominal aorta reveal that the true lumen of the distal aorta is in fact quite narrowed.
Courtesy Laura Feldman MD. 35116c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Type B Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Type B Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
True Lumen Compressed on Left
Slow Flow in False Lumen
abdomen artery + abdominal aorta + fx crescentic crescent shaped false lumen fx dissection + dx iatrogenic + imaging radiology CTscan radiologists and detectives
Copyright 2012 Courtesy Ashley DAvidoff MD 19408
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
True Lumen Compressed on Left
Slow Flow in False Lumen
abdomen artery + abdominal aorta + fx crescentic crescent shaped false lumen fx dissection + dx iatrogenic + imaging radiology CTscan radiologists and detectives
Copyright 2012 Courtesy Ashley DAvidoff MD 19408
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
abdomen artery + abdominal aorta + fx crescentic crescent shaped false lumen fx dissection + dx iatrogenic + imaging radiology CTscan radiologists and detectives
Copyright 2012 Courtesy Ashley DAvidoff MD 19408
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
abdomen artery + abdominal aorta + fx crescentic crescent shaped false lumen fx dissection + dx iatrogenic + imaging radiology CTscan radiologists and detectives
Copyright 2012 Courtesy Ashley DAvidoff MD 19408
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
True Lumen Compressed on Left
Slow Flow in False Lumen
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
True Lumen Compressed on Left
Slow Flow in False Lumen
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
True Lumen Compressed and Supplying Right Renal Artery
artery aorta fx dissection dx dissection angiography
Copyright 2012 Courtesy Ashley Davidoff MD 17474
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
True Lumen Compressed and Supplying Right Renal Artery
artery aorta fx dissection dx dissection angiography
Copyright 2012 Courtesy Ashley Davidoff MD 17474
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
artery aorta fx dissection dx dissection angiography
Copyright 2012 Courtesy Ashley Davidoff MD 17474
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
artery aorta fx dissection dx dissection angiography
Copyright 2012 Courtesy Ashley Davidoff MD 17474
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
True Lumen Compressed and Supplying Right Renal Artery
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
True Lumen Compressed and Supplying Right Renal Artery
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Dissection Caused by Ulcerating Plaque Complicated by Mural Hematoma
This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease.
Copyright 2012 Courtesy Ashley Davidoff MD. 19416c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Dissection Caused by Ulcerating Plaque Complicated by Mural Hematoma
This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease.
Copyright 2012 Courtesy Ashley Davidoff MD. 19416c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease.
Copyright 2012 Courtesy Ashley Davidoff MD. 19416c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease.
Copyright 2012 Courtesy Ashley Davidoff MD. 19416c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Dissection Caused by Ulcerating Plaque Complicated by Mural Hematoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Dissection Caused by Ulcerating Plaque Complicated by Mural Hematoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Atelectasis Masquerading as a Dissection
This series of CT scans from the arch to the abdominal inlet shows a curvilinear density around the aorta on its left lateral edge that masquerades as a dissection The last three images (g,h,i) and their magnified counterparts below them (j,k,l) shows air bronchograms opacified vessels within the crescentic density, and deviation from the contour of the aorta, confirming the atelectatic nature of the crescent.
Copyright 2012 Courtesy Ashley Davidoff MD 37071c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Atelectasis Masquerading as a Dissection
This series of CT scans from the arch to the abdominal inlet shows a curvilinear density around the aorta on its left lateral edge that masquerades as a dissection The last three images (g,h,i) and their magnified counterparts below them (j,k,l) shows air bronchograms opacified vessels within the crescentic density, and deviation from the contour of the aorta, confirming the atelectatic nature of the crescent.
Copyright 2012 Courtesy Ashley Davidoff MD 37071c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This series of CT scans from the arch to the abdominal inlet shows a curvilinear density around the aorta on its left lateral edge that masquerades as a dissection The last three images (g,h,i) and their magnified counterparts below them (j,k,l) shows air bronchograms opacified vessels within the crescentic density, and deviation from the contour of the aorta, confirming the atelectatic nature of the crescent.
Copyright 2012 Courtesy Ashley Davidoff MD 37071c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This series of CT scans from the arch to the abdominal inlet shows a curvilinear density around the aorta on its left lateral edge that masquerades as a dissection The last three images (g,h,i) and their magnified counterparts below them (j,k,l) shows air bronchograms opacified vessels within the crescentic density, and deviation from the contour of the aorta, confirming the atelectatic nature of the crescent.
Copyright 2012 Courtesy Ashley Davidoff MD 37071c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Atelectasis Masquerading as a Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Atelectasis Masquerading as a Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Color Flow Doppler – Descending Thoracic Aorta Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Color Flow Doppler – Descending Thoracic Aorta Dissection
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Doppler US of the descending thoracic aorta showing flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Color Flow Doppler – Descending Thoracic Aorta Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Color Flow Doppler – Descending Thoracic Aorta Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection.
Courtesy Philips Medical Systems 33167
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Thoracic Aorta – Dissection
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection.
Courtesy Philips Medical Systems 33167
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection.
Courtesy Philips Medical Systems 33167
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Gray scale US of the descending thoracic aorta showing a hypoechoic true lumen (black) and homogeneous echoes of the thrombosed lumen in this patient with aortic dissection.
Courtesy Philips Medical Systems 33167
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Thoracic Aorta – Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Thoracic Aorta – Dissection
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
36865c
This series of CT scans were taken 1 day apart. The patient presented with chest pain and the soft tissue changes around contrast filled aorta (a,b,c) suggested a chronic dissection, or an acute thrombosed dissection. 1 day later the non-contrast CT clearly reveals an acute thrombosed dissection (d,e,f) that started in the arch and extended along the descending thoracic aorta. The last series (g,h,i) enhance the non contrats study. A non contrast CT followed by contrast injection, is an important tchnique to optimally characterise acute changes in this clincal setting.
Copyright 2012 Courtesy Ashley Davidoff MD 36865c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
36865c
This series of CT scans were taken 1 day apart. The patient presented with chest pain and the soft tissue changes around contrast filled aorta (a,b,c) suggested a chronic dissection, or an acute thrombosed dissection. 1 day later the non-contrast CT clearly reveals an acute thrombosed dissection (d,e,f) that started in the arch and extended along the descending thoracic aorta. The last series (g,h,i) enhance the non contrats study. A non contrast CT followed by contrast injection, is an important tchnique to optimally characterise acute changes in this clincal setting.
Copyright 2012 Courtesy Ashley Davidoff MD 36865c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This series of CT scans were taken 1 day apart. The patient presented with chest pain and the soft tissue changes around contrast filled aorta (a,b,c) suggested a chronic dissection, or an acute thrombosed dissection. 1 day later the non-contrast CT clearly reveals an acute thrombosed dissection (d,e,f) that started in the arch and extended along the descending thoracic aorta. The last series (g,h,i) enhance the non contrats study. A non contrast CT followed by contrast injection, is an important tchnique to optimally characterise acute changes in this clincal setting.
Copyright 2012 Courtesy Ashley Davidoff MD 36865c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This series of CT scans were taken 1 day apart. The patient presented with chest pain and the soft tissue changes around contrast filled aorta (a,b,c) suggested a chronic dissection, or an acute thrombosed dissection. 1 day later the non-contrast CT clearly reveals an acute thrombosed dissection (d,e,f) that started in the arch and extended along the descending thoracic aorta. The last series (g,h,i) enhance the non contrats study. A non contrast CT followed by contrast injection, is an important tchnique to optimally characterise acute changes in this clincal setting.
Copyright 2012 Courtesy Ashley Davidoff MD 36865c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
36865c
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
36865c
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Arch Dissection – Narrowed True Lumen
thorax thoracic aorta arch aorta fx dissection dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20449
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Arch Dissection – Narrowed True Lumen
thorax thoracic aorta arch aorta fx dissection dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20449
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
thorax thoracic aorta arch aorta fx dissection dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20449
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
thorax thoracic aorta arch aorta fx dissection dx aortic dissection type A CTscan
Copyright 2012 Courtesy Ashley Davidoff MD 20449
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Arch Dissection – Narrowed True Lumen
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Arch Dissection – Narrowed True Lumen
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Type A Aortic Dissection
This combination of images from a CTscan through the thorax, reveals an aortic dissection starting at the level of the aortic valve and extending into the abdomen with involvement of the celiac axis. The true lumen is overlaid in pink while the false lumen is overlaid in a darker red. The green structure is the intimal flap. Flow in the false lumen is slightly delayed and slower as seen by the lower density of the contrasyt within it.
Copyright 2012 Courtesy Ashley Davidoff MD. 19412c02 code CVS artery AO aorta dissection fx crescent
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Type A Aortic Dissection
This combination of images from a CTscan through the thorax, reveals an aortic dissection starting at the level of the aortic valve and extending into the abdomen with involvement of the celiac axis. The true lumen is overlaid in pink while the false lumen is overlaid in a darker red. The green structure is the intimal flap. Flow in the false lumen is slightly delayed and slower as seen by the lower density of the contrasyt within it.
Copyright 2012 Courtesy Ashley Davidoff MD. 19412c02 code CVS artery AO aorta dissection fx crescent
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This combination of images from a CTscan through the thorax, reveals an aortic dissection starting at the level of the aortic valve and extending into the abdomen with involvement of the celiac axis. The true lumen is overlaid in pink while the false lumen is overlaid in a darker red. The green structure is the intimal flap. Flow in the false lumen is slightly delayed and slower as seen by the lower density of the contrasyt within it.
Copyright 2012 Courtesy Ashley Davidoff MD. 19412c02 code CVS artery AO aorta dissection fx crescent
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This combination of images from a CTscan through the thorax, reveals an aortic dissection starting at the level of the aortic valve and extending into the abdomen with involvement of the celiac axis. The true lumen is overlaid in pink while the false lumen is overlaid in a darker red. The green structure is the intimal flap. Flow in the false lumen is slightly delayed and slower as seen by the lower density of the contrasyt within it.
Copyright 2012 Courtesy Ashley Davidoff MD. 19412c02 code CVS artery AO aorta dissection fx crescent
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Type A Aortic Dissection
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Type A Aortic Dissection
)

{kind=link}
{kind=link}